








Tratamiento de tumores de células germinales del sistema nervioso central
Find state-of-the-art care for germ cell tumors of the central nervous system at Montefiore Einstein Comprehensive Cancer Center at the Children's Hospital at Montefiore Einstein (CHAM). We focus on creating a supportive, nurturing environment for patients and their families.
The childhood cancer team at CHAM conduct groundbreaking research and offer the most up-to-date treatments, including radiation therapy and, when necessary, chemotherapy and surgery. They’re committed to improving outcomes for central nervous system germ cell tumors and all types of cancer by providing access to the latest treatments available through clinical trials.
Si lo que usted desea es lo mejor para su hijo, acuda a los especialistas del Centro Oncológico Integral Montefiore Einstein en CHAM, quienes se dedican con pasión a erradicar el cáncer y a atender todas las necesidades de salud de su hijo.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Childhood Central Nervous System Germ Cell Tumors Treatment (PDQ®)–Patient Version
General Information About Childhood Central Nervous System (CNS) Germ Cell Tumors
Puntos clave
- Childhood central nervous system (CNS) germ cell tumors form from germ cells.
- There are different types of childhood CNS germ cell tumors.
- Germinomas
- Nongerminomas
- Teratomas
- Signs and symptoms of childhood CNS germ cell tumors include unusual thirst, frequent urination, or vision changes.
- Imaging studies and other tests are used to help diagnose childhood CNS germ cell tumors.
- A biopsy may be done to be sure of the diagnosis of a CNS germ cell tumor.
- Hay ciertos factores que afectan al pronóstico (la probabilidad de recuperación).
Childhood central nervous system (CNS) germ cell tumors form from germ cells.
Germ cells are the reproductive cells in a fetus. These cells later become sperm in the testicles or unfertilized eggs in the ovaries. Sometimes the germ cells travel to or from other parts of the fetus as it develops and later become germ cell tumors. Most germ cell tumors form in the testes or ovaries. Germ cell tumors that form in the brain or spinal cord are called CNS (central nervous system) germ cell tumors.
CNS germ cell tumors occur most often in young people aged 10 to 19 years. They are more common in males than in females. In older children, CNS germ cell tumors usually form in the brain near the pineal gland and in an area of the brain that includes the pituitary gland and the tissue just above it. Sometimes germ cell tumors form in other areas of the brain.
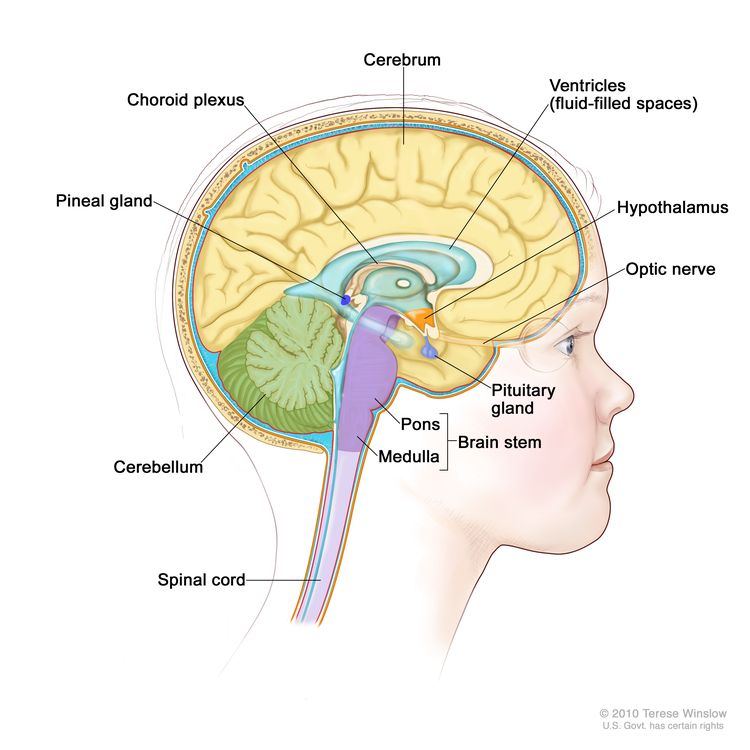
Anatomy of the inside of the brain, showing the pineal and pituitary glands, optic nerve, ventricles (with cerebrospinal fluid shown in blue), and other parts of the brain.
The cause of most childhood CNS germ cell tumors is not known.
This summary is about germ cell tumors that start in the central nervous system (brain and spinal cord). Germ cell tumors may also form in other parts of the body. For information on germ cell tumors that are extracranial (outside the brain), see Childhood Extracranial Germ Cell Tumors Treatment.
Treatment of CNS germ cell tumors may be different for children and adults. For information about treatment for adults, see the following PDQ summaries:
There are different types of childhood CNS germ cell tumors.
Different types of CNS germ cell tumors can form from the germ cells that later become sperm or unfertilized eggs. The type of CNS germ cell tumor that is diagnosed depends on what the cells look like under a microscope and results of laboratory tests that check tumor marker levels.
This summary is about the treatment of several types of CNS germ cell tumors.
Germinomas
Germinomas are the most common type of CNS germ cell tumor and have a good prognosis. Tumor marker levels are not used to diagnose germinomas.
Nongerminomas
Some nongerminomas make hormones, such as alpha-fetoprotein (AFP) and beta-human chorionic gonadotropin (beta-hCG). Types of nongerminomas include:
- Embryonal carcinomas make the hormone AFP.
- Yolk sac tumors make the hormone AFP.
- Choriocarcinomas make the hormone beta-hCG.
- Mixed germ cell tumors are made of more than one kind of germ cell. They may make AFP and beta-hCG.
Teratomas
CNS teratomas are described as mature or immature, based on how normal the cells look under a microscope. Mature teratomas look almost like normal cells under a microscope and are made of different kinds of tissue, such as hair, muscle, and bone. Immature teratomas look very different from normal cells under a microscope and are made of cells that look like fetal cells. Some immature teratomas are a mix of mature and immature cells. Tumor marker levels are not used to diagnose teratomas.
Signs and symptoms of childhood CNS germ cell tumors include unusual thirst, frequent urination, or vision changes.
- Where the tumor has formed.
- The size of the tumor.
- Whether the tumor or the body make too much of certain hormones.
Signs and symptoms may be caused by childhood CNS germ cell tumors or by other conditions. Check with your child's doctor if your child has:
- Excess thirst.
- Large amounts of urine that is clear or almost clear.
- Frequent urination.
- Bed-wetting or frequent urination at night.
- Trouble moving the eyes or seeing clearly.
- Double vision.
- Loss of appetite.
- Pérdida de peso sin causa aparente
- Early puberty.
- Headaches.
- Nausea and vomiting.
- Feeling very tired.
- Problems with schoolwork.
Imaging studies and other tests are used to help diagnose childhood CNS germ cell tumors.
In addition to asking about your child's personal and family health history and doing a physical exam, your child's doctor may perform the following tests and procedures:
- Neurological exam: A series of questions and tests to check the brain, spinal cord, and nerve function. The exam checks a person's mental status, coordination, and ability to walk normally, and how well the muscles, reflexes, and senses work. This may also be called a neuro exam or a neurologic exam.
- Visual field exam: An exam to check a person's field of vision (the total area in which objects can be seen). This test measures both central vision (how much a person can see when looking straight ahead) and peripheral vision (how much a person can see in all other directions while staring straight ahead). The eyes are tested one at a time. The eye not being tested is covered.
- MRI (magnetic resonance imaging) with and without gadolinium: A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the brain and spinal cord. A substance called gadolinium is injected into a vein. The gadolinium may collect around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- Punción lumbar: procedimiento utilizado para recolectar líquido cefalorraquídeo (LCR) de la columna vertebral. Esto se hace colocando una aguja entre dos huesos de la columna vertebral and into the lining around the spinal cord to remove a sample of the CSF. The sample of CSF is checked under a microscope for signs of tumor cells and tested for tumor markers. The amount of proteína y glucose in the sample may also be tested. This procedure is also called an LP or spinal tap.
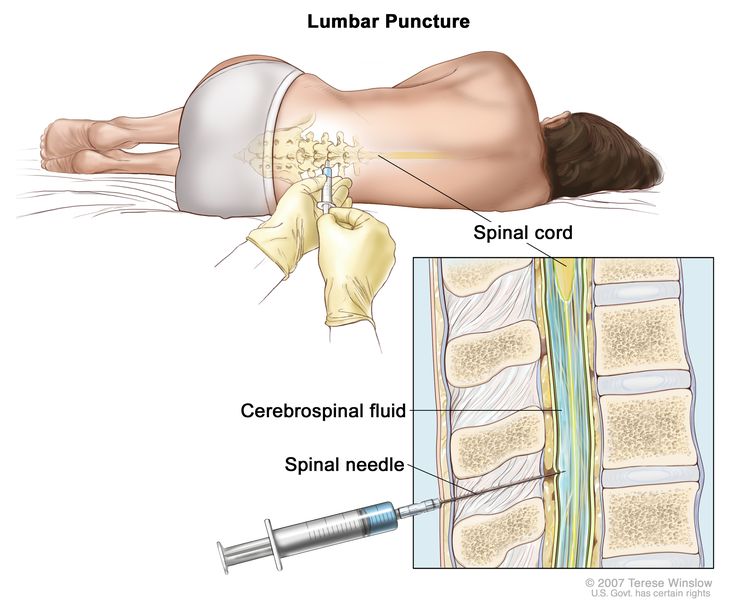
Punción lumbar. El paciente se recuesta en una camilla. Tras adormecer una pequeña zona de la parte baja de la espalda, se inserta una aguja espinal (una aguja larga y delgada) en la parte inferior de la columna vertebral para extraer líquido cefalorraquídeo (LCR, mostrado en azul). El líquido puede enviarse a un laboratorio para su análisis.
- Tumor marker tests: procedimiento en el que se toma una muestra de sangre or cerebrospinal fluid (CSF) is checked to measure the amounts of certain substances released into the blood or CSF normally by organs and tissues, or at abnormally high levels by tumor cells in the body. Certain substances are linked to specific types of cancer when found at increased levels in the blood or CSF. These are called tumor markers.
The following tumor markers are used to diagnose some CNS germ cell tumors:
- Alfafetoproteína (AFP)
- Gonadotropina coriónica humana beta (beta-hCG)
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher- or lower-than-normal) amount of a substance can be a sign of disease.
- Blood hormone studies: A procedure in which a blood sample is checked to measure the amounts of certain hormones released into the blood by organs and tissues in the body. An unusual (higher- or lower-than-normal) amount of a substance can be a sign of disease in the organ or tissue that makes it. The blood will be checked for the levels of hormones made by the pituitary gland and other glands.
A biopsy may be done to be sure of the diagnosis of a CNS germ cell tumor.
If doctors think your child may have a CNS germ cell tumor, a biopsy may be done. For brain tumors, the biopsy can be done by removing part of the skull or making a small hole in the skull and using a needle or surgical device to remove a sample of tissue. Sometimes, when a needle is used, it is guided by a computer to remove the tissue sample. A pathologist views the tissue under a microscope to look for cancer cells. If cancer cells are found, the doctor may remove as much tumor as safely possible during the same surgery. The piece of skull is usually put back in place after the procedure.
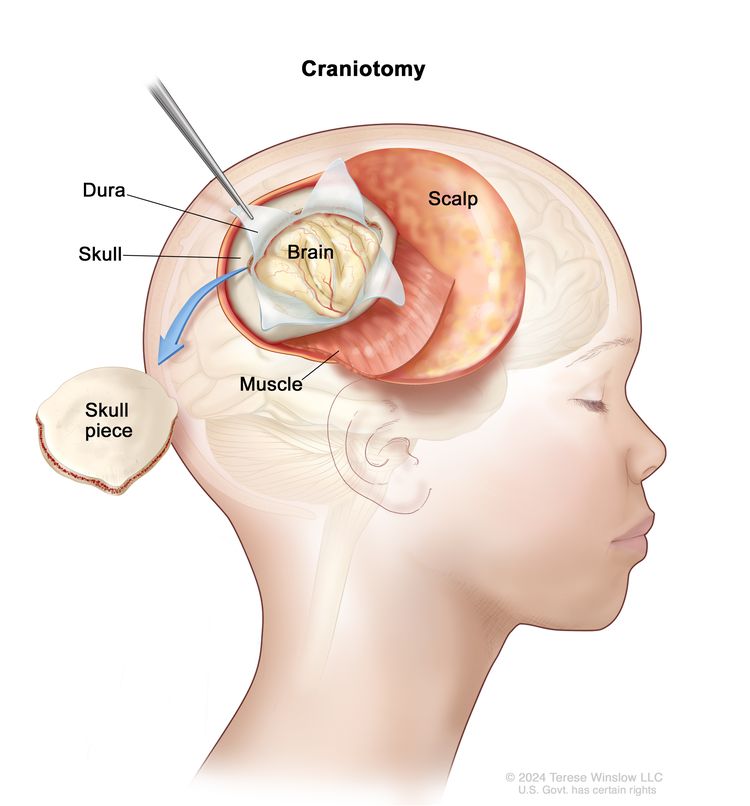
Craniotomy. An opening is made in the skull and a piece of the skull is removed to show part of the brain.
The following test may be done on the sample of tissue that is removed:
- Immunohistochemistry: A laboratory test that uses antibodies to check for certain antigens (markers) in a sample of a patient's tissue. The antibodies are usually linked to an enzyme or a fluorescent dye. After the antibodies bind to a specific antigen in the tissue sample, the enzyme or dye is activated, and the antigen can then be seen under a microscope. This type of test is used to help diagnose cancer and to help tell one type of cancer from another type of cancer.
Sometimes the diagnosis can be made based on the results of imaging and tumor marker tests and a biopsy is not needed.
Hay ciertos factores que afectan al pronóstico (la probabilidad de recuperación).
El pronóstico depende de:
- The type of germ cell tumor.
- The type and level of any tumor markers.
- Where the tumor is in the brain or in the spinal cord.
- Whether the cancer has spread within the brain and spinal cord or to other parts of the body.
- Whether the tumor is newly diagnosed or has recurred (come back) after treatment.
Stages of Childhood CNS Germ Cell Tumors
Puntos clave
- Childhood central nervous system (CNS) germ cell tumors rarely spread outside of the brain and spinal cord.
- Sometimes childhood central nervous system germ cell tumors come back after treatment.
Childhood central nervous system (CNS) germ cell tumors rarely spread outside of the brain and spinal cord.
The process used to find out how much cancer there is and whether the cancer has spread is called staging. There is no standard staging system for childhood central nervous system (CNS) germ cell tumors.
The treatment plan depends on:
- The type of germ cell tumor.
- Whether the tumor has spread within the brain and spinal cord or to other parts of the body, such as the lung or bone.
- The results of tests and procedures done to diagnose childhood CNS germ cell tumors.
- Whether the tumor is newly diagnosed or has recurred (come back) after treatment.
Sometimes childhood central nervous system germ cell tumors come back after treatment.
The tumors usually recur (come back) where they first formed. The tumors may also come back in other places and/or in the meninges (thin layers of tissue that cover and protect the brain and spinal cord).
Descripción general de las opciones de tratamiento
Puntos clave
- There are different types of treatment for children with central nervous system (CNS) germ cell tumors.
- Children with CNS germ cell tumors should have their treatment planned by a team of health care providers who are experts in treating cancer in children.
- Se utilizan los siguientes tipos de tratamiento:
- Radioterapia
- Quimioterapia
- Cirugía
- Quimioterapia de dosis alta con rescate de células madre
- Se están probando nuevos tipos de tratamiento en ensayos clínicos.
- Treatment for childhood CNS germ cell tumors may cause side effects.
- Los pacientes pueden evaluar la posibilidad de participar en un ensayo clínico.
- Los pacientes pueden participar en ensayos clínicos antes, durante o después de comenzar el tratamiento contra el cáncer.
- Follow-up care may be needed.
There are different types of treatment for children with central nervous system (CNS) germ cell tumors.
Different types of treatment are available for children with central nervous system (CNS) germ cell tumors. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for people with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment.
Dado que el cáncer infantil es poco frecuente, debe considerarse la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Children with CNS germ cell tumors should have their treatment planned by a team of health care providers who are experts in treating cancer in children.
Treatment will be overseen by a pediatric oncologist and/or a radiation oncologist. A pediatric oncologist is a doctor who specializes in treating children with cancer. A radiation oncologist specializes in treating cancer with radiation therapy. These doctors work with other pediatric health care providers who are experts in treating children with CNS germ cell tumors and who specialize in certain areas of medicine. These may include the following specialists:
Se utilizan los siguientes tipos de tratamiento:
Radioterapia
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing.
External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer. Certain ways of giving radiation therapy can help keep radiation from damaging nearby healthy tissue. This type of radiation therapy may include:
- Stereotactic radiosurgery: Stereotactic radiosurgery is a type of external radiation therapy. A rigid head frame is attached to the skull to keep the head still during the radiation treatment. A machine aims a single large dose of radiation directly at the tumor. This procedure does not involve surgery. It is also called stereotaxic radiosurgery, radiosurgery, and radiation surgery.
Radiation therapy to the brain can affect growth and development in young children. Certain ways of giving radiation therapy can lessen the damage to healthy brain tissue. For children younger than 3 years, chemotherapy may be given instead. This can delay or reduce the need for radiation therapy.
Quimioterapia
La quimioterapia es un tratamiento contra el cáncer que utiliza medicamentos para detener el crecimiento de las células cancerosas, ya sea destruyéndolas o impidiendo su división. Cuando la quimioterapia se administra por vía oral o se inyecta en una vena o músculo, los medicamentos entran en el torrente sanguíneo y pueden llegar a las células cancerosas de todo el cuerpo (quimioterapia sistémica).
Cirugía
Whether surgery to remove the tumor can be done depends on where the tumor is in the brain. Surgery to remove the tumor may cause severe, long-term side effects.
Surgery may be done to remove teratomas and may be used for germ cell tumors that come back. After the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given chemotherapy or radiation therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
Quimioterapia de dosis alta con rescate de células madre
High doses of chemotherapy are given to kill cancer cells. Healthy cells, including blood-forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient and are frozen and stored. After the patient completes chemotherapy, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
Se están probando nuevos tipos de tratamiento en ensayos clínicos.
La información sobre los ensayos clínicos está disponible en el sitio web del NCI.
Treatment for childhood CNS germ cell tumors may cause side effects.
Para obtener más información sobre los efectos secundarios que aparecen durante el tratamiento del cáncer, consulte la sección Efectos secundarios.
Side effects from cancer treatment that begin after treatment and continue for months or years are called late effects. Late effects of cancer treatment may include:
- Physical problems, including:
- Problemas de la vista
- Endocrine problems, such as diabetes insipidus.
- Blood vessel problems, such as stroke.
- Cambios en el estado de ánimo, los sentimientos, el pensamiento, el aprendizaje o la memoria
- Segundos cánceres (nuevos tipos de cáncer)
Some late effects may be treated or controlled. Talk with your child's doctors about the possible late effects caused by some treatments. Learn more at Late Effects of Treatment for Childhood Cancer.
Los pacientes pueden evaluar la posibilidad de participar en un ensayo clínico.
Para algunos pacientes, participar en un ensayo clínico puede ser la mejor opción de tratamiento. Los ensayos clínicos son parte del proceso de investigación del cáncer y se realizan para determinar si los nuevos tratamientos para el cáncer son seguros y eficaces o mejores que el tratamiento estándar.
Muchos de los tratamientos estándar actuales para el cáncer se basan en ensayos clínicos anteriores. Los pacientes que participan en un ensayo clínico pueden recibir el tratamiento estándar o ser de los primeros en recibir uno nuevo.
Los pacientes que participan en ensayos clínicos también ayudan a mejorar la forma en que se tratará el cáncer en el futuro. Incluso cuando los ensayos clínicos no conducen a nuevos tratamientos efectivos, suelen responder a preguntas clave y contribuir de forma significativa al avance de la investigación.
Los pacientes pueden participar en ensayos clínicos antes, durante o después de comenzar el tratamiento contra el cáncer.
Algunos ensayos clínicos solo incluyen a pacientes que aún no han recibido tratamiento. Otros ensayos prueban tratamientos para pacientes cuyo cáncer no ha mejorado. También hay ensayos clínicos que prueban nuevas formas de evitar que el cáncer recidive (regrese) o de reducir los efectos secundarios del tratamiento del cáncer.
Se están realizando ensayos clínicos en muchas partes del país. Puede encontrar información sobre los ensayos clínicos respaldados por el NCI en el sitio web de búsqueda de ensayos clínicos del NCI. Puede encontrar ensayos clínicos respaldados por otras organizaciones en el sitio web ClinicalTrials.gov.
Follow-up care may be needed.
As your child goes through treatment, they will have follow-up tests or check-ups. Some of the tests that were done to diagnose the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Algunas de las pruebas se seguirán realizando periódicamente después de que finalice el tratamiento. Los resultados de estas pruebas pueden mostrar si la afección de su hijo o hija ha cambiado o si el cáncer ha recidivado (regresado).
Children whose cancer affected their pituitary gland when the cancer was diagnosed will usually need to have their blood hormone levels checked. If the blood hormone level is low, replacement hormone medicine is given.
Children who had a high tumor marker level (alpha-fetoprotein or beta-human chorionic gonadotropin) when the cancer was diagnosed usually need to have their blood tumor marker level checked. If the tumor marker level increases after initial treatment, the tumor may have recurred.
Treatment of Childhood CNS Germinomas
Para más información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
Treatment of newly diagnosed central nervous system (CNS) germinomas may include:
- Chemotherapy followed by radiation therapy.
- Radiation therapy to the whole brain including the ventricles (fluid-filled spaces of the brain) and spinal cord. A higher dose of radiation is given to the tumor than the area around the tumor.
- Radiation therapy to the ventricles and the tumor.
Treatment of Childhood CNS Nongerminomas
Para más información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
It is not clear what treatment is best for newly diagnosed central nervous system (CNS) nongerminomas.
Treatment of choriocarcinoma, embryonal carcinoma, yolk sac tumor, or mixed germ cell tumor may include:
- Chemotherapy followed by radiation therapy.
- Cirugía. If a mass remains after chemotherapy that continues to grow and tumor marker levels are normal (called growing teratoma syndrome), Cirugía may be needed to check if the mass is part teratoma, fibrosis, or a growing tumor.
- If the mass is a mature teratoma or fibrosis, radiation therapy is given.
- If the mass is a growing tumor, other treatments may be given.
- A clinical trial of chemotherapy with radiation therapy to treat patients with CNS nongerminomas that have not spread.
Treatment of Childhood CNS Teratomas
Para más información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
Treatment of newly diagnosed mature and immature central nervous system (CNS) teratomas may include:
Treatment of Recurrent Childhood CNS Germ Cell Tumors
Treatment of recurrent childhood central nervous system (CNS) germ cell tumors may include:
- Chemotherapy followed by radiation therapy, for germinomas.
- High-dose chemotherapy with stem cell rescue using the patient's stem cells, with or without more radiation therapy, for germinomas and nongerminomas.
Current Clinical Trials
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
To Learn More About Childhood CNS Germ Cell Tumors
For more information about childhood central nervous system germ cell tumors, see:
Para obtener más información sobre el cáncer infantil y otros recursos generales sobre el cáncer, consulte los siguientes sitios web:
- El cáncer
- Cánceres infantiles
- CureSearch para el cáncer infantil
- Efectos tardíos del tratamiento del cáncer infantil
- Adolescentes y adultos jóvenes con cáncer
- Niños con cáncer: una guía para padres
- El cáncer en los niños y los adolescentes
- Estadificación del cáncer
- Cómo hacer frente al cáncer
- Preguntas para el médico sobre el cáncer
- Para supervivientes, cuidadores e intercesores
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
This PDQ cancer information summary has current information about the treatment of childhood central nervous system germ cell tumors. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
La información de este resumen para pacientes procede de la versión para profesionales de la salud, la cual es revisada y actualizada periódicamente por el comité editorial del PDQ sobre el tratamiento pediátrico según sea necesario.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
PDQ® Pediatric Treatment Editorial Board. PDQ Childhood Central Nervous System Germ Cell Tumors Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/brain/patient/child-cns-germ-cell-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389502]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Updated:
Source URL: https://www.cancer.gov/node/212044/syndication
Agencia de origen: National Cancer Institute (NCI)
Captured Date: 2013-09-14 09:06:11.0