








Tratamiento de tumores embrionarios del sistema nervioso central
Si a su hijo le han diagnosticado un tumor embrionario del sistema nervioso central, encontrará atención integral y compasiva en el Centro Oncológico Integral Montefiore Einstein del Hospital Infantil Montefiore Einstein (CHAM) . Nuestro equipo ofrece un entorno de apoyo y cuidado para bebés y niños pequeños afectados por estos tumores y sus familias.
Disponemos de las terapias más avanzadas y actualizadas, junto con nuevos tratamientos prometedores desarrollados mediante investigaciones y ensayos clínicos innovadores. Estos estudios se basan en los datos científicos más recientes y son ofrecidos a través de consorcios reconocidos internacionalmente, como el Children's Oncology Group y la National Pediatric Cancer Foundation.
Contamos con un equipo de especialistas dedicado a cada paciente con el que trabajamos. Este equipo incluye oncólogos pediátricos, cirujanos oncólogos, enfermeros especializadas en oncología, oncólogos radiólogos, radiólogos de diagnóstico, patólogos, psiquiatras, psicólogos, fisioterapeutas y terapeutas ocupacionales, además de trabajadores sociales y especialistas en vida infantil, entre otros. Juntos, crean un entorno afectuoso y enriquecedor para que usted y su hijo o hija se sientan lo más cómodos posible durante el proceso de atención.
Si lo que usted desea es lo mejor para su hijo, acuda a los especialistas del Centro Oncológico Integral Montefiore Einstein en CHAM, quienes se dedican con pasión a erradicar el cáncer y a atender todas las necesidades de salud de su hijo.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Tratamiento del meduloblastoma y otros tumores embrionarios infantiles del sistema nervioso central (PDQ®): versión para pacientes
Información general sobre el meduloblastoma y otros tumores embrionarios del sistema nervioso central infantil
Puntos clave
- El meduloblastoma y otros tumores embrionarios del sistema nervioso central (SNC) pueden comenzar en las células embrionarias (fetales) que permanecen en el cerebro después del nacimiento.
- Hay diferentes tipos de tumores embrionarios del SNC.
- El pineoblastoma se forma en las células de la glándula pineal.
- Ciertas alteraciones genéticas aumentan el riesgo de meduloblastoma infantil.
- Se puede realizar asesoramiento genético para niños con meduloblastoma o pineoblastoma.
- Los síntomas del meduloblastoma, otros tumores embrionarios del SNC y el pineoblastoma dependen de la edad del niño y de la ubicación del tumor.
- Las pruebas que examinan el cerebro y la médula espinal se utilizan para diagnosticar meduloblastoma infantil, otros tumores embrionarios del SNC y pineoblastoma.
- Se puede hacer una biopsia para confirmar el diagnóstico.
- Hay ciertos factores que afectan al pronóstico (probabilidad de recuperación) y a las opciones de tratamiento.
- Es posible que desee obtener una segunda opinión.
El meduloblastoma y otros tumores embrionarios del sistema nervioso central (SNC) pueden comenzar en las células embrionarias (fetales) que permanecen en el cerebro después del nacimiento.
El meduloblastoma es un tumor de rápido crecimiento que se forma en el cerebelo (la parte inferior y posterior del cerebro). El meduloblastoma es el tipo más común de tumor embrionario del SNC. Los tumores embrionarios del SNC son crecimientos incontrolados de células en el cerebro. Estos tumores se forman en células que quedan del desarrollo fetal, llamadas células embrionarias. El pineoblastoma es un tipo de tumor cerebral de rápido crecimiento que se forma en o alrededor de un órgano diminuto cerca del centro del cerebro llamado glándula pineal.
Estos tumores pueden ser benignos (no cancerosos) o malignos (cancerosos). Los tumores cerebrales benignos crecen y presionan áreas cercanas del cerebro, pero rara vez se diseminan a otras partes del cerebro. Es probable que los tumores cerebrales malignos crezcan rápidamente y se propaguen a otras partes del cerebro. También pueden propagarse a otras partes del cuerpo, pero eso es menos común. Cuando un tumor crece y presiona un área del cerebro o se propaga a otras partes del cerebro, puede impedir que esa parte del cerebro funcione como debería. Tanto los tumores cerebrales benignos como los malignos pueden causar signos o síntomas graves y necesitan tratamiento.
La mayoría de los meduloblastomas, otros tumores embrionarios del SNC y los pineoblastomas en niños son malignos. Estos tumores tienden a diseminarse a través del líquido cefalorraquídeo a otras partes del cerebro y a la médula espinal.
Aunque el cáncer es poco frecuente en los niños, los tumores cerebrales son el segundo tipo más común de cáncer infantil, después de la leucemia. Este resumen trata sobre el tratamiento de los tumores cerebrales primarios (tumores que comienzan en el cerebro).
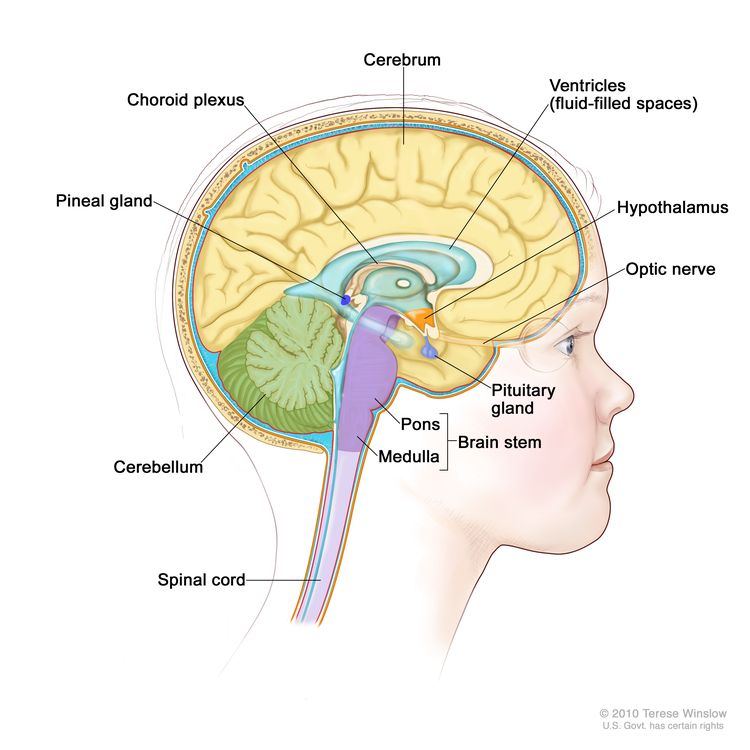
Anatomía del interior del encéfalo que muestra la glándula pineal y la hipófisis, el nervio óptico, los ventrículos (el líquido cefalorraquídeo se ve en color azul) y otras partes del encéfalo.
Hay diferentes tipos de tumores embrionarios del SNC.
Los diferentes tipos de tumores embrionarios del SNC pueden ser:
- Meduloblastomas
La mayoría de los tumores embrionarios del SNC son meduloblastomas, tumores de rápido crecimiento que se forman en las células cerebrales del cerebelo. El cerebelo está ubicado en la parte inferior trasera del cerebro, entre el cerebro y el tronco del encéfalo, y se encarga de controlar el movimiento, el equilibrio y la postura. Es raro que los meduloblastomas se propaguen a los huesos, la médula ósea, los pulmones u otras partes del cuerpo.
- Otros tipos de tumores embrionarios del SNC (no meduloblastoma)
Los tumores embrionarios del SNC, distintos al meduloblastoma, son de rápido crecimiento y pueden formarse en las células cerebrales en cualquier parte del sistema nervioso central, incluido el cerebro, el tronco encefálico o la médula espinal. El cerebro se encuentra en la parte superior de la cabeza y es su estructura más grande. Además, controla funciones como el pensamiento, el aprendizaje, la resolución de problemas, las emociones, el habla, la lectura, la escritura y el movimiento voluntario. Es poco común que estos tumores se diseminen a los huesos, la médula ósea, los pulmones u otras partes del cuerpo.
Hay muchos tipos de tumores embrionarios (no meduloblastomas) del SNC:
- Tumores neuroepiteliales cribiformes
El tumor neuroepitelial cribiforme se desarrolla en los ventrículos del cerebro, y se da con mayor frecuencia en bebés y niños pequeños. El tumor neuroepitelial cribiforme aparece con mayor frecuencia en niños varones.
- Tumores embrionarios con rosetas multicapa
Los tumores embrionarios con rosetas multicapa (ETMR) son tumores raros que aparecen en el cerebro y la médula espinal. Los ETMR se dan con mayor frecuencia en niños pequeños y son tumores de rápido crecimiento.
- Neuroblastomas del SNC
Los neuroblastomas del SNC son un tipo muy raro de neuroblastoma que se forma en el tejido nervioso del cerebro o en las capas de tejido que cubren el cerebro y la médula espinal. Estos tumores pueden alcanzar un gran tamaño y propagarse a otras regiones del cerebro o la médula espinal.
- Tumor neuroepitelial de alto grado del SNC con un cambio en el gen BCOR
El tumor neuroepitelial de alto grado del SNC es un tumor muy raro que se forma en el cerebro. Es más frecuente en niños menores de 10 años, aunque también puede manifestarse en niños mayores y adolescentes.
- Sarcoma de Ewing del SNC con un cambio en el gen CIC
El sarcoma de Ewing del SNC es un tumor muy raro que aparece en el cerebro o en la columna vertebral, afectando principalmente a niños menores de 10 años.
- Tumor neuroepitelial de alto grado del SNC con un cambio en el gen MN1
El tumor neuroepitelial de alto grado del SNC es un tumor muy raro que se forma en el cerebro o la médula espinal. Este tumor se da con mayor frecuencia en adolescentes y mujeres.
- Meduloepiteliomas
El meduloepitelioma es un tumor de rápido crecimiento que generalmente se forma en el cerebro, la médula espinal o los nervios cercanos a la columna vertebral. Se presenta con mayor frecuencia en bebés y niños pequeños.
- Tumor embrionario del sistema nervioso central con cambios en el gen PLAGL
El tumor embrionario del sistema nervioso central con alteraciones del gen PLAGL es un tumor muy poco frecuente que se forma en el cerebro y afecta tanto a niños como a adultos.
- Tumores neuroepiteliales cribiformes
El tumor teratoide rabdoide atípico del sistema nervioso central también es un tipo de tumor embrionario, pero su tratamiento difiere del de otros tumores embrionarios del sistema nervioso central infantil. Obtenga más información en Tratamiento del tumor teratoide rabdoide atípico del sistema nervioso central infantil.
El pineoblastoma se forma en las células de la glándula pineal.
La glándula pineal es un órgano diminuto en el centro del cerebro. La glándula produce melatonina, una sustancia que ayuda a controlar nuestro ciclo de sueño. Los pineoblastomas suelen ser tumores malignos de rápido crecimiento con células que se ven muy diferentes de las células normales de la glándula pineal. Los pineoblastomas no son un tipo de tumor embrionario del SNC, pero su tratamiento es similar al tratamiento de los tumores embrionarios del SNC.
El pineoblastoma está asociado con cambios hereditarios en el gen del retinoblastoma (RB1). Los niños con la forma hereditaria de retinoblastoma (cáncer que se forma en los tejidos de la retina) tienen un mayor riesgo de desarrollar pineoblastoma. Cuando el retinoblastoma aparece simultáneamente con un tumor en la glándula pineal o cerca de ella, se le conoce como retinoblastoma trilateral. Las pruebas de resonancia magnética (MRI) en niños con retinoblastoma pueden detectar el pineoblastoma en una etapa temprana, cuando aún es posible tratarlo con éxito. Es poco común que el pineoblastoma se disemine a los huesos, la médula ósea, los pulmones u otras partes del cuerpo.
Ciertas alteraciones genéticas aumentan el riesgo de meduloblastoma infantil.
El meduloblastoma infantil se debe a ciertos cambios en el funcionamiento de las células cerebrales, especialmente en la forma en que crecen y se dividen para generar nuevas células. A menudo, la causa exacta de estos cambios celulares es desconocida. Más información sobre cómo se desarrolla el cáncer en la sección ¿Qué es el cáncer?
Un factor de riesgo es cualquier elemento que aumenta la probabilidad de desarrollar una enfermedad. No todos los niños que tienen uno o más factores de riesgo desarrollarán meduloblastoma, y algunos niños pueden padecerlo sin tener un factor de riesgo conocido.
El riesgo de meduloblastoma se incrementa en personas que tienen alguna de las siguientes enfermedades hereditarias:
- Síndrome de Turcot
- Síndrome de Rubinstein-Taybi
- Síndrome de carcinoma nevoide de células basales (Gorlin)
- Síndrome de Li-Fraumeni
- Anemia de Fanconi
Hable con el médico de su hijo si cree que su hijo puede estar en riesgo.
Se puede realizar asesoramiento genético para niños con meduloblastoma o pineoblastoma.
Es posible que el historial médico familiar no dé la información suficiente para determinar si un niño con un tumor cerebral tiene una afección hereditaria que incrementa su riesgo. Los asesores genéticos y otros profesionales de la salud especialmente capacitados pueden analizar el diagnóstico de su hijo o hija, y el historial médico de la familia para comprender:
- Las opciones de pruebas genéticas para los genes ELP1, APC, SUFU, PTCH1, TP53, PALB2, o BRCA2, en caso de meduloblastoma.
- Las opciones de pruebas genéticas para el gen RB1 o DICER1, en caso de pineoblastoma.
- El riesgo de que su hijo o hija desarrolle otro tipo de cáncer.
- El riesgo de de que los hermanos de su hijo o hija desarrollen cáncer.
- Los riesgos y beneficios de conocer su información genética.
Los asesores genéticos también pueden ayudarle a afrontar los resultados de las pruebas genéticas de su hijo o hija, incluido cómo comunicarlos a los miembros de la familia.
Obtenga más información sobre las pruebas genéticas para detectar el riesgo de cáncer hereditario .
Los síntomas del meduloblastoma, otros tumores embrionarios del SNC y el pineoblastoma dependen de la edad del niño y de la ubicación del tumor.
Es posible que los niños no presenten síntomas de meduloblastoma, otros tumores embrionarios del sistema nervioso central o pineoblastoma hasta que el tumor haya crecido. Es importante consultar con el médico de su hijo si su hijo presenta:
- Pérdida del equilibrio, dificultad para caminar, falta de coordinación o habla lenta
- Dolor de cabeza, especialmente por la mañana, o cefalea que desaparece después de vomitar.
- Debilidad general
- Parálisis o debilidad en un lado de la cara
- Somnolencia inusual o cambios en los niveles de energía
- Convulsiones
- Visión doble u otros problemas oculares
- Náuseas y vómitos
Los bebés y niños pequeños con estos tumores pueden estar irritables o experimentar un crecimiento lento. Además, pueden presentar dificultades para alimentarse y no alcanzar hitos del desarrollo como sentarse, caminar y hablar en oraciones. Estos tumores también pueden causar un aumento en el tamaño de la cabeza de un bebé.
Estos síntomas pueden deberse a problemas distintos del meduloblastoma, otros tumores embrionarios del sistema nervioso central o el pineoblastoma. La única forma de saberlo es que su hijo o hija acuda al médico.
Las pruebas que examinan el cerebro y la médula espinal se utilizan para diagnosticar meduloblastoma infantil, otros tumores embrionarios del SNC y pineoblastoma.
Si su hijo o hija tiene síntomas que sugieren meduloblastoma, otro tipo de tumor embrionario del sistema nervioso central o pineoblastoma, el médico deberá averiguar si se deben a cáncer u otro problema. Le preguntará sobre el historial de salud personal y familiar de su hijo o hija, y le realizará un reconocimiento físico. Según los resultados, es posible que le recomiende otras pruebas. Si a su hijo o hija le diagnostican meduloblastoma, otro tipo de tumor embrionario del sistema nervioso central o pineoblastoma, los resultados de estas pruebas le ayudarán a usted y al médico o pediatra a planificar el tratamiento.
Las pruebas utilizadas para diagnosticar el meduloblastoma, otros tumores embrionarios del SNC y el pineoblastoma pueden consistir en:
- La resonancia magnética (RM) del cerebro y la médula espinal con gadolinio es un procedimiento que utiliza un imán, ondas de radio y una computadora para generar una serie de imágenes detalladas de áreas dentro del cerebro y la médula espinal. Se inyecta una sustancia llamada gadolinio en una vena. El gadolinio se acumula alrededor de las células cancerosas, haciéndolas más brillantes en la imagen. Este procedimiento también se denomina resonancia magnética nuclear (RMN). En ocasiones, se realiza una espectroscopia por resonancia magnética (ERM) durante la misma RM para observar la composición química del tejido cerebral.
- La tomografía computarizada (TC) utiliza una computadora conectada a una máquina de rayos X para crear una serie de imágenes detalladas del interior del cuerpo desde diferentes ángulos. Se puede inyectar un tinte en una vena o ingerirlo para ayudar a que los órganos o tejidos se vean con más claridad. Este procedimiento también se denomina tomografía axial computarizada o exploración por TAC. Más información sobre las tomografías computarizadas (TC) y el cáncer.
- Punción lumbar es un procedimiento que se utiliza para recolectar líquido cefalorraquídeo (LCR) de la columna vertebral. Esto se hace colocando una aguja entre dos huesos de la columna vertebral y dentro del revestimiento que rodea la médula espinal para extraer una muestra de LCR. La muestra de LCR se examina bajo un microscopio para detectar signos de células tumorales. La muestra también puede analizarse para determinar la cantidad de proteína y glucosa. Una cantidad de proteína por encima de lo normal o una concentración de glucosa por debajo de lo esperado pueden indicar la presencia de un tumor. Este procedimiento también se conoce como PL o punción espinal.
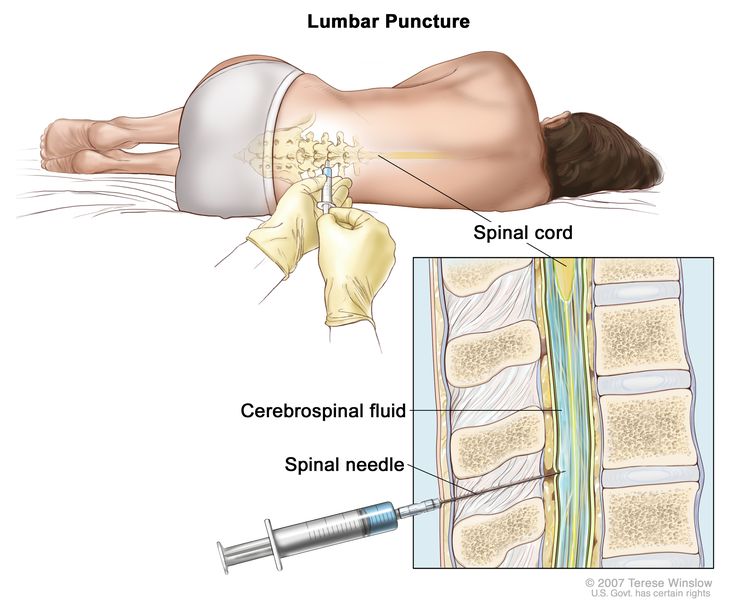
Punción lumbar. El paciente se recuesta en una camilla. Tras adormecer una pequeña zona de la parte baja de la espalda, se inserta una aguja espinal (una aguja larga y delgada) en la parte inferior de la columna vertebral para extraer líquido cefalorraquídeo (LCR, mostrado en azul). El líquido puede enviarse a un laboratorio para su análisis.
Se puede hacer una biopsia para confirmar el diagnóstico.
Si los médicos creen que su hijo o hija puede tener meduloblastoma, otro tipo de tumor embrionario del SNC o pineoblastoma, se puede realizar una biopsia. La biopsia se realiza extirpando parte del cráneo y usando una aguja para extraer una muestra de tejido. A veces, se utiliza una aguja guiada por computadora para extraer la muestra de tejido. Un patólogo observa el tejido bajo un microscopio para buscar células cancerosas. Si se encuentran células cancerosas, el médico puede extirpar la mayor cantidad de tumor posible de manera segura durante la misma cirugía. Por lo general, el trozo de cráneo se vuelve a colocar en su lugar después del procedimiento.
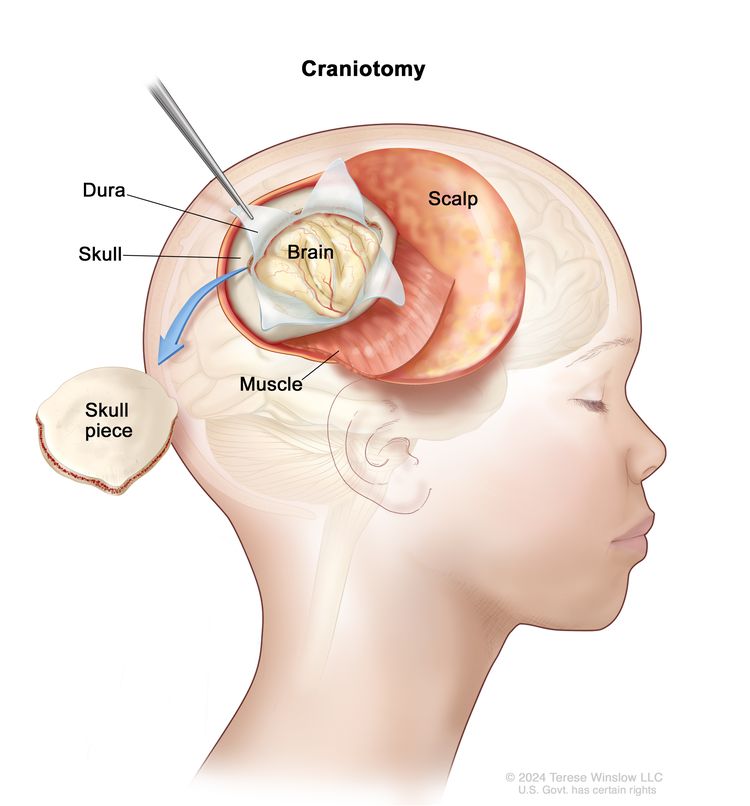
Craneotomía. Se practica una abertura en el cráneo y se extrae una parte del cráneo para mostrar parte del cerebro.
Se pueden realizar las siguientes pruebas en la muestra de tejido que se extrae:
- La inmunohistoquímica es una prueba de laboratorio que emplea anticuerpos para identificar determinados antígenos (marcadores) en una muestra de tejido de un paciente. Los anticuerpos suelen estar ligados a una enzima o a un colorante fluorescente. Una vez que los anticuerpos se unen a un antígeno específico en la muestra de tejido, la enzima o el colorante se activan, lo que permite visualizar el antígeno con un microscopio. Este tipo de prueba se utiliza para diagnosticar el cáncer y diferenciar distintos tipos de cáncer.
- Las pruebas moleculares analizan la presencia de determinados genes, proteínas u otras moléculas en muestras de tejido, sangre o médula ósea. También permiten detectar cambios específicos en un gen o cromosoma que pueden influir en el desarrollo de meduloblastoma, otros tumores embrionarios o pineoblastoma. Estas pruebas pueden utilizarse para planificar el tratamiento, evaluar su efectividad o establecer un pronóstico. Los niños con meduloblastoma, otros tumores embrionarios o pineoblastoma podrían ser candidatos para pruebas moleculares a través de la Iniciativa de Caracterización Molecular.
La Iniciativa de Caracterización Molecular ofrece pruebas moleculares gratuitas a niños, adolescentes y adultos jóvenes con ciertos tipos de cáncer recién diagnosticados. El programa se imparte a través de la Iniciativa de Datos sobre Cáncer Infantil del NCI. Para más información, visite el sitio Acerca de la Iniciativa de Caracterización Molecular.
Hay ciertos factores que afectan al pronóstico (probabilidad de recuperación) y a las opciones de tratamiento.
Si a su hijo o hija le han diagnosticado meduloblastoma, otro tumor embrionario del sistema nervioso central o pineoblastoma, es natural que tenga preguntas sobre la gravedad del cáncer y las posibilidades de supervivencia. El resultado o curso probable de una enfermedad se conoce como pronóstico.
El pronóstico y las opciones de tratamiento dependen de:
- El tipo de tumor y su ubicación en el cerebro
- Si el cáncer se ha propagado dentro del cerebro y la médula espinal en el momento del diagnóstico
- La edad del niño cuando se encuentra el tumor
- Cuánto queda del tumor después de la cirugía
- Si hay ciertos cambios en los cromosomas, genes o células cerebrales
- Si el tumor acaba de ser diagnosticado o ha reaparecido (regresado)
No hay dos personas iguales y la respuesta al tratamiento puede variar considerablemente. El equipo de atención médica del cáncer de su hijo o hija es el más indicado para hablar con usted sobre el pronóstico.
Es posible que desee obtener una segunda opinión.
Es posible que desee obtener una segunda opinión para confirmar el diagnóstico y el plan de tratamiento de su hijo hija. Si busca una segunda opinión, deberá reunir los resultados de pruebas médicas importantes y los informes del primer médico para compartirlos con el segundo especialista. Este segundo médico revisará los resultados de las pruebas genéticas, el informe patológico, las diapositivas y las exploraciones. Podrá confirmar el diagnóstico inicial, sugerir modificaciones en el plan de tratamiento o dar información adicional sobre el tumor de su hijo o hija.
Para obtener más información sobre cómo elegir un médico y obtener una segunda opinión, consulte Búsqueda de tratamiento para el cáncer. Puede comunicarse con el Servicio de Información de Cáncer del NCI por chat, correo electrónico o teléfono (tanto en inglés como en español) para obtener ayuda para encontrar un médico, un hospital o una segunda opinión. Si tiene alguna pregunta que desee hacer en las citas de su hijo o hija, consulte Preguntas para el médico sobre el cáncer.
Estadificación del meduloblastoma y otros tumores embrionarios del sistema nervioso central infantil, y pineoblastoma
Puntos clave
- El meduloblastoma, otros tumores embrionarios del SNC y el pineoblastoma en niños se tratan según el tipo de tumor y la edad del paciente.
- El tratamiento del meduloblastoma en niños mayores de 3 años también depende de si el tumor es de riesgo promedio o alto.
- Riesgo promedio
- Riesgo alto
- Los resultados de pruebas y procedimientos realizados para diagnosticar meduloblastoma, otros tumores embrionarios del SNC y pineoblastoma en niños se emplean para planificar el tratamiento del cáncer.
- A veces, el meduloblastoma y otros tumores embrionarios del sistema nervioso central infantil pueden reaparecer después del tratamiento.
El meduloblastoma, otros tumores embrionarios del SNC y el pineoblastoma en niños se tratan según el tipo de tumor y la edad del paciente.
El estadio del cáncer describe su extensión en el cuerpo, incluyendo el tamaño del tumor, si se ha propagado y qué tan lejos ha llegado desde su lugar de origen. No existe un sistema de estadificación específico para el meduloblastoma infantil, otros tumores embrionarios del sistema nervioso central (SNC) o el pineoblastoma, pero las pruebas y procedimientos utilizados para diagnosticar el cáncer también ayudan a planificar el tratamiento.
El tratamiento de otros tumores embrionarios del SNC y del pineoblastoma en niños se basa en la edad del paciente. Los niños de 3 años o menos pueden recibir un tratamiento diferente al de los niños mayores de 3 años.
El tratamiento del meduloblastoma en niños mayores de 3 años también depende de si el tumor es de riesgo promedio o alto.
Riesgo promedio
Los meduloblastomas se denominan de riesgo promedio cuando se cumplen todas las condiciones siguientes:
- El tumor se ha extirpado completamente mediante cirugía o solo ha quedado una cantidad muy pequeña.
- El cáncer no se ha propagado a otras partes del cuerpo.
Riesgo alto
Los meduloblastomas se denominan de alto riesgo si se cumple alguna de las siguientes condiciones:
- Parte del tumor no se ha extirpado mediante cirugía.
- El cáncer se ha propagado a otras partes del cerebro, la médula espinal o el cuerpo.
En general, es más probable que el cáncer recurra (regrese) después del tratamiento en pacientes con un tumor de alto riesgo.
Los resultados de pruebas y procedimientos realizados para diagnosticar meduloblastoma, otros tumores embrionarios del SNC y pineoblastoma en niños se emplean para planificar el tratamiento del cáncer.
Si a su hijo o hija le diagnostican meduloblastoma, otro tipo de tumor embrionario del sistema nervioso central (SNC) o pineoblastoma, lo derivarán a un oncólogo pediátrico o neurooncólogo, que es un médico que se especializa en la estadificación y el tratamiento de cánceres infantiles. Recomendará pruebas para determinar la extensión (estadio) del cáncer. Algunas de las pruebas que se utilizan para diagnosticar el cáncer se repiten después de la cirugía. Esto es para averiguar cuánto tumor queda después de la cirugía y para ver si el cáncer se ha propagado desde el cerebro a la columna vertebral u otras partes del cuerpo. Es importante saber si el cáncer se ha propagado para planificar el mejor tratamiento. Más información sobre las pruebas de diagnóstico en la sección Información general.
Se pueden usar las siguientes pruebas para determinar si el cáncer se ha propagado más allá del cerebro y la médula espinal:
- Biopsia y aspiración de la médula ósea son procedimientos en los que se extrae una muestra de médula ósea y hueso del hueso de la cadera o esternón utilizando una aguja especial. Un patólogo ve la muestra bajo un microscopio para buscar signos de cáncer. La aspiración y la biopsia de la médula ósea solo se realizan cuando hay signos de que el cáncer se ha propagado a la médula ósea.
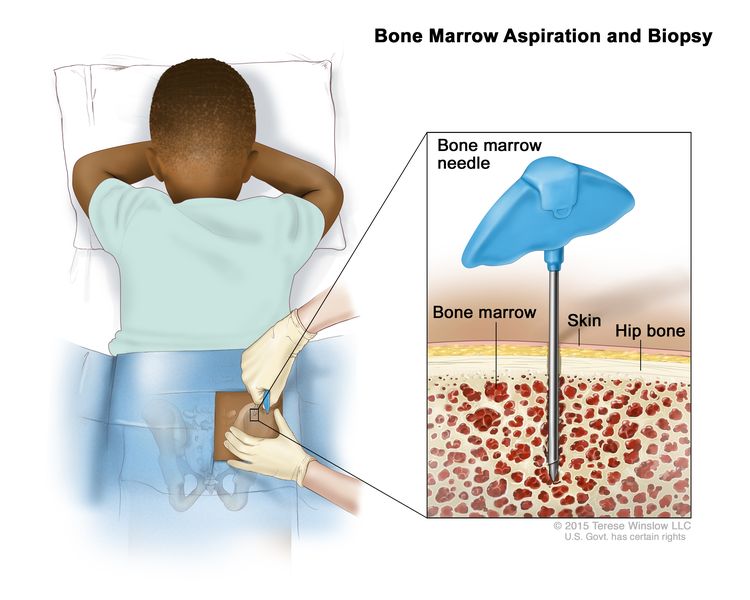
Aspiración y biopsia de médula ósea: tras anestesiar una pequeña zona de la piel, se introduce una aguja para médula ósea en el hueso de la cadera del niño. Se extraen muestras de sangre, hueso y médula ósea para examinarlas con un microscopio.
- La gammagrafía ósea es un procedimiento para verificar si hay células que se dividen rápidamente, como células cancerosas, en el hueso. Se inyecta una cantidad muy pequeña de material radiactivo en una vena y viaja a través del torrente sanguíneo. El material radiactivo se acumula en los huesos con cáncer y se detecta mediante un escáner. Una gammagrafía ósea solo se realiza cuando hay signos o síntomas de que el cáncer se ha propagado al hueso.
A veces, el meduloblastoma y otros tumores embrionarios del sistema nervioso central infantil pueden reaparecer después del tratamiento.
El meduloblastoma y otros tipos de tumores embrionarios del SNC infantil suelen recidivar (regresar) dentro de los tres años posteriores al tratamiento, aunque también pueden reaparecer muchos años después. El meduloblastoma recidivante y otros tumores embrionarios del SNC infantil pueden reaparecer en el mismo sitio del tumor original y/o en una ubicación diferente dentro del cerebro o la médula espinal.
Descripción general de las opciones de tratamiento
Puntos clave
- Existen diferentes tipos de tratamiento para los niños que tienen meduloblastoma y otros tumores embrionarios del sistema nervioso central (SNC).
- Los niños con meduloblastoma, otros tumores embrionarios del SNC y pineoblastoma deben recibir un tratamiento planificado por un equipo de especialistas en tumores cerebrales pediátricos.
- Pueden emplearse los siguientes tipos de tratamiento:
- Cirugía
- Radioterapia
- Quimioterapia
- Quimioterapia de dosis alta con rescate de células madre autólogas
- Terapia dirigida
- Se están probando nuevos tipos de tratamiento en ensayos clínicos.
Existen diferentes tipos de tratamiento para los niños que tienen meduloblastoma y otros tumores embrionarios del sistema nervioso central (SNC).
Existen diferentes tipos de tratamiento para niños y adolescentes con meduloblastoma, otros tipos de tumores embrionarios del sistema nervioso central o pineoblastoma. Usted y el equipo de atención médica del cáncer de su hijo o hija trabajarán juntos para decidir el tratamiento. Se tendrán en cuenta muchos factores, como la salud general del menor y si el tumor es un diagnóstico reciente o si ha reaparecido.
Los niños con meduloblastoma, otros tumores embrionarios del SNC y pineoblastoma deben recibir un tratamiento planificado por un equipo de especialistas en tumores cerebrales pediátricos.
El oncólogo pediátrico, un médico que se especializa en el tratamiento de niños con cáncer, supervisa el tratamiento del meduloblastoma, otros tumores embrionarios del sistema nervioso central y el pineoblastoma. El oncólogo pediátrico trabaja con otros proveedores de atención médica que son expertos en el tratamiento de tumores cerebrales, cada uno con conocimientos específicos en diferentes áreas de la medicina. El equipo también puede incluir a otros profesionales, como:
- Pediatra
- Neurocirujano
- Neurólogo
- Neuropatólogo
- Neurorradiólogo
- Especialista en rehabilitación
- Oncólogo radioterapeuta
- Psicólogo
El plan de tratamiento de su hijo o hija incluirá información sobre el cáncer, los objetivos terapéuticos, las opciones disponibles y los posibles efectos secundarios. Es recomendable hablar con el equipo médico antes de que comience el tratamiento para conocer qué esperar en cada etapa. Para obtener ayuda en cada paso del proceso, consulte nuestro folleto descargable Niños con cáncer: una guía para padres.
Pueden emplearse los siguientes tipos de tratamiento:
Cirugía
La cirugía se utiliza para diagnosticar y tratar el meduloblastoma, otros tumores embrionarios del SNC infantil y el pineoblastoma, como se describe en la sección Información general de este resumen.
Después de que el médico haya extirpado todo el cáncer que se puede observar en el momento de la cirugía, es posible que algunos pacientes reciban quimioterapia, radioterapia o ambas para destruir las células cancerosas que queden. El tratamiento administrado después de la cirugía, para reducir el riesgo de que el cáncer regrese, se llama terapia adyuvante.
Radioterapia
La radioterapia utiliza rayos X de alta energía u otros tipos de radiación para matar las células cancerosas o evitar que crezcan. El meduloblastoma, otros tumores embrionarios del SNC o el pineoblastoma en niños pueden tratarse con radioterapia de haz externo. La radioterapia de haz externo utiliza una máquina fuera del cuerpo para enviar radiación hacia el área del cuerpo con cáncer.
Hay ciertas formas de administrar radioterapia externa que pueden ayudar a evitar que la radiación dañe el tejido sano circundante. Estos tipos de radioterapia incluyen:
- La radioterapia conformada emplea una computadora para generar una imagen tridimensional (3D) del tumor, permitiendo moldear los haces de radiación para que se adapten a su forma. Esto facilita que una dosis alta de radiación alcance el tumor con mayor precisión, minimizando el daño al tejido sano circundante.
- La radioterapia estereotáxica dirige la radiación directamente al tumor, minimizando el daño al tejido sano circundante. La dosis total de radiación se divide en varias aplicaciones más pequeñas administradas a lo largo de varios días. Durante el tratamiento, se fija un marco rígido al cráneo para mantener la cabeza inmóvil, garantizando la precisión del procedimiento. Este método también se conoce como radiocirugía estereotáxica y radioterapia estereotáxica.
Debido a que la radioterapia puede afectar al crecimiento y el desarrollo del cerebro en niños pequeños, especialmente en niños de 3 años o menos, se puede administrar quimioterapia para retrasar o reducir la necesidad de radioterapia.
La radioterapia dirigida al cerebro también puede afectar el crecimiento y el desarrollo de niños mayores de 3 años. Por esta razón, se están estudiando ensayos clínicos nuevas formas de administrar radiación que pueden tener menos efectos secundarios que los métodos estándar.
Quimioterapia
La quimioterapia (también llamada quimio) usa medicamentos para detener el crecimiento de las células cancerosas, ya sea destruyéndolas o impidiendo que se multipliquen. La quimioterapia se puede administrar sola o con otros tipos de tratamiento, como la radioterapia.
Para tratar el meduloblastoma, otros tumores embrionarios del sistema nervioso central y el pineoblastoma, la quimioterapia se administra por vía oral o se inyecta en una vena. Cuando se administra de esta manera, los medicamentos ingresan al torrente sanguíneo, permitiendo que alcancen las células cancerosas en todo el cuerpo. Las opciones de quimioterapia que pueden utilizarse solas o en combinación son:
- Carboplatino
- Cisplatino
- Ciclofosfamida
- Etopósido
- Irinotecán
- lomustina
- Metotrexato
- Temozolomida
- Tiotepa
- Topotecán
- Vincristina
También pueden utilizarse otros medicamentos quimioterápicos no incluidos en esta lista.
Más información sobre la quimioterapia para tratar el cáncer.
Quimioterapia de dosis alta con rescate de células madre autólogas
Se administran altas dosis de quimioterapia para eliminar las células cancerosas. Este tratamiento también afecta las células sanas, incluidas aquellas responsables de la producción de sangre. El trasplante de células madre es un procedimiento utilizado para reemplazar estas células productoras de sangre. Las células madre (células sanguíneas inmaduras) se extraen de la sangre o de la médula ósea del paciente, luego se congelan y almacenan. Una vez completada la quimioterapia, las células madre almacenadas se descongelan y se reinfunden en el paciente mediante una infusión. Estas células reinfundidas crecen y restauran la producción de células sanguíneas en el cuerpo.
Terapia dirigida
La terapia dirigida utiliza medicamentos u otras sustancias para bloquear la acción de enzimas, proteínas u otras moléculas específicas involucradas en el crecimiento y la propagación de las células cancerosas.
El vismodegib se puede usar para tratar el meduloblastoma recurrente en niños que han completado su crecimiento.
La terapia dirigida también está en estudio para el tratamiento del meduloblastoma y otros tumores embrionarios del SNC infantil que recidivan (regresan) después del tratamiento.
Obtenga más información en Terapia dirigida para tratar el cáncer.
Se están probando nuevos tipos de tratamiento en ensayos clínicos.
Un ensayo clínico de tratamiento es un estudio de investigación destinado a ayudar a mejorar los tratamientos actuales u obtener información sobre nuevos tratamientos para pacientes con cáncer. Para algunos pacientes, participar en un ensayo clínico puede ser la mejor opción de tratamiento.
Utilice nuestra herramienta de búsqueda de ensayos clínicos para encontrar ensayos clínicos sobre el cáncer respaldados por el NCI que admitan pacientes. Puede buscar ensayos según el tipo de cáncer, la edad del paciente y el lugar donde se realizan. Los ensayos clínicos respaldados por otras organizaciones se pueden encontrar en el sitio web ClinicalTrials.gov.
Obtenga más información en Información sobre estudios clínicos para pacientes y cuidadores. Debido a que el cáncer en los niños es raro, se debe considerar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos están abiertos solo a pacientes que no han iniciado el tratamiento.
Tratamiento del meduloblastoma infantil
Para más información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
Niños más pequeños con meduloblastoma
El tratamiento del meduloblastoma recién diagnosticado en niños de 3 años o menos consiste en:
- Cirugía para extirpar la mayor cantidad posible del tumor, seguida de quimioterapia
Otros tratamientos que se pueden administrar después de la cirugía son:
- Quimioterapia sistémica e intraventricular en dosis altas
- Quimioterapia en dosis altas con rescate de células madre
- Quimioterapia con o sin radioterapia en el área donde se extirpó el tumor
Niños mayores de 3 años con meduloblastoma de riesgo promedio
El tratamiento del meduloblastoma de riesgo promedio recién diagnosticado en niños mayores de 3 años consiste en:
- Cirugía para extirpar la mayor cantidad posible de tumor. A continuación, se realiza radioterapia en el cerebro y la médula espinal. También se puede administrar quimioterapia durante y después de la radioterapia.
- Cirugía para extirpar el tumor, radioterapia y quimioterapia de dosis alta con rescate de células madre
Niños mayores de 3 años con meduloblastoma de riesgo alto
El tratamiento del meduloblastoma de riesgo alto recién diagnosticado en niños mayores de 3 años consiste en:
- Cirugía para extirpar la mayor cantidad posible del tumor. A esto le sigue una dosis mayor de radioterapia al cerebro y la médula espinal que la dosis administrada para el meduloblastoma de riesgo promedio. La quimioterapia también se administra durante y después de la radioterapia.
- Cirugía para extirpar el tumor, radioterapia y quimioterapia de dosis alta con rescate de células madre
Tratamiento de otros tumores embrionarios (distintos del meduloblastoma) del SNC en niños
Para más información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
Niños de 3 años o menos con tumores embrionarios distintos del meduloblastoma y del meduloepitelioma
El tratamiento de tumores embrionarios distintos del meduloblastoma y del meduloepitelioma recién diagnosticados en niños de 3 años o menos consiste en:
- Cirugía para extirpar la mayor cantidad posible del tumor, seguida de quimioterapia
Niños mayores de 3 años con tumores embrionarios distintos del meduloblastoma y del meduloepitelioma
El tratamiento de los tumores embrionarios distintos del meduloblastoma y del meduloepitelioma recién diagnosticados en niños mayores de 3 años consiste en:
- Cirugía para extirpar la mayor cantidad posible de tumor. A continuación, se aplica radioterapia al cerebro y la médula espinal. También se administra quimioterapia durante y después de la radioterapia.
Niños con tumores embrionarios con rosetas multicapa o meduloepitelioma
El tratamiento del tumor embrionario recién diagnosticado con rosetas multicapa (ETMR) o meduloepitelioma puede consistir en:
- Cirugía para extirpar la mayor cantidad posible del tumor, seguida de quimioterapia. También puede administrarse radioterapia.
- Cirugía para extirpar el tumor, seguida de quimioterapia en dosis altas con rescate de células madre
Niños con neuroblastoma del SNC
El tratamiento del neuroblastoma del SNC recién diagnosticado puede consistir en:
- Cirugía para extirpar la mayor cantidad posible del tumor. A esto le sigue radioterapia al cerebro y la médula espinal. También se puede administrar quimioterapia.
Tratamiento del pineoblastoma infantil
Para más información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
Niños de 3 años y menores
El tratamiento del pineoblastoma recién diagnosticado en niños de 3 años o menos consiste en:
- Una biopsia para diagnosticar el pineoblastoma y cirugía para extirpar la mayor cantidad posible del tumor. Generalmente, se administra quimioterapia después de la cirugía.
- Cirugía seguida de quimioterapia en dosis altas con rescate de células madre
- Si el tumor responde a la quimioterapia, se administra radioterapia cuando el niño es mayor
Niños mayores de 3 años
El tratamiento del pineoblastoma recién diagnosticado en niños mayores de 3 años consiste en:
- Cirugía para extirpar la mayor parte posible del tumor. A continuación, se realiza radioterapia en el cerebro y la médula espinal y quimioterapia.
Tratamiento del meduloblastoma y otros tumores embrionarios del sistema nervioso central infantil recidivante
Para más información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento para el meduloblastoma infantil recurrente y otros tumores embrionarios del SNC puede consistir en:
- Una biopsia para diagnosticar meduloblastoma y otros tumores embrionarios del SNC. En algunos casos, se puede realizar una cirugía para extirpar la mayor cantidad posible del tumor.
- En el caso de los niños que recibieron radioterapia y quimioterapia anteriormente, el tratamiento puede incluir radioterapia repetida en el lugar donde se originó el cáncer y donde se ha propagado el tumor. También se puede utilizar radioterapia estereotáctica o quimioterapia.
- Para los bebés y niños pequeños que previamente recibieron solo quimioterapia y presentan una recurrencia local, el tratamiento puede consistir en quimioterapia complementada con radioterapia dirigida al tumor y al área circundante. También se puede realizar una cirugía para extirpar el tumor.
- Para los pacientes que han recibido radioterapia previamente, se puede considerar el uso de quimioterapia en dosis altas junto con rescate de células madre. Sin embargo, aún no se ha determinado si este tratamiento mejora la supervivencia.
- Terapia dirigida con un inhibidor de la transducción de señales (vismodegib) para pacientes cuyo cáncer presenta ciertos cambios en los genes.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Efectos secundarios
Puntos clave
- El tumor y su tratamiento pueden provocar síntomas que persisten incluso después de que el tratamiento haya finalizado.
El tumor y su tratamiento pueden provocar síntomas que persisten incluso después de que el tratamiento haya finalizado.
Los signos o síntomas causados por el tumor pueden comenzar antes del diagnóstico de cáncer y persistir durante meses o años. Es importante hablar con los médicos de su hijo sobre los signos o síntomas que puedan persistir después del tratamiento.
Los tratamientos contra el cáncer pueden causar efectos secundarios. La naturaleza de estos efectos dependerá del tipo de tratamiento, la dosis administrada y de cómo reaccione el cuerpo de su hijo o hija. Hable con el equipo de tratamiento del niño sobre los efectos secundarios a los que debe prestar atención y las formas de controlarlos.
Para obtener más información sobre los efectos secundarios que aparecen durante el tratamiento del cáncer, consulte la sección Efectos secundarios.
Los problemas derivados del tratamiento del cáncer que comienzan seis o más meses después del tratamiento y continúan durante meses o años se denominan efectos tardíos. A continuación se enumeran algunos efectos tardíos del tratamiento del cáncer:
- Problemas físicos que afectan a:
- El crecimiento y desarrollo de huesos y músculos
- La función tiroidea, cardiaca o auditiva
- Cambios en el estado de ánimo, los sentimientos, el pensamiento, el aprendizaje o la memoria
- Segundos cánceres (nuevos tipos de cáncer), como de tiroides u otros tumores cerebrales
Los niños diagnosticados con meduloblastoma pueden experimentar dificultades después de la cirugía o la radioterapia, como alteraciones en la capacidad de pensar, aprender y concentrarse. Además, el síndrome de mutismo cerebeloso puede aparecer tras la cirugía. Este síndrome se caracteriza por:
- Retraso en la capacidad para hablar
- Problemas para tragar y comer
- Pérdida del equilibrio, dificultad para caminar y empeoramiento de la escritura
- Pérdida del tono muscular
- Cambios de humor y de personalidad
Algunos efectos tardíos pueden tratarse o controlarse. Es importante hablar con los pediatras sobre los efectos que el tratamiento del cáncer puede tener en su hijo o hija. Para obtener más información, consulte Efectos tardíos del tratamiento anticanceroso en la niñez.
Atención de seguimiento
Algunas pruebas realizadas para diagnosticar el cáncer o determinar su estadio pueden repetirse para evaluar la efectividad del tratamiento. Los resultados de estas pruebas pueden influir en decisiones sobre continuar, modificar o suspender la terapia. A este proceso se le conoce como reestadificación. Más información sobre estas pruebas en la sección Información general.
Hay ciertas pruebas de diagnóstico por imágenes que continuarán realizándose periódicamente después de que finalice el tratamiento. Los resultados de estas pruebas pueden indicar si la afección de su hijo o hija ha cambiado o si el tumor cerebral ha reaparecido. Si las imágenes muestran tejido anómalo en el cerebro, se puede realizar una biopsia para determinar si se trata de células tumorales muertas o si están proliferando nuevas células cancerosas. Estas pruebas a menudo se denominan pruebas de seguimiento o controles y son fundamentales para evaluar la evolución del paciente.
Lidiar con el cáncer
Cuando un niño tiene cáncer, toda la familia necesita apoyo. Es fundamental cuidar también de uno mismo durante este difícil momento. Para recibir ayuda, comuníquese con el equipo médico de su hijo o hija, así como con familiares y miembros de la comunidad. Para más información, consulte Apoyo para familias: Cáncer infantil y el folleto Niños con cáncer: una guía para padres.
Recursos relacionados
Para obtener más información sobre el meduloblastoma infantil y otros tumores embrionarios del sistema nervioso central, consulte:
Para obtener más información sobre el cáncer infantil y otros recursos generales sobre el cáncer, consulte los siguientes sitios web:
- El cáncer
- Cánceres infantiles
- CureSearch para el cáncer infantil
- Efectos tardíos del tratamiento del cáncer infantil
- Adolescentes y adultos jóvenes con cáncer
- Niños con cáncer: una guía para padres
- El cáncer en los niños y los adolescentes
- Estadificación del cáncer
- Cómo hacer frente al cáncer
- Preguntas para el médico sobre el cáncer
- Para supervivientes, cuidadores e intercesores
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen del PDQ sobre el cáncer contiene información actualizada del tratamiento del meduloblastoma y otros tumores embrionarios del sistema nervioso central infantil. El propósito es informar y ayudar a los pacientes, sus familiares y cuidadores. No da pautas ni recomendaciones formales para tomar decisiones relacionadas con la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
La información de este resumen para pacientes procede de la versión para profesionales de la salud, la cual es revisada y actualizada periódicamente por el comité editorial del PDQ sobre el tratamiento pediátrico según sea necesario.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial de tratamiento pediátrico de PDQ®. PDQ Tratamiento del meduloblastoma infantil y otros tumores embrionarios del sistema nervioso central. Bethesda, MD: Instituto Nacional del Cáncer. Actualizado
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Actualizado:
URL de origen: https://www.cancer.gov/node/6311/syndication
Agencia de origen: National Cancer Institute (NCI)
Fecha de captura: 2013-09-14 09:03:26.0