








Complicaciones gastrointestinales
Acceda a una atención excepcional para complicaciones gastrointestinales y otros problemas relacionados con los cánceres gastrointestinales en Montefiore Einstein Comprehensive Cancer Center. Nuestro equipo multidisciplinario cuenta con una amplia experiencia en el tratamiento de esta afección. Como uno de los primeros centros del cáncer designados por el NCI, llevamos más de 50 años liderando la investigación, el diagnóstico y el tratamiento de más de 200 tipos de cáncer.
Estamos a la vanguardia en el tratamiento y la investigación de las complicaciones gastrointestinales y otros desafíos asociados con los cánceres gastrointestinales. Dado que muchos tratamientos contra el cáncer pueden provocar complicaciones gastrointestinales, estamos preparados para ayudar a controlar los efectos secundarios del tratamiento. Nuestra atención centrada en el paciente y basada en la evidencia aborda las necesidades únicas de cada paciente.
Si necesita atención médica para el cáncer gastrointestinal, confíe en nuestros proveedores, quienes se dedican con pasión a combatir el cáncer y a atender todas sus necesidades de salud.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Complicaciones gastrointestinales (PDQ®): versión para pacientes
Información general
El tracto gastrointestinal (GI) forma parte del sistema digestivo, que procesa los nutrientes de los alimentos que se ingieren y ayuda a eliminar los desechos del cuerpo. El tracto GI incluye el estómago y los intestinos .
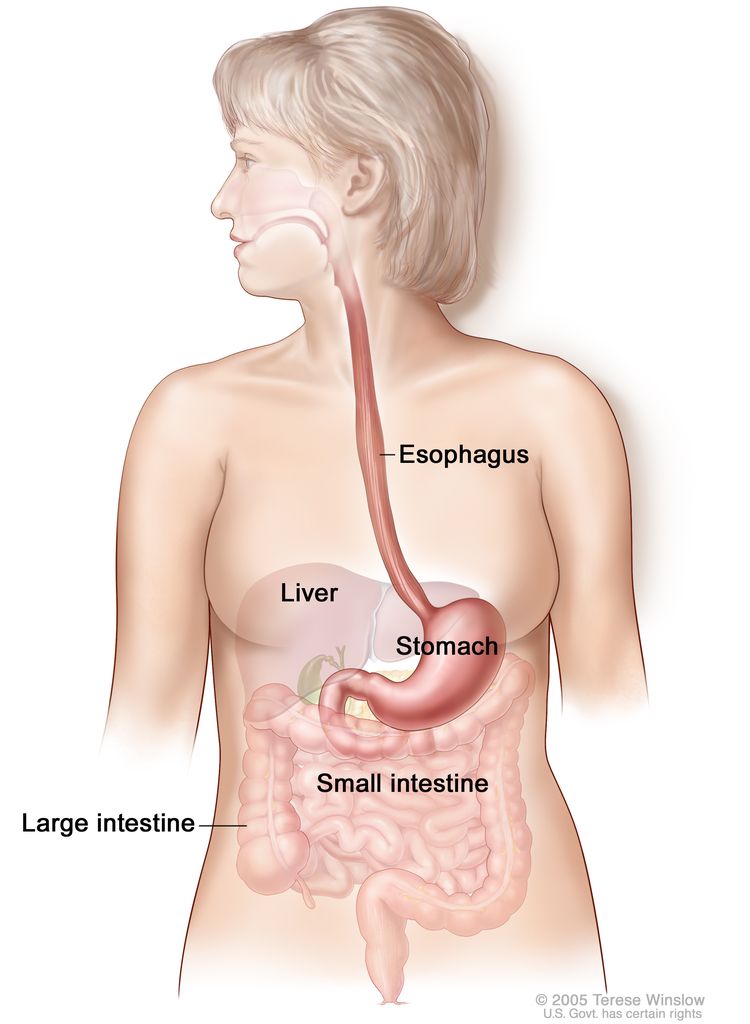
- Los alimentos pasan de la garganta al estómago a través de un tubo llamado esófago .
- Una vez que los alimentos y líquidos entran en el estómago, los músculos estomacales los descomponen y los mezclan con los jugos gástricos.
- Tras salir del estómago, los alimentos parcialmente digeridos pasan al intestino delgado y luego al intestino grueso .
- El extremo del intestino grueso, llamado recto, almacena los desechos de los alimentos digeridos hasta que son expulsados por el ano durante la defecación.
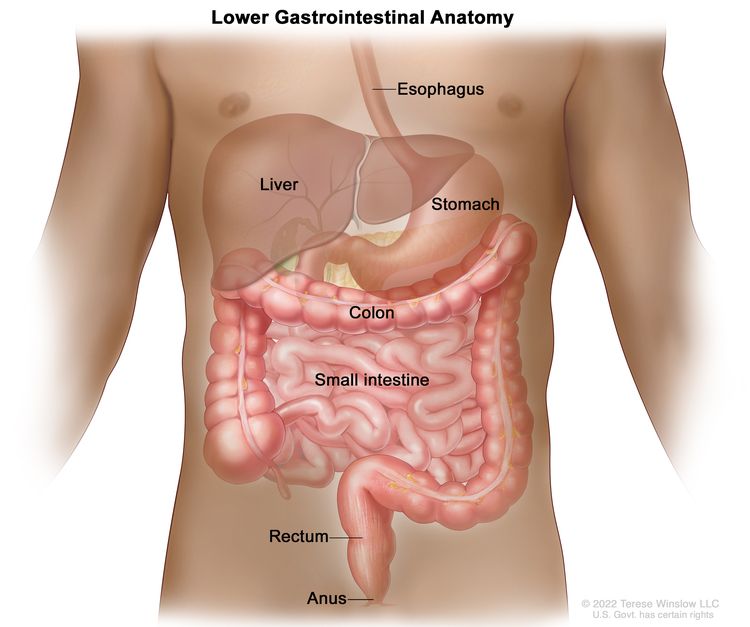
Anatomy of the lower gastrointestinal (digestive) system showing the colon, rectum, and anus. Other organs that make up the digestive system are also shown.
Las complicaciones gastrointestinales abarcan diversos problemas que pueden afectar al sistema digestivo. Son frecuentes en personas con cáncer y pueden deberse al propio cáncer, al tratamiento oncológico o a los medicamentos utilizados para controlar los síntomas.
Los niños y los adultos con cáncer pueden experimentar complicaciones gastrointestinales similares, pero las causas y los tratamientos varían según la edad y otros factores. Esta página describe las siguientes complicaciones gastrointestinales en adultos, sus causas y tratamientos:
Constipación
Puntos clave
- El estreñimiento es una afección en la que las deposiciones son difíciles o dolorosas de evacuar y no ocurren con mucha frecuencia.
- El estreñimiento es un problema común en las personas con cáncer.
- La evaluación del estreñimiento incluye la historia clínica, el examen físico y otras pruebas.
- Es importante prevenir y tratar el estreñimiento para evitar problemas graves.
El estreñimiento es una afección en la que las deposiciones son difíciles o dolorosas de evacuar y no ocurren con mucha frecuencia.
El estreñimiento se produce por el lento movimiento de las heces a través del intestino grueso . A medida que las heces se mueven lentamente por el intestino grueso, pierden líquido y se endurecen.
Una persona con estreñimiento puede ser incapaz de evacuar, tener que hacer más fuerza para evacuar o tener evacuaciones poco frecuentes.
No existe un número "normal" de deposiciones para una persona con cáncer. Cada persona es diferente. Sin embargo, si tiene deposiciones poco frecuentes, podría estar estreñido.
El estreñimiento es un problema común en las personas con cáncer.
Las causas comunes de estreñimiento incluyen la edad avanzada, cambios en la dieta y la ingesta de líquidos, y la falta de ejercicio. Además de estas causas comunes, otras causas de estreñimiento en personas con cáncer incluyen:
- Medicamentos. La quimioterapia, los opioides, los antidepresivos, los antiácidos y los diuréticos pueden causar estreñimiento al afectar los nervios y los músculos del tracto digestivo, lo que ralentiza los movimientos intestinales.
- Cambios en tus hábitos en el baño. Es posible que tengas poca o ninguna privacidad y necesites ayuda para ir al baño.
- Movilidad limitada. Los períodos prolongados de inactividad debido al cáncer pueden causar estreñimiento.
- Trastornos intestinales. Esto incluye trastornos como el síndrome del intestino irritable y la diverticulitis.
- Trastornos musculares y nerviosos. Una lesión en la médula espinal o la presión ejercida sobre ella por un tumor pueden causar estreñimiento.
- Cambios metabólicos. Algunos tipos de cáncer pueden afectar el apetito y la capacidad de absorber, almacenar y utilizar nutrientes.
- Depresión. La depresión puede provocar una disminución de la actividad física y alteraciones en las funciones corporales. El estreñimiento también puede ser un efecto secundario de los medicamentos para tratar la depresión.
La evaluación del estreñimiento incluye la historia clínica, el examen físico y otras pruebas.
Las siguientes pruebas y procedimientos pueden realizarse para ayudar a diagnosticar el estreñimiento:
- Historial médico: Se hablará con su médico sobre sus hábitos intestinales, incluyendo la frecuencia, la consistencia de las heces y si experimenta síntomas como dolor, hinchazón o náuseas cuando está estreñido. El médico también le preguntará sobre su dieta, la ingesta de líquidos y los medicamentos que toma, así como si ha habido cambios recientes en alguno de estos aspectos. En el caso de personas con colostomía, se abordará el cuidado de la misma.
- Examen físico: Un examen del cuerpo para comprobar el estado general de salud, incluyendo la detección de signos de enfermedad, como bultos o cualquier otra anomalía. El médico examinará el abdomen para comprobar si está inflamado, auscultará los ruidos intestinales y palpará posibles zonas dolorosas.
Si la causa del estreñimiento no queda clara a partir del historial médico y el examen físico, su médico puede solicitar más pruebas para averiguar si otro problema está causando el estreñimiento:
- Examen digital rectal (EDR): exploración del recto. El médico o el enfermero introduce un dedo enguantado y lubricado en la parte inferior del recto para palpar si hay bultos o cualquier otra cosa que parezca irregular. En las mujeres, también se puede examinar la vagina.
- Prueba de sangre oculta en heces: una prueba para detectar la presencia de sangre en las heces que solo se puede ver con un microscope. Se colocan pequeñas muestras de heces en tarjetas especiales y se entregan al médico o al laboratorio para su análisis.

Una prueba de guayacol en heces (FOBT, por sus siglas en inglés) busca sangre oculta en las heces. Se colocan pequeñas muestras de heces en una tarjeta especial y se envían a un médico o laboratorio para su análisis.
- Radiografía abdominal: Una radiografía de los órganos dentro del abdomen. Una radiografía es un tipo de radiación de alta energía que puede atravesar el cuerpo y quedar plasmada en una película, creando una imagen de las áreas internas del cuerpo.
- Sigmoidoscopia: Procedimiento para examinar el interior del recto y el colon sigmoide (parte inferior del colon) en busca de pólipos, áreas anormales o cáncer . Se introduce un sigmoidoscopio a través del recto hasta el colon sigmoide. El sigmoidoscopio es un instrumento delgado, con forma de tubo, que cuenta con una luz y una lente para la visualización. También puede incluir un instrumento para extraer pólipos o muestras de tejido, que se examinan al microscopio para detectar signos de cáncer.
- Colonoscopia: un procedimiento para observar el interior del recto y el colon en busca de pólipos, áreas anómalas o cáncer. Un colonoscopio se inserta a través del recto hasta el colon. Un colonoscopio es un instrumento delgado, similar a un tubo, con una luz y una lente para observar. También puede tener una herramienta para extraer pólipos o muestras de tejido, que se examinan al microscopio para detectar signos de cáncer.
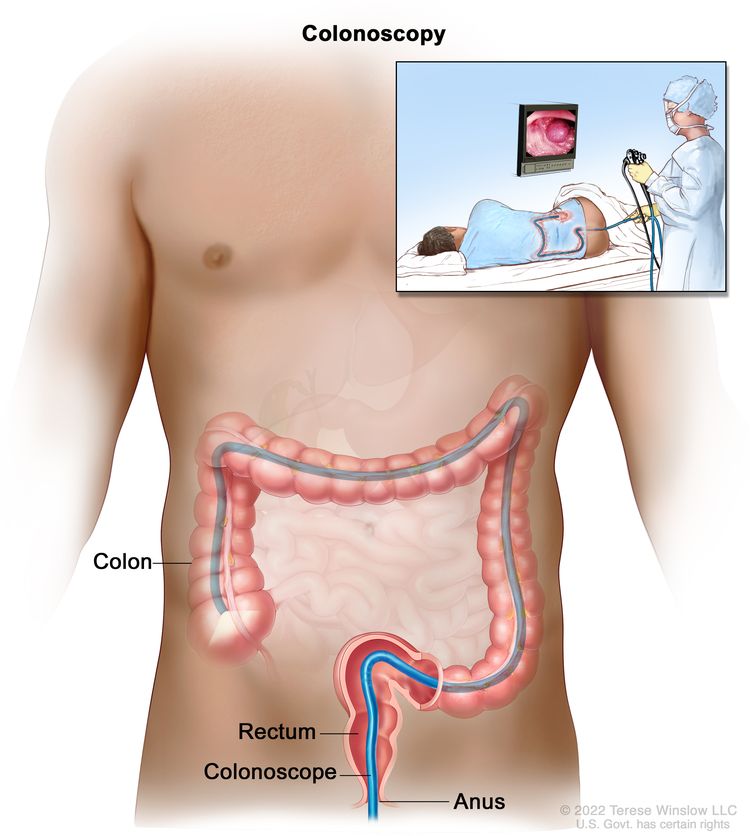
Colonoscopia. Se inserta un tubo delgado y con luz a través del ano y el recto hasta el colon para buscar áreas anómalas.
Es importante prevenir y tratar el estreñimiento para evitar problemas graves.
El equipo médico le informará sobre cómo prevenir y tratar el estreñimiento. El estreñimiento puede ser incómodo y causar malestar . Si no se trata, puede provocar impactación fecal, una afección grave en la que las heces no salen del colon o el recto. Es importante tratar el estreñimiento para prevenir la impactación fecal.
La prevención y el tratamiento del estreñimiento no son iguales para todas las personas. Lleve un registro de la frecuencia con la que evacúa y siga estos consejos para prevenir y tratar el estreñimiento:
- Beba más líquidos cada día, a menos que tenga una afección médica que restrinja la ingesta de líquidos.
- Haz ejercicio con regularidad. Las personas que no pueden caminar pueden hacer ejercicios abdominales en la cama o levantarse de la cama y sentarse en una silla.
- Aumenta la cantidad de fibra en tu dieta. Es importante beber más líquidos al consumir alimentos ricos en fibra para evitar que el estreñimiento empeore. Las personas que han tenido una obstrucción intestinal (del intestino delgado o grueso) o que se han sometido a una cirugía intestinal (por ejemplo, una colostomía) no deben seguir una dieta rica en fibra.
- Beba una bebida tibia o caliente aproximadamente media hora antes de la hora habitual de evacuar los intestinos.
- Busque intimidad y tranquilidad a la hora de evacuar.
- Utilice el inodoro o una silla con orinal en lugar de una bacinilla.
- Las personas que toman opioides podrían necesitar comenzar a tomar laxantes de inmediato para prevenir el estreñimiento. También se pueden administrar otros medicamentos para prevenirlo.
Las personas con riesgo de hemorragia o infección deben consultar con su médico antes de usar supositorios o enemas.
Impactación fecal
Puntos clave
- La impactación fecal es una forma grave de estreñimiento en la que las heces secas y duras no pueden salir del colon o del recto.
- La impactación fecal y el estreñimiento comparten síntomas similares, pero la impactación fecal puede causar otros síntomas graves, como problemas respiratorios, mareos o presión arterial baja.
- La evaluación del estreñimiento incluye la historia clínica, el examen físico y otras pruebas.
- La impactación fecal generalmente se trata con un enema.
La impactación fecal es una forma grave de estreñimiento en la que las heces secas y duras no pueden salir del colon o del recto.
La impactación fecal es la presencia de heces secas que no pueden ser expulsadas del cuerpo. El estreñimiento no tratado puede provocar impactación fecal. Por esta razón, las causas de la impactación fecal son las mismas que las del estreñimiento. Para obtener más información, consulte la sección sobre las causas del estreñimiento .
La impactación fecal y el estreñimiento comparten síntomas similares, pero la impactación fecal puede causar otros síntomas graves, como problemas respiratorios, mareos o presión arterial baja.
Los síntomas de la impactación fecal incluyen:
- ser incapaz de tener una evacuación intestinal
- tener que hacer más fuerza para evacuar pequeñas cantidades de heces duras y secas
- tener menos de lo habitual deposiciones
- tener el abdomen hinchado
- tener dolor de espalda o abdomen
- orinar con más o menos frecuencia de lo habitual, o ser incapaz de orinar.
- tener problemas respiratorios
- tener latidos cardíacos rápidos o dolor en el pecho
- mareos o presión arterial baja
- tener diarrea repentina y explosiva (a medida que las heces se mueven alrededor de la impactación)
- pérdida de heces al toser
- nausea and vomiting
- deshidración
- estar confundido y perder la noción del tiempo y el lugar, con latidos cardíacos rápidos, sudoración, fiebre y presión arterial alta o baja
Es importante que hable con su médico si presenta estos síntomas.
La evaluación del estreñimiento incluye la historia clínica, el examen físico y otras pruebas.
Las siguientes pruebas y procedimientos pueden realizarse para ayudar a diagnosticar la impactación fecal:
- Historial médico: Conversará con su médico sobre sus hábitos intestinales, incluyendo la frecuencia, la consistencia de las heces y si experimenta síntomas como dolor, hinchazón o náuseas cuando está estreñido. El médico también le preguntará sobre su dieta, la ingesta de líquidos y los medicamentos que toma, así como si ha habido cambios recientes en alguno de estos aspectos.
- Examen físico: Un examen del cuerpo para comprobar el estado general de salud, incluyendo la detección de signos de enfermedad, como bultos o cualquier otra anomalía. El médico examinará el abdomen para comprobar si está inflamado, auscultará los ruidos intestinales y palpará posibles zonas dolorosas.
- Radiografía abdominal: Una radiografía de los órganos dentro del abdomen. Una radiografía es un tipo de radiación de alta energía que puede atravesar el cuerpo y quedar plasmada en una película, creando una imagen de las áreas internas del cuerpo para detectar una posible impactación fecal.
- Examen digital rectal (EDR): examen del recto. El médico o el enfermero introduce un dedo enguantado y lubricado en la parte inferior del recto para palpar si hay impactación fecal, bultos o cualquier otra cosa que parezca anómala.
- Sigmoidoscopia:un procedimiento para mirar dentro del recto y colon sigmoide (inferior) para ver si hay una impactación fecal, pólipos, anómalas áreas o El cáncer. Un sigmoidoscopio se inserta a través del recto hasta el colon sigmoide. Un sigmoidoscopio es un instrumento delgado, similar a un tubo, con una luz y un lente para su visualización. También puede tener una herramienta para eliminar pólipos o tejidos muestras, que se controlan bajo un microscope para detectar signos de cáncer.
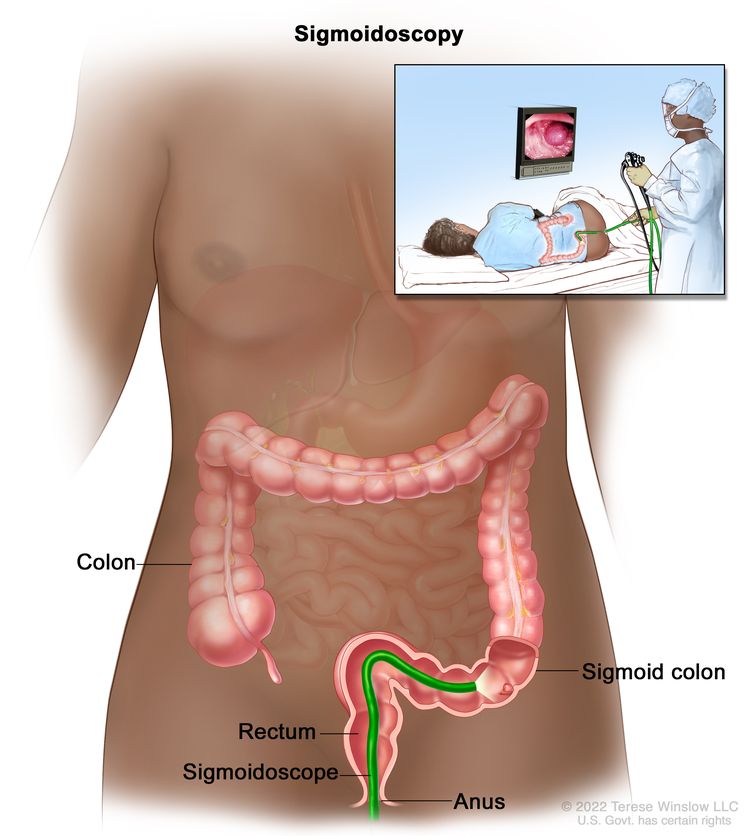
Sigmoidoscopia. Se inserta un tubo delgado con luz a través del ano y el recto hasta la parte inferior del colon para buscar áreas anómalas.
La impactación fecal generalmente se trata con un enema.
El tratamiento principal para la impactación fecal consiste en humedecer y ablandar las heces para facilitar su expulsión. Esto se suele realizar mediante un enema. Los enemas se administran únicamente bajo prescripción médica para reducir el riesgo de hemorragia o infección en pacientes con recuentos sanguíneos bajos y porque un exceso de enemas puede dañar el intestino . En algunos casos, puede ser necesario extraer las heces manualmente del recto una vez ablandadas.
Obstrucción intestinal
Puntos clave
- Una obstrucción intestinal es un bloqueo del intestino delgado o grueso por algo distinto a la impactación fecal.
- Una obstrucción intestinal puede causar dolor.
- La evaluación de una obstrucción intestinal incluye un examen físico y pruebas de imagen.
- El tratamiento para la obstrucción intestinal aguda puede incluir cirugía.
- El tratamiento de una obstrucción intestinal crónica y maligna puede incluir cirugía para mejorar la calidad de vida.
Una obstrucción intestinal es un bloqueo del intestino delgado o grueso por algo distinto a la impactación fecal.
Una obstrucción intestinal puede deberse a una torsión del intestino, una hernia, inflamación, tejido cicatricial tras una cirugía o cáncer. La obstrucción impide el paso de las heces a través del intestino delgado o grueso. El intestino puede estar parcial o totalmente bloqueado, e incluso puede presentar obstrucciones en dos puntos.
Una obstrucción intestinal puede provocar una disminución del flujo sanguíneo en una zona de los intestinos. Es necesario corregir este flujo sanguíneo, de lo contrario, el tejido afectado podría morir.
Los cánceres de estómago, colon y ovario pueden extenderse al abdomen y causar una obstrucción. Las personas con estos cánceres o que se han sometido a cirugía o radioterapia abdominal tienen un mayor riesgo de sufrir una obstrucción intestinal. Las obstrucciones intestinales son más frecuentes en las etapas avanzadas del cáncer.
Una obstrucción intestinal puede causar dolor.
Los siguientes pueden ser síntomas de una obstrucción intestinal:
- dolor o calambres abdominales
- hinchazón en el abdomen
- Constipación
- Diarrea
- náuseas o vómitos
- problemas para expulsar gases
- Pérdida del apetito
Es importante que hable con su médico si presenta estos síntomas.
La evaluación de una obstrucción intestinal incluye un examen físico y pruebas de imagen.
Se pueden realizar las siguientes pruebas y procedimientos para diagnosticar una obstrucción intestinal:
- Examen físico: Un examen del cuerpo para comprobar signos generales de salud, incluyendo la búsqueda de signos de enfermedad, como bultos o cualquier otra cosa que parezca inusual.
- Hemograma completo: procedimiento en el que se extrae una muestra de sangre y se examina:
- el número de glóbulos rojos, glóbulos blancos y plaquetas
- la cantidad de hemoglobina (la proteína que transporta oxígeno ) en los glóbulos rojos
- la porción de la muestra de sangre compuesta por glóbulos rojos
- Panel de electrolitos: análisis de sangre que mide los niveles de electrolitos, como sodio, potasio y cloruro.
- Análisis de orina: prueba para comprobar el color de la orina y su contenido, como azúcar, proteínas, glóbulos rojos y glóbulos blancos.
- Tomografía computarizada (TC): Este procedimiento utiliza una computadora conectada a un equipo de rayos X para obtener una serie de imágenes detalladas de áreas internas del cuerpo, como el abdomen, tomadas desde diferentes ángulos. Se puede inyectar un contraste en una vena o ingerirlo para que los órganos o tejidos se visualicen con mayor claridad. Este procedimiento también se conoce como tomografía computarizada o tomografía axial computarizada.
- Radiografía abdominal: radiografía de los órganos internos del abdomen. Un rayo X es un tipo de haz de energía que atraviesa el cuerpo y se plasma en una película, generando una imagen de áreas del interior del cuerpo.
- Enema de bario: una serie de radiografías de la parte inferior del tracto gastrointestinal. Un líquido que contiene bario (un blanco plateado metálico compuesto) se pone en el recto. El bario recubre el tracto gastrointestinal inferior y se toman radiografías. Este procedimiento también se denomina serie gastrointestinal inferior. Esta prueba puede mostrar qué parte del intestino está obstruida.
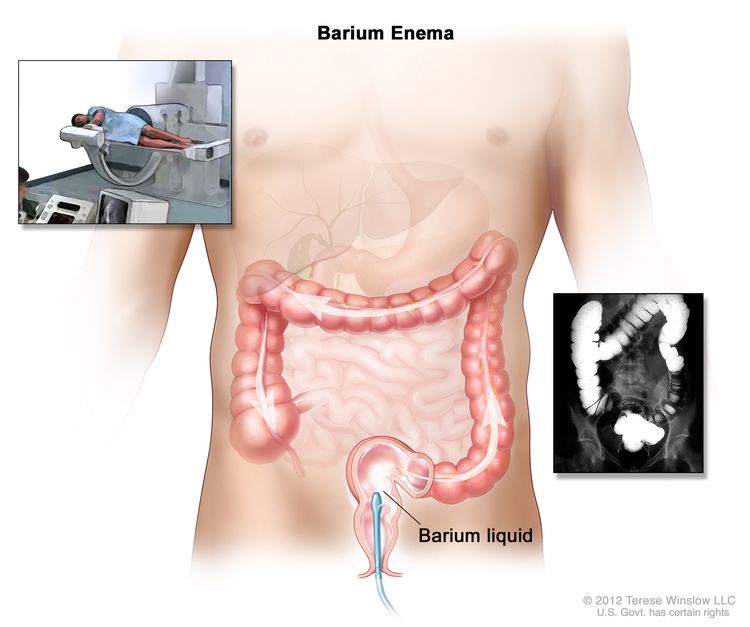
Procedimiento de enema de bario. El paciente se recuesta en una mesa de rayos X. Se introduce bario líquido en el recto y fluye a través del colon. Se toman radiografías para detectar áreas anómalas.
El tratamiento para la obstrucción intestinal aguda puede incluir cirugía.
Las obstrucciones intestinales agudas ocurren repentinamente y pueden tratarse. El tratamiento puede incluir lo siguiente:
- Terapia de reposición de líquidos: Un tratamiento para restablecer los niveles normales de líquidos en el cuerpo. Se pueden administrar líquidos intravenosos (IV) y se pueden recetar medicamentos .
- Corrección de electrolitos: Un tratamiento para obtener las cantidades adecuadas de sustancias químicas en la sangre, como sodio, potasio y cloruro. Los líquidos con electrolitos se pueden administrar por infusión .
- Transfusión de sangre: Procedimiento mediante el cual se administra a una persona una infusión de sangre entera o de partes de sangre.
- Reposo intestinal: Se suspende la ingesta de alimentos y, en ocasiones, de líquidos para dar tiempo a los intestinos a recuperarse.
- Sonda nasogástrica o colorrectal: Se inserta una sonda nasogástrica a través de la nariz y el esófago hasta el estómago . Se inserta una sonda colorrectal a través del recto hasta el colon . Esto se hace para disminuir la inflamación, eliminar la acumulación de líquidos y gases, y aliviar la presión.
- Stents: Tubo metálico que se inserta en el intestino para abrir la zona obstruida y aliviar los síntomas causados por la obstrucción.
- Cirugía: Se puede realizar una cirugía para aliviar la obstrucción si esta causa síntomas graves que no se alivian con otros tratamientos.
Las personas cuyos síntomas sigan empeorando serán sometidas a exámenes de seguimiento para comprobar si existen signos y síntomas de shock y para asegurarse de que la obstrucción no esté empeorando.
El tratamiento de una obstrucción intestinal crónica y maligna puede incluir cirugía para mejorar la calidad de vida.
Las obstrucciones intestinales crónicas malignas pueden empeorar con el tiempo. Las personas con cáncer avanzado pueden presentar obstrucciones intestinales crónicas que no se pueden eliminar mediante cirugía. El intestino puede estar bloqueado o estrechado en más de un punto, o el tumor puede ser demasiado grande para extirparlo por completo. Los tratamientos incluyen los siguientes:
- Cirugía: Se elimina la obstrucción para aliviar el dolor y mejorar la calidad de vida del paciente.
- Stent: Tubo metálico que se inserta en el intestino para abrir la zona obstruida, aliviar los síntomas y mejorar la calidad de vida del paciente.
- Sonda de gastrostomía: Tubo insertado a través de la pared abdominal directamente en el estómago. La sonda de gastrostomía puede conectarse a una bolsa de drenaje con válvula. Al abrir la válvula, el líquido y el aire acumulados pueden salir del estómago para aliviar los síntomas causados por la obstrucción. Además, las personas pueden comer o beber por vía oral, ya que los alimentos se drenan directamente a la bolsa. Esto les permite saborear la comida y mantener la boca húmeda. Se evitan los alimentos sólidos, ya que pueden obstruir la sonda que conecta con la bolsa de drenaje. Si la obstrucción no bloquea completamente el intestino, la sonda de gastrostomía también puede utilizarse para administrar medicamentos directamente en el estómago.
- Medicamentos: Inyecciones o infusiones de medicamentos para el dolor, las náuseas y los vómitos, y/o para vaciar los intestinos. Esto puede prescribirse a personas que no pueden someterse a cirugía o que no pueden recibir ayuda con un stent o una sonda de gastrostomía.
Diarrea
Puntos clave
- La diarrea consiste en deposiciones frecuentes, blandas y acuosas.
- El tratamiento del cáncer es la causa más común de diarrea en personas con cáncer.
- La evaluación de la diarrea incluye la historia clínica, el examen físico y las pruebas de laboratorio.
- El tratamiento de la diarrea depende de su causa.
La diarrea consiste en deposiciones frecuentes, blandas y acuosas.
La diarrea aguda se define como tres o más deposiciones blandas o líquidas en un solo día. Puede durar más de 4 días pero menos de 2 semanas. Las deposiciones frecuentes y líquidas que duran más de 2 meses se denominan diarrea crónica. La diarrea puede presentarse en cualquier momento durante el tratamiento del cáncer y puede ser física y emocionalmente estresante para las personas que lo padecen.
El tratamiento del cáncer es la causa más común de diarrea en personas con cáncer.
Las causas de diarrea en personas con cáncer incluyen las siguientes:
- Los tratamientos contra el cáncer, como Quimioterapia, Terapia dirigida, Inmunoterapia, Radioterapia, trasplante de médula ósea, and Cirugía.
- Algunos fármacos de quimioterapia y terapias dirigidas provocan diarrea al alterar la forma en que los nutrientes se descomponen y se absorben en el intestino delgado .
- La inmunoterapia es un tipo de tratamiento contra el cáncer que ayuda al sistema inmunitario a combatirlo. Al atacar las células cancerosas, también ataca las células y los tejidos sanos. Esto puede provocar diarrea.
- La radioterapia en el abdomen y la pelvis puede causar inflamación intestinal . La diarrea puede durar de 8 a 12 semanas después del tratamiento o puede no presentarse durante meses o años. Las personas que reciben radioterapia y quimioterapia suelen sufrir diarrea severa.
- Las personas que reciben un trasplante de médula ósea de donante pueden desarrollar la enfermedad de injerto contra huésped (EICH). Los síntomas gastrointestinales de la EICH incluyen náuseas y vómitos, dolor y calambres abdominales intensos y diarrea acuosa de color verde. Los síntomas pueden aparecer entre una semana y tres meses después del trasplante.
- Cirugía de estómago o intestinos
- El cáncer en sí
- Estrés y ansiedad por el diagnóstico de cáncer y su tratamiento
- Afecciones médicas y enfermedades distintas del cáncer
- Infecciones.
- Tratamiento con antibióticos para ciertas infecciones. El tratamiento con antibióticos puede irritar el revestimiento intestinal y causar diarrea que, a menudo, no mejora con el tratamiento.
- Alimentación por sonda.
- Impactación fecal en la que las heces se filtran alrededor de la obstrucción.
- Ciertos alimentos como los productos lácteos, las frutas, las verduras y los alimentos ricos en fibra o grasas.
La evaluación de la diarrea incluye la historia clínica, el examen físico y las pruebas de laboratorio.
La diarrea puede provocar complicaciones potencialmente mortales en personas con cáncer. Es importante determinar la causa para poder iniciar el tratamiento lo antes posible.
Para diagnosticar la diarrea y ayudar a planificar el tratamiento, se pueden realizar las siguientes pruebas y procedimientos:
- Historial médico: Conversará con su médico sobre sus hábitos urinarios e intestinales, incluyendo la frecuencia, la consistencia de las heces y si presenta síntomas como mareos, somnolencia, dolor, náuseas, vómitos o fiebre. El médico también le preguntará sobre su dieta y consumo de líquidos recientes, viajes recientes y los medicamentos que toma, así como la frecuencia de su administración.
- Examen físico: Un examen del cuerpo para comprobar el estado general de salud, incluyendo la detección de signos de enfermedad, como bultos o cualquier otra anomalía. El médico examinará el abdomen en busca de zonas dolorosas y auscultará los ruidos intestinales.
- Examen digital rectal (EDR): exploración del recto. El médico o el enfermero introduce un dedo enguantado y lubricado en la parte inferior del recto para palpar si hay bultos o cualquier otra cosa que parezca irregular. El examen busca signos de impactación fecal. Se pueden extraer heces para su análisis en el laboratorio.
- Prueba de sangre oculta en heces: prueba para detectar sangre en las heces, la cual solo se puede ver con un microscopio. Se colocan pequeñas muestras de heces en tarjetas especiales y se envían al médico o al laboratorio para su análisis.
- Análisis de heces: prueba de laboratorio para verificar los niveles de agua y sodio en las heces y detectar posibles sustancias que puedan estar causando diarrea. También se analizan las heces para detectar infecciones bacterianas, fúngicas o virales.
- Hemograma completo: procedimiento en el que se extrae una muestra de sangre y se examina:
- el número de glóbulos rojos, glóbulos blancos y plaquetas
- la cantidad de hemoglobina (la proteína que transporta oxígeno ) en los glóbulos rojos
- la porción de la muestra de sangre compuesta por glóbulos rojos
- Panel de electrolitos: análisis de sangre que mide los niveles de electrolitos, como sodio, potasio y cloruro.
- Análisis de orina: prueba para comprobar el color de la orina y su contenido, como azúcar, proteínas, glóbulos rojos y glóbulos blancos.
- Radiografía abdominal: Una radiografía de los órganos internos del abdomen. Una radiografía utiliza radiación de alta energía que atraviesa el cuerpo y se proyecta sobre una película, creando una imagen de las áreas internas. Las radiografías abdominales también se pueden realizar para detectar obstrucciones intestinales u otros problemas.
El tratamiento de la diarrea depende de su causa.
El tratamiento depende de la causa de la diarrea. El médico puede modificar sus medicamentos, dieta y/o líquidos. El tratamiento de la diarrea puede incluir lo siguiente:
- Puede ser necesario un cambio en el uso de laxantes.
- Se pueden recetar medicamentos para tratar la diarrea con el fin de ralentizar el funcionamiento de los intestinos, disminuir el líquido secretado por los intestinos y ayudar a absorber los nutrientes.
- La diarrea causada por el tratamiento del cáncer puede tratarse con cambios en la dieta. Coma en pequeñas cantidades y con frecuencia, y evite los siguientes alimentos:
- Beba más líquidos claros para mantenerse hidratado. Estos incluyen agua, bebidas deportivas, caldo, té descafeinado suave, refrescos sin cafeína, jugos claros y gelatina. En caso de diarrea severa, la persona podría necesitar líquidos intravenosos (IV) u otras formas de nutrición intravenosa.
- La diarrea causada por la enfermedad de injerto contra huésped (EICH) suele tratarse con una dieta especial. Algunas personas pueden necesitar tratamiento y control dietético a largo plazo.
- Se pueden recomendar probióticos . Los probióticos son microorganismos vivos que se utilizan como suplemento dietético para favorecer la digestión y el funcionamiento intestinal normal. Las investigaciones sobre el uso de Lactobacillus acidophilus y Bifidobacterium han demostrado beneficios en el tratamiento de la diarrea.
- Las personas que tienen diarrea con otros síntomas pueden necesitar líquidos y medicamentos administrados por vía intravenosa.
Enteritis por radiación
Puntos clave
- La enteritis por radiación es una inflamación del intestino causada por la radioterapia.
- La dosis total de radiación y otros factores afectan al riesgo de enteritis por radiación.
- La enteritis por radiación aguda y crónica presentan síntomas similares.
- La evaluación de la enteritis por radiación incluye un examen físico y la historia clínica.
- El tratamiento de la enteritis aguda por radiación incluye el tratamiento de los síntomas.
- El tratamiento de la enteritis crónica por radiación puede incluir los mismos tratamientos que la enteritis aguda por radiación.
La enteritis por radiación es una inflamación del intestino causada por la radioterapia.
El intestino delgado y el grueso son sensibles a la radiación . La radioterapia administrada para eliminar las células cancerosas en el abdomen y la pelvis afecta a las células normales del revestimiento intestinal. La radioterapia detiene el crecimiento de las células cancerosas y otras células de rápido crecimiento. Dado que las células normales del revestimiento intestinal crecen rápidamente, la radiación en esa zona puede detener su crecimiento. Esto dificulta la reparación del tejido. A medida que las células mueren y no se reemplazan, se producen problemas gastrointestinales en los días y semanas siguientes.
La enteritis por radiación es una afección en la que la mucosa intestinal se inflama durante o después de la radioterapia en el abdomen, la pelvis o el recto . Cuanto mayor sea la dosis de radiación, mayor será el daño que se puede causar al tejido sano.
La enteritis por radiación puede ser aguda o crónica:
- La enteritis aguda por radiación se produce durante la radioterapia o dentro de los tres meses posteriores a su finalización.
- La enteritis crónica por radiación puede aparecer meses después de finalizar la radioterapia.
La dosis total de radiación y otros factores afectan al riesgo de enteritis por radiación.
La duración y la gravedad de la enteritis dependen de lo siguiente:
- el tipo y la dosis total de radiación recibida
- la cantidad de intestino normal tratado
- el tamaño del tumor y cuánto se ha extendido
- si la quimioterapia se administró al mismo tiempo que la radioterapia.
- Si la persona ha sido sometida a cirugía en el abdomen o la pelvis.
- si la persona tiene presión arterial alta, diabetes, antecedentes de tabaquismo o mala nutrición
Entre el 10% y el 20% de las personas tratadas con radiación en el abdomen presentarán problemas crónicos.
La enteritis por radiación aguda y crónica presentan síntomas similares.
Las personas con enteritis aguda por radiación pueden presentar los siguientes síntomas:
- Náuseas
- Vómitos
- calambres abdominales
- Ganas frecuentes de defecar
- Dolor rectal, sangrado o mucosidad en las heces.
- diarrea acuosa
- Cansancio excesivo
Los síntomas de enteritis aguda generalmente desaparecen entre dos y tres semanas después de finalizar el tratamiento.
Los síntomas de la enteritis crónica por radiación suelen aparecer entre 6 y 18 meses después de finalizar la radioterapia. Su diagnóstico puede ser difícil. El médico primero verificará si los síntomas se deben a un tumor recurrente en el intestino. También necesitará conocer el historial completo de tratamientos de radiación del paciente.
Las personas con enteritis por radiación crónica pueden presentar los siguientes signos y síntomas:
- dolor abdominal
- diarrea con sangre
- heces grasosas y aceitosas
- pérdida de peso
- Náuseas
- Vómitos
Es importante que hable con su médico si presenta estos síntomas.
La evaluación de la enteritis por radiación incluye un examen físico y la historia clínica.
El médico realizará un examen físico y hará preguntas sobre lo siguiente:
- patrón habitual de deposiciones
- patrón de diarrea:
- cuando empezó
- cuánto tiempo ha durado
- con qué frecuencia ocurre
- cantidad y tipo de heces
- otros síntomas junto con la diarrea (como gases, calambres, hinchazón, urgencia, sangrado y dolor rectal)
- nutrición y salud:
- altura y peso
- hábitos alimenticios habituales
- cambios en los hábitos alimenticios
- cantidad de fibra en la dieta
- signos de deshidratación (como tono de piel apagado, mayor debilidad o sensación de mucho cansancio)
- niveles de estrés y capacidad para afrontarlo
- cambios en el estilo de vida causados por la enteritis
El tratamiento de la enteritis aguda por radiación incluye el tratamiento de los síntomas.
Los síntomas de la enteritis por radiación suelen mejorar con el tratamiento, pero si empeoran, puede que haya que interrumpir el tratamiento oncológico durante un tiempo.
El tratamiento de la enteritis aguda por radiación o de sus síntomas puede incluir:
- medicamentos antiinflamatorios que mejoran el flujo sanguíneo a través del cuerpo
- antibióticos
- Esteroides
- medicamentos para detener la diarrea y reducir el colesterol en la sangre
- vitamina E
- probiótico
- cambios en la dieta
- Los intestinos dañados por la radioterapia pueden no producir suficiente cantidad de ciertas sustancias. enzimas necesarias para la digestión, especialmente lactasa. La lactasa es necesaria para digerir lactosa, que se encuentra en la leche y los productos lácteos. Una dieta sin lactosa, baja en grasas y baja en fibra puede ayudar a controlar los síntomas de la enteritis aguda. Alimentos que se deben evitar:
- leche y algunos productos lácteos
- pan y cereales integrales
- frutos secos, semillas y coco
- alimentos fritos, grasosos o aceitosos
- Frutas frescas y secas, y algunos zumos de frutas (como el zumo de ciruelas pasas).
- verduras crudas
- pasteles ricos
- palomitas de maíz, papas fritas y pretzels
- especias y hierbas fuertes
- chocolate, café, té y refrescos con cafeína
- alcohol y tabaco
- Alimentos a elegir:
- pescado, aves y carne asados a la parrilla o al horno
- plátanos
- puré de manzana y manzanas peladas
- zumos de manzana y uva
- pan blanco y tostadas
- pastas
- patatas asadas, hervidas o en puré
- Verduras cocidas de sabor suave, como puntas de espárragos, judías verdes y amarillas, zanahorias, espinacas y calabaza.
- queso procesado suave, que puede no causar problemas porque se le quita la lactosa durante su elaboración.
- Suplementos para batidos sin lactosa, como suero de leche, yogur y otros, como Ensure.
- huevos
- mantequilla de cacahuete suave
- Consejos útiles:
- Consuma los alimentos a temperatura ambiente.
- Beba aproximadamente 12 vasos de 240 ml (8 onzas) de líquido al día.
- Deje que los refrescos pierdan su efervescencia antes de beberlos.
- Agregue nuez moscada a la comida. Esto ayuda a ralentizar el movimiento de los alimentos digeridos en los intestinos.
- Comience una dieta baja en fibra el primer día de radioterapia.
- Los intestinos dañados por la radioterapia pueden no producir suficiente cantidad de ciertas sustancias. enzimas necesarias para la digestión, especialmente lactasa. La lactasa es necesaria para digerir lactosa, que se encuentra en la leche y los productos lácteos. Una dieta sin lactosa, baja en grasas y baja en fibra puede ayudar a controlar los síntomas de la enteritis aguda. Alimentos que se deben evitar:
El tratamiento de la enteritis crónica por radiación puede incluir los mismos tratamientos que la enteritis aguda por radiación.
El tratamiento de la enteritis por radiación crónica puede incluir lo siguiente:
- Los mismos tratamientos que para los síntomas de enteritis por radiación aguda.
- En algunos pacientes puede ser necesaria la cirugía para controlar los síntomas. Se pueden utilizar dos tipos de cirugía:
- Bypass intestinal: Procedimiento en el que el médico crea una nueva vía para el flujo del contenido intestinal alrededor del tejido dañado.
- Resección intestinal total: Cirugía para extirpar completamente los intestinos.
Ensayos clínicos actuales
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Obtenga más información sobre las complicaciones gastrointestinales
Para obtener más información del Instituto Nacional del Cáncer sobre el estreñimiento o la diarrea, consulte lo siguiente:
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen de información sobre el cáncer del PDQ contiene información actualizada sobre las causas y el tratamiento de las complicaciones gastrointestinales, como la constipación o estreñimiento, la impactación intestinal, la obstrucción intestinal, la diarrea y la enteritis por radiación. Su objetivo es informar y ayudar a los pacientes, las familias y los cuidadores. No proporciona directrices ni recomendaciones formales para tomar decisiones sobre la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
La información de este resumen para pacientes se obtuvo de la versión para profesionales de la salud, que el comité editorial del PDQ sobre cuidados paliativos y de apoyo revisa con regularidad y actualiza en caso necesario.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre cuidados paliativos y de apoyo. Complicaciones gastrointestinales (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Actualizado:
URL de origen: https://www.cancer.gov/node/2328/syndication
Agencia de origen: National Cancer Institute (NCI)
Fecha de captura: 2013-09-14 09:00:53.0