








Mieloma múltiple y cánceres de células plasmáticas
Acceda a una atención excepcional para el mieloma múltiple, los cánceres de células plasmáticas y otros tipos de cáncer de sangre y médula ósea en el Centro Oncológico Integral Montefiore Einstein. Nuestro equipo multidisciplinario cuenta con amplia experiencia en el tratamiento de estos cánceres poco comunes. Como uno de los primeros centros oncológicos designados por el NCI, durante más de 50 años hemos sido líderes en la investigación, el diagnóstico y el tratamiento de más de 200 tipos de cáncer.
Estamos a la vanguardia en el tratamiento e investigación del linfoma de Hodgkin y otros cánceres de sangre y médula ósea. Contamos con amplia experiencia en todo el espectro de cánceres de sangre, incluyendo trasplantes de células madre y otros tratamientos celulares como la terapia con células T CAR, un tratamiento innovador que ayuda al sistema inmunitario del cuerpo a combatir mejor el cáncer. En particular, actualmente estamos tratando a pacientes con mieloma múltiple BCMA con terapia de células T CAR como parte de ensayos clínicos en curso.
Cuando necesite atención médica del cáncer de células plasmáticas, recurra a nuestros proveedores, a quienes les apasiona acabar con el cáncer y abordar todas sus necesidades de salud.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Tratamiento de las neoplasias de células plasmáticas (incluido el mieloma múltiple) (PDQ®): versión para pacientes
Información general sobre las neoplasias de células plasmáticas
Puntos clave
- Las neoplasias de células plasmáticas son enfermedades en las que el cuerpo produce demasiadas células plasmáticas.
- Las neoplasias de células plasmáticas pueden ser benignas (no cancerosas) o malignas (cancerosas).
- Existen varios tipos de neoplasias de células plasmáticas.
- Gammapatía monoclonal de significado incierto (GMSI)
- Plasmacitoma
- Mieloma múltiple
- El mieloma múltiple y otras neoplasias de células plasmáticas pueden producir una enfermedad llamada amiloidosis.
- La edad puede afectar el riesgo de desarrollar neoplasias de células plasmáticas.
- Las pruebas que examinan la sangre, la médula ósea y la orina se utilizan para diagnosticar el mieloma múltiple y otras neoplasias de células plasmáticas.
- Certain factors affect prognosis (chance of recovery) and treatment options.
Las neoplasias de células plasmáticas son enfermedades en las que el cuerpo produce demasiadas células plasmáticas.
Las células plasmáticas se desarrollan a partir de los linfocitos B (células B), un tipo de glóbulo blanco que se produce en la médula ósea . Normalmente, cuando las bacterias o los virus entran en el cuerpo, algunas células B se transforman en células plasmáticas. Las células plasmáticas producen anticuerpos para combatir las bacterias y los virus, y así prevenir infecciones y enfermedades.
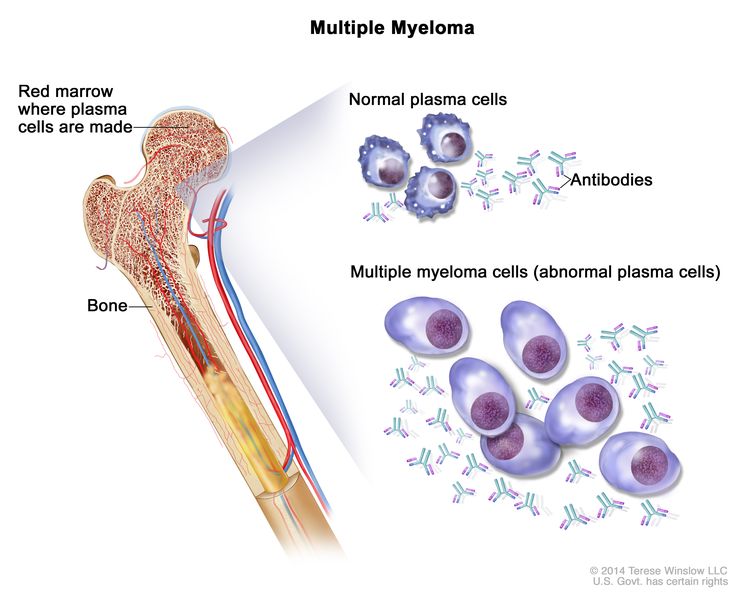
Mieloma múltiple. Las células de mieloma múltiple son células plasmáticas anómalas (un tipo de glóbulo blanco) que se acumulan en la médula ósea y forman tumores en muchos huesos del cuerpo. Las células plasmáticas normales producen anticuerpos para ayudar al cuerpo a combatir infecciones y enfermedades. A medida que aumenta la cantidad de células de mieloma múltiple, se producen más anticuerpos. Esto puede hacer que la sangre se espese, lo que evita que la médula ósea produzca suficientes células sanguíneas sanas. Las células de mieloma múltiple también dañan y debilitan el hueso.
Las neoplasias de células plasmáticas son enfermedades en las que las células plasmáticas anómalas forman tumores en los huesos o los tejidos blandos del cuerpo. Las células plasmáticas también producen una proteína de anticuerpos, llamada proteína M, que el cuerpo no necesita y no ayuda a combatir las infecciones. Estas proteínas de anticuerpos se acumulan en la médula ósea y pueden provocar el espesamiento de la sangre o dañar los riñones.
Las neoplasias de células plasmáticas pueden ser benignas (no cancerosas) o malignas (cancerosas).
Si bien la gammapatía monoclonal de significado incierto (GMSI) no es cáncer, puede llegar a convertirse. Los siguientes tipos de neoplasias de células plasmáticas son cáncer:
- Linfoma linfoplasmocítico (también llamado macroglobulinemia de Waldenström). Para obtener más información, consulte la página del Tratamiento del linfoma no Hodgkin.
- Plasmacitoma.
- Mieloma múltiple.
Existen varios tipos de neoplasias de células plasmáticas.
Los tipos de neoplasia de células plasmáticas son:
Gammapatía monoclonal de significado incierto (GMSI)
En este tipo de neoplasia de células plasmáticas, menos del 10 % de la médula ósea está formada por células plasmáticas anómalas y no hay presencia de cáncer. Estas células plasmáticas anómalas producen proteína M, que a veces se detecta en los análisis de sangre u orina de rutina. En la mayoría de los pacientes, la cantidad de proteína M permanece igual y no se manifiestan signos, síntomas ni problemas de salud.
En algunos pacientes, la GMSI puede convertirse en una afección más grave con el tiempo, como la amiloidosis, o producir problemas en los riñones, el corazón o los nervios. La GMSI también puede convertirse en cáncer, como el mieloma múltiple, el linfoma linfoplasmocítico o la leucemia linfocítica crónica.
Plasmacitoma
En este tipo de neoplasia de células plasmáticas, las células plasmáticas anómalas (células de mieloma) están concentradas en un lugar y forman un tumor, llamado plasmocitoma. A veces, el plasmocitoma se puede curar. Hay dos tipos de plasmocitoma.
- En el plasmocitoma óseo aislado, se forma un tumor de células plasmáticas en el hueso, menos del 10 % de la médula ósea está formada por células plasmáticas y no hay otros signos de cáncer. El plasmocitoma óseo a menudo se convierte en mieloma múltiple.
- En el plasmocitoma extramedular, se forma un tumor de células plasmáticas en el tejido blando, pero no en el hueso ni en la médula ósea. Los plasmocitomas extramedulares comúnmente se forman en los tejidos de la garganta, las amígdalas y los senos paranasales.
Los signos y síntomas dependen de la ubicación del tumor.
- En los huesos, el plasmocitoma puede provocar dolor o fracturas.
- En el tejido blando, el tumor puede presionar áreas cercanas y causar dolor u otros problemas. Por ejemplo, un plasmocitoma en la garganta poría dificultar la deglución.
Mieloma múltiple
En el mieloma múltiple, las células plasmáticas anómalas (células de mieloma) se acumulan en la médula ósea y forman tumores en muchos huesos del cuerpo. Estos tumores pueden impedir que la médula ósea produzca suficientes células sanguíneas sanas. Normalmente, la médula ósea produce células madre (células inmaduras) que se convierten en tres tipos de células sanguíneas maduras:
- Glóbulos rojos, que transportan oxígeno y otras sustancias a todos los tejidos del cuerpo
- Glóbulos blancos que combaten infecciones y enfermedades
- Plaquetas que forman coágulos de sangre para ayudar a prevenir hemorragias
A medida que aumenta la cantidad de células de mieloma, se producen menos glóbulos rojos, glóbulos blancos y plaquetas. Las células de mieloma también dañan y debilitan el hueso.
En ocasiones, el mieloma múltiple no causa ningún signo ni síntoma. Esto se denomina mieloma múltiple latente. Puede detectarse cuando se realiza un análisis de sangre u orina para otra afección. Los signos y síntomas pueden ser causados por el mieloma múltiple u otras afecciones. Consulte con su médico si presenta alguno de los siguientes síntomas:
- Dolor de huesos, especialmente en la espalda o las costillas
- Huesos que se fracturan con facilidad.
- Fiebre sin causa aparente o infecciones frecuentes
- Predisposición a hematomas o hemorragias
- Dificultad para respirar
- Debilidad de los brazos o piernas
- Cansancio extremo
Un tumor puede dañar el hueso y provocar hipercalcemia (un nivel demasiado elevado de calcio en la sangre). Esto puede afectar a muchos órganos del cuerpo, como los riñones, los nervios, el corazón, los músculos y el tracto digestivo, así como causar problemas de salud graves.
La hipercalcemia puede provocar los siguientes signos y síntomas:
El mieloma múltiple y otras neoplasias de células plasmáticas pueden producir una enfermedad llamada amiloidosis.
En casos poco frecuentes, el mieloma múltiple puede provocar el fallo de los nervios periféricos (nervios que no están en el cerebro ni en la médula espinal) y de los órganos. Esto puede deberse a una afección llamada amiloidosis, en la que las proteínas de anticuerpos se acumulan y se adhieren entre sí en los nervios periféricos y los órganos, como los riñones y el corazón. Esta acumulación puede endurecer estos tejidos e impedir que funcionen correctamente.
La amiloidosis puede provocar los siguientes signos y síntomas:
La edad puede afectar el riesgo de desarrollar neoplasias de células plasmáticas.
Cualquier factor que aumenta la probabilidad de que una persona desarrolle una enfermedad se denomina factor de riesgo. No todas las personas con uno o más de estos factores de riesgo desarrollarán neoplasias de células plasmáticas, y estas pueden desarrollarse en personas sin ningún factor de riesgo conocido. Consulte con su médico si cree que podría estar en riesgo.
Las neoplasias de células plasmáticas son más comunes en personas de mediana edad o mayores. Para el mieloma múltiple y el plasmocitoma, otros factores de riesgo son:
- Ser negro
- Ser hombre
- Tener un historial personal de GMSI o plasmocitoma
- Estar expuesto a radiación o ciertos químicos
Se están llevando a cabo estudios sobre cómo los factores raciales, sociales y financieros afectan el acceso al tratamiento y las tasas de neoplasias de células plasmáticas.
Las pruebas que examinan la sangre, la médula ósea y la orina se utilizan para diagnosticar el mieloma múltiple y otras neoplasias de células plasmáticas.
In addition to asking about your personal and family health history and doing a physical exam, your doctor may perform the following tests and procedures:
- Estudios de inmunoglobulinas en sangre y orina.: es un procedimiento en el que se analiza una muestra de sangre u orina para medir la cantidad de ciertos anticuerpos (inmunoglobulinas). En el caso del mieloma múltiple, se miden la beta-2-microglobulina, la proteína M, las cadenas ligeras libres y otras proteínas producidas por las células del mieloma. Una cantidad superior a la normal de estas sustancias puede ser un signo de enfermedad.
- Aspiración y biopsia de médula ósea: consiste en la extracción de médula ósea, sangre y un pequeño fragmento de hueso mediante la inserción de una aguja hueca en el hueso de la cadera o el esternón. Un pathologist observará la médula ósea, la sangre y el hueso con un microscope para verificar si hay presencia de células anómalas. Se pueden realizar las siguientes pruebas sobre la muestra de tejido extraída durante la aspiración y biopsia de médula ósea:
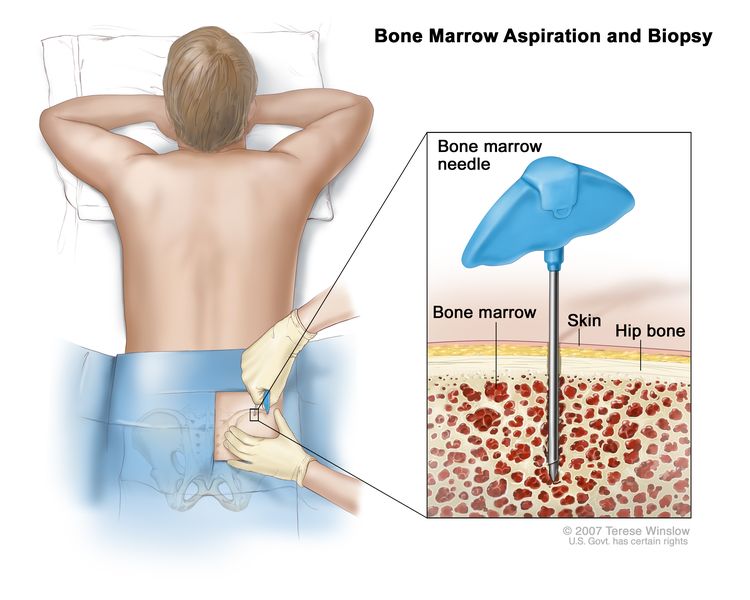
Aspiración y biopsia de médula ósea. Tras anestesiar una pequeña zona de la piel, se introduce una aguja larga y hueca a través de la piel y el hueso de la cadera del paciente hasta la médula ósea. Se extrae una muestra de médula ósea y un pequeño fragmento de hueso para su examen microscópico.
- Análisis citogenético: es una prueba de laboratorio en la que se cuentan los cromosomas de las células de una muestra de médula ósea y se comprueba si hay cambios, como cromosomas fragmentados, ausentes, reorganizados o adicionales. Los cambios en ciertos cromosomas pueden ser un signo de cáncer. El análisis citogenético se utiliza para diagnosticar el cáncer, planificar el tratamiento o determinar qué tan bien está funcionando el mismo.
- Hibridación in situ con fluorescencia (FISH): prueba de laboratorio que se utiliza para observar y contar genes o cromosomas en células y tejidos. Se generan fragmentos de ADN con colorantes fluorescentes en el laboratorio y se añaden a una muestra de células o tejidos del paciente. Cuando estos fragmentos de ADN teñidos se unen a ciertos genes o zonas de cromosomas en la muestra, se iluminan al observarlos con un microscopio de fluorescencia. La prueba FISH se utiliza para diagnosticar el cáncer y planificar el tratamiento.
- Citometría de flujo: es una prueba de laboratorio que mide la cantidad de células en una muestra, el porcentaje de células vivas y ciertas características celulares, como el tamaño, la forma y la presencia de marcadores tumorales (u otros) en la superficie celular. Para esta prueba, se tiñen las células de una muestra de médula ósea con un tinte fluorescente, se colocan en un líquido y luego se pasan una a la vez a través de un haz de luz. Los resultados se basan en cómo reaccionan las células teñidas al haz de luz. Esta prueba se utiliza para diagnosticar y controlar ciertos tipos de cánceres, como la leucemia y el linfoma.
- Estudio de los huesos esqueléticos: en un estudio de los huesos esqueléticos, se toman radiografías de todos los huesos del cuerpo. Las radiografías se utilizan para encontrar áreas donde el hueso está dañado. Una radiografía es un tipo de haz de energía que puede atravesar el cuerpo y plasmarse en una película, lo que genera una imagen de las áreas internas del cuerpo.
- Hemograma completo (CBC, por sus siglas en inglés) con diferencial: procedimiento en el que se extrae una muestra de sangre y se examina:
- El número de glóbulos rojos y plaquetas
- El número y tipo de glóbulos blancos
- La cantidad de hemoglobina (la proteína que transporta el oxígeno) en los glóbulos rojos
- La parte de la muestra de sangre compuesta por glóbulos rojos.
- Estudios de química sanguínea: es un procedimiento en el que se analiza una muestra de sangre para medir la cantidad de ciertas sustancias, como el calcio o la albúmina, liberadas a la sangre por los órganos y tejidos del cuerpo. Una cantidad inusual (mayor o menor de lo normal) de una sustancia puede ser un signo de enfermedad.
- Prueba de orina de veinticuatro horas: es una prueba en la que se recolecta orina durante 24 horas para medir la cantidad de ciertas sustancias. Una cantidad inusual (más alta o más baja de lo normal) de una sustancia puede ser un signo de enfermedad en el órgano o tejido que la produce. Una cantidad de proteína superior a la normal podría ser un signo de mieloma múltiple.
- Resonancia magnética (imagen por resonancia magnética): es un procedimiento que utiliza un imán, ondas de radio y una computadora para generar una serie de imágenes detalladas de áreas internas del cuerpo. Este procedimiento también se llama resonancia magnética nuclear (NMRI). Se puede usar una resonancia magnética de la columna y la pelvis para identificar áreas donde el hueso está dañado.
- Exploración PET (tomografía por emisión de positrones): es un procedimiento que se utiliza para detectar células tumorales malignas en el cuerpo. Se inyecta una pequeña cantidad de glucosa (azúcar) radiactiva en una vena. El escáner PET gira alrededor del cuerpo y genera una imagen que muestra dónde se está utilizando la glucosa en el cuerpo. Las células tumorales malignas aparecen más brillantes en la imagen porque tienen un mayor nivel de actividad y absorben más glucosa que las células normales.
- Exploración por tomografía computarizada (TC): es un procedimiento que genera una serie de imágenes detalladas de las áreas internas del cuerpo, como la columna vertebral, tomadas desde diferentes ángulos. Las imágenes son tomadas por una computadora conectada a una máquina de rayos X. Se puede inyectar un tinte en una vena o ingerirlo para permitir que los órganos o los tejidos se visualicen con más claridad. Este procedimiento también se denomina tomografía axial computarizada.
- Exploración PET-TC: es un procedimiento que combina una tomografía por emisión de positrones (PET) y una tomografía computarizada (CT). Las exploraciones PET y TC se realizan al mismo tiempo con la misma máquina. Al combinar ambos procedimientos, se generan imágenes más detalladas de las áreas internas del cuerpo, como la columna vertebral, que las que se obtendrían realizando cada exploración por sí sola.
Certain factors affect prognosis (chance of recovery) and treatment options.
El pronóstico depende de los siguientes factores:
- El tipo de neoplasia de células plasmáticas
- El estadio de la enfermedad
- Si hay presencia de determinada inmunoglobulina (anticuerpo).
- Si hay ciertos cambios genéticos
- Si el riñón está dañado.
- Si el cáncer responde al tratamiento inicial o recidiva (regresa).
Las opciones de tratamiento dependen de los siguientes factores:
- El tipo de neoplasia de células plasmáticas
- La edad y el estado de salud general del paciente
- Si hay signos, síntomas o problemas de salud, como insuficiencia renal o infección, relacionados con la enfermedad.
- Si el cáncer responde al tratamiento inicial o recidiva (regresa).
Estadios de las neoplasias de células plasmáticas
Puntos clave
- No existen sistemas de estadificación estándar para la gammapatía monoclonal de significado incierto (GMSI) y el plasmocitoma.
- Después del diagnóstico de mieloma múltiple, se realizan pruebas para determinar la extensión del cáncer en el cuerpo.
- La etapa del mieloma múltiple se basa en los niveles de beta-2-microglobulina y albúmina en la sangre.
- El mieloma múltiple se estadifica de la siguiente forma:
- Mieloma múltiple en estadio I
- Mieloma múltiple en estadio II
- Mieloma múltiple en estadio III
- Las neoplasias de células plasmáticas pueden no responder al tratamiento o reaparecer después de este.
No existen sistemas de estadificación estándar para la gammapatía monoclonal de significado incierto (GMSI) y el plasmocitoma.
Después del diagnóstico de mieloma múltiple, se realizan pruebas para determinar la extensión del cáncer en el cuerpo.
El proceso que se utiliza para determinar la cantidad de cáncer en el cuerpo se denomina estadificación. Es importante saber el estadio para planificar el tratamiento.
Las siguientes pruebas y procedimientos pueden usarse para determinar la extensión del cáncer en el cuerpo:
- Estudio de los huesos esqueléticos: en un estudio de los huesos esqueléticos, se toman radiografías de todos los huesos del cuerpo. Las radiografías se utilizan para encontrar áreas donde el hueso está dañado. Una radiografía es un tipo de haz de energía que puede atravesar el cuerpo y plasmarse en una película, lo que genera una imagen de las áreas internas del cuerpo.
- Resonancia magnética ( resonancia magnética ): procedimiento que utiliza un imán, ondas de radio y una computadora para generar una serie de imágenes detalladas de áreas internas del cuerpo, como la médula ósea . Este procedimiento también se denomina resonancia magnética nuclear (RMN).
- Densitometría ósea: procedimiento que utiliza un tipo especial de rayos X para medir la densidad ósea.
La etapa del mieloma múltiple se basa en los niveles de beta-2-microglobulina y albúmina en la sangre.
La beta-2-microglobulina y la albúmina se encuentran en la sangre. La beta-2-microglobulina es una proteína presente en las células plasmáticas. La albúmina constituye la mayor parte del plasma sanguíneo. Impide que el líquido se filtre fuera de los vasos sanguíneos. También aporta nutrientes a los tejidos y transporta hormonas, vitaminas, medicamentos y otras sustancias, como el calcio, por todo el cuerpo. En la sangre de pacientes con mieloma múltiple, la cantidad de beta-2-microglobulina aumenta y la de albúmina disminuye.
El mieloma múltiple se estadifica de la siguiente forma:
Mieloma múltiple en estadio I
En el mieloma múltiple en estadio I, los niveles en sangre son los siguientes:
- El nivel de beta-2-microglobulina es inferior a 3.5 mg/L.
- El nivel de albúmina es de 3,5 g/dL o superior.
Mieloma múltiple en estadio II
En el mieloma múltiple en estadio II, los niveles en sangre se encuentran entre los niveles del estadio I y el estadio III.
Mieloma múltiple en estadio III
En el mieloma múltiple en estadio III, el nivel en sangre de beta-2-microglobulina es de 5.5 mg/L o más y el paciente también presenta uno de los siguientes:
- Nivel alto de lactato deshidrogenasa (LDH)
- Ciertos cambios en los cromosomas
Las neoplasias de células plasmáticas pueden no responder al tratamiento o reaparecer después de este.
Las neoplasias de células plasmáticas se denominan refractarias cuando el número de células plasmáticas sigue aumentando a pesar de que se administra tratamiento. Las neoplasias de células plasmáticas se denominan recidivantes cuando han reaparecido después del tratamiento.
Treatment Option Overview
Puntos clave
- Existen diferentes tipos de tratamiento para los pacientes con neoplasias de células plasmáticas.
- The following types of treatment are used:
- Quimioterapia
- Otras terapias farmacológicas
- Terapia dirigida
- Quimioterapia de dosis alta con trasplante de células madre
- Inmunoterapia
- Radioterapia
- Cirugía
- Observación cuidadosa
- New types of treatment are being tested in clinical trials.
- Nuevas combinaciones de terapias
- El tratamiento de las neoplasias de células plasmáticas puede producir efectos secundarios.
- Se ofrece atención de apoyo para aliviar los problemas causados por la enfermedad o su tratamiento.
- Patients may want to think about taking part in a clinical trial.
- Patients can enter clinical trials before, during, or after starting their cancer treatment.
- Pueden ser necesarias pruebas de seguimiento.
Existen diferentes tipos de tratamiento para los pacientes con neoplasias de células plasmáticas.
Existen diferentes tipos de tratamientos disponibles para los pacientes con neoplasia de células plasmáticas. Algunos tratamientos son estándar (el tratamiento que se utiliza actualmente) y otros se están probando en ensayos clínicos. Un ensayo clínico de tratamiento es un estudio de investigación cuyo objetivo es ayudar a mejorar los tratamientos actuales u obtener información sobre nuevos tratamientos para pacientes con cáncer. Cuando los ensayos clínicos muestran que un nuevo tratamiento es mejor que el actual, este puede convertirse en estándar. Es posible que los pacientes deseen considerar participar en un ensayo clínico. Algunos ensayos clínicos están abiertos solo a pacientes que no han comenzado el tratamiento.
The following types of treatment are used:
Quimioterapia
La quimioterapia es un tratamiento contra el cáncer que utiliza medicamentos para detener el crecimiento de las células cancerosas, ya sea matándolas o impidiendo que se dividan. Cuando la quimioterapia se toma por vía oral o se inyecta en una vena o músculo, los medicamentos ingresan al torrente sanguíneo y pueden llegar a las células cancerosas de todo el cuerpo (quimioterapia sistémica).
Consulte la página de Medicamentos aprobados para el mieloma múltiple y otras neoplasias de células plasmáticas.
Otras terapias farmacológicas
Los corticosteroides son esteroides que tienen efectos antitumorales en el mieloma múltiple.
Terapia dirigida
La terapia dirigida es un tipo de tratamiento que utiliza medicamentos u otras sustancias para identificar y atacar células cancerosas específicas. Se pueden utilizar varios tipos de terapia dirigida para tratar el mieloma múltiple y otras neoplasias de células plasmáticas. Existen diferentes tipos de terapia dirigida:
- Terapia con inhibidores del proteasoma: este tratamiento bloquea la acción de los proteasomas en las células cancerosas. Un proteasoma es una proteína que elimina a otras que la célula ya no necesita. Cuando las proteínas no se eliminan de la célula, se acumulan y pueden provocar la muerte de la célula cancerosa. El bortezomib, el carfilzomib y el ixazomib son inhibidores del proteasoma utilizados en el tratamiento del mieloma múltiple y otras neoplasias de células plasmáticas.
- Anticuerpo monoclonal los anticuerpos monoclonales son proteínas del sistema inmunitario que se producen en el laboratorio para tratar muchas enfermedades, como el cáncer. Cuando se utiliza para tratar el cáncer, estos anticuerpos se adhieren a un objetivo específico en las células cancerosas u otras células que podrían estar causando el crecimiento del cáncer. De esta forma, los anticuerpos pueden eliminar las células cancerosas, bloquear su crecimiento o evitar que se propaguen. Los anticuerpos monoclonales son administrados por infusión. Pueden utilizarse solos o para transportar medicamentos, toxinaso radioactivo material directamente a las células cancerosas. daratumumab and elotuzumab son anticuerpos monoclonales utilizados en el tratamiento del mieloma múltiple y otras neoplasias de células plasmáticas. El denosumab es un anticuerpo monoclonal que se utiliza para retardar la pérdida ósea y reducir el dolor óseo en pacientes con mieloma múltiple.
- Terapia con inhibidores de BCL2: este tratamiento bloquea una proteína llamada BCL2. Este bloqueo puede ayudar a destruir las células cancerosas y aumentar su sensibilidad a los medicamentos para el cáncer. El venetoclax es un inhibidor de la BCL2 que se está estudiando para el tratamiento del mieloma múltiple recidivante o refractario.
Consulte la página de Medicamentos aprobados para el mieloma múltiple y otras neoplasias de células plasmáticas.
Quimioterapia de dosis alta con trasplante de células madre
Se administran dosis altas de quimioterapia para matar las células cancerosas. El tratamiento contra el cáncer también destruye las células sanas, incluidas las células productoras de sangre. El trasplante de células madre es un tratamiento para reemplazar las células productoras de sangre. Las células madre (células sanguíneas inmaduras) se extraen de la sangre o de la médula ósea del paciente (autólogas) o de un donante (alogénicas) y se congelan y almacenan. Una vez que el paciente completa la quimioterapia, las células madre almacenadas se descongelan y se devuelven al paciente mediante una infusión. Estas células madre reinfundidas crecen (y restauran) las células sanguíneas del cuerpo.
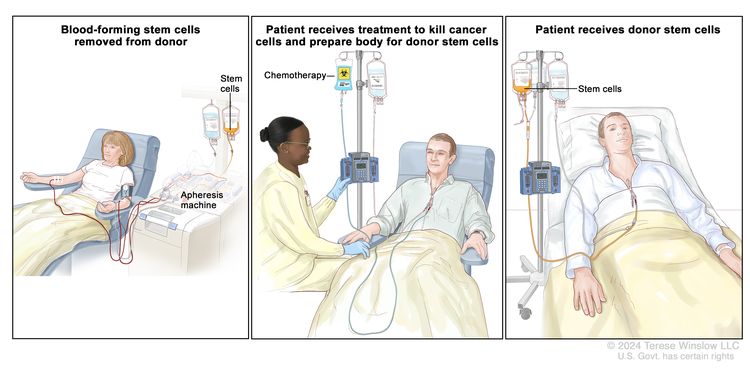
Trasplante de células madre de un donante. (Paso 1): Cuatro o cinco días antes de la recolección de células madre del donante, este recibe un medicamento para aumentar la cantidad de células madre que circulan por su torrente sanguíneo (no se muestra en la imagen). Las células madre hematopoyéticas se extraen del donante a través de una vena grande del brazo. La sangre fluye a través de una máquina de aféresis que extrae las células madre. El resto de la sangre se devuelve al donante a través de una vena del otro brazo. (Paso 2): El paciente recibe quimioterapia para destruir las células cancerosas y preparar su cuerpo para las células madre del donante. El paciente también puede recibir radioterapia (no se muestra en la imagen). (Paso 3): El paciente recibe una infusión de las células madre del donante.
Inmunoterapia
La inmunoterapia es un tratamiento que utiliza el sistema inmunológico del paciente para combatir el cáncer. Las sustancias producidas por el cuerpo o en un laboratorio se utilizan para estimular, dirigir o restaurar las defensas naturales del cuerpo contra el cáncer. Este tratamiento contra el cáncer es un tipo de terapia biológica.
- Terapia inmunomoduladora: la talidomida, la lenalidomida y la pomalidomida son inmunomoduladores que se usan para tratar el mieloma múltiple y otras neoplasias de células plasmáticas.
- Terapia con células CAR-T: este tratamiento cambia las células T (un tipo de célula del sistema inmunológico) del paciente para que ataquen ciertas proteínas en la superficie de las células cancerosas. Estas células se obtienen del paciente y se les añaden receptores especiales a su superficie en el laboratorio. Las células cambiadas se llaman (receptor de antígeno quimérico) ). Estas se cultivan en el laboratorio y se administran al paciente mediante infusión; se multiplican en la sangre del paciente y atacan a las células cancerosas. La terapia de células CAR-T está en estudio para el tratamiento del mieloma múltiple en recaída (recidivante).
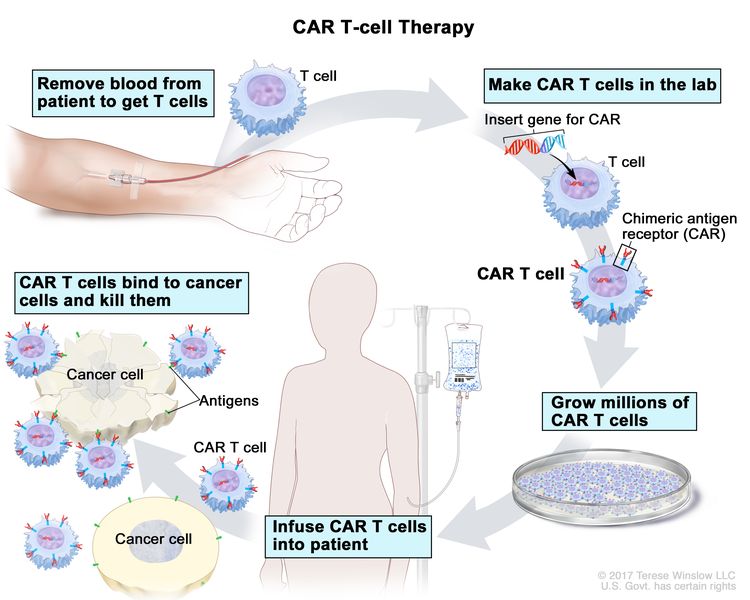
Terapia con células CAR-T: es un tratamiento en el que las células T del paciente (un tipo de célula inmunitaria) se modifican en el laboratorio para que se unan a las células cancerosas y las destruyan. La sangre del paciente fluye desde una vena del brazo a través de un tubo hacia una máquina de aféresis (no mostrada en el dibujo), que extrae los glóbulos blancos, incluidas las células T, y devuelve el resto de la sangre al paciente. En el laboratorio, se inserta un gen especial llamado receptor de antígeno quimérico (CAR) en las células T. Millones de estas células CAR-T se cultivan y se administran al paciente mediante una infusión. Una vez en el cuerpo, las células CAR-T se unen a un antígeno en las células cancerosas y las destruyen.
Consulte la página de Medicamentos aprobados para el mieloma múltiple y otras neoplasias de células plasmáticas.
Radioterapia
La radioterapia es un tratamiento contra el cáncer que utiliza rayos X de alta energía u otros tipos de radiación para matar las células cancerosas o evitar que crezcan. Para la radioterapia externa se usa una máquina que envía la radiación hacia la zona con cáncer desde el exterior del cuerpo.
Cirugía
Se puede realizar una cirugía para extirpar el tumor. Después de que el médico extirpe todo el cáncer visible al momento de la cirugía, algunos pacientes pueden recibir radioterapia para eliminar cualquier célula cancerosa restante. El tratamiento posterior a la cirugía, cuyo objetivo es reducir el riesgo de reaparición del cáncer, se denomina terapia adyuvante.
Observación cuidadosa
La observación cuidadosa consiste en monitorear de cerca el estado del paciente sin administrar ningún tratamiento hasta que aparezcan o cambien los signos o síntomas.
New types of treatment are being tested in clinical trials.
En esta sección se resumen los tratamientos que se están estudiando en ensayos clínicos. Es posible que no se mencionen todos los tratamientos nuevos que se están estudiando. La información sobre los ensayos clínicos está disponible en el sitio web del NCI.
Nuevas combinaciones de terapias
Los ensayos clínicos están estudiando diferentes combinaciones de inmunoterapia, quimioterapia, terapia con esteroides y medicamentos. También se están estudiando nuevos regímenes de tratamiento con selinexor.
El tratamiento de las neoplasias de células plasmáticas puede producir efectos secundarios.
For information about side effects caused by treatment for cancer, visit our Side Effects page.
Se ofrece atención de apoyo para aliviar los problemas causados por la enfermedad o su tratamiento.
Esta terapia controla los problemas o efectos secundarios causados por la enfermedad o su tratamiento y mejora la calidad de vida del paciente. Se ofrece atención de apoyo para tratar problemas causados por el mieloma múltiple y otras neoplasias de células plasmáticas.
La atención de apoyo pueden consistir en:
- Plasmaféresis: si la sangre se espesa debido a un exceso de anticuerpos e interfiere con la circulación, se realiza una plasmaféresis para eliminar el exceso de plasma y anticuerpos. En este procedimiento, se extrae sangre del paciente y se pasa por una máquina que separa el plasma (la parte líquida de la sangre) de las células sanguíneas. El plasma, que contiene los anticuerpos innecesarios, no se le devuelve. Las células sanguíneas normales se reintegran al torrente sanguíneo junto con el plasma donado o un sustituto. La plasmaféresis no impide la formación de nuevos anticuerpos.
- Terapia de inducción con trasplante de células madre: si se produce amiloidosis, el tratamiento puede consistir en terapia de inducción seguida de un trasplante de células madre utilizando las propias células madre del paciente.
- Inmunoterapia: la inmunoterapia con talidomida, lenalidomida o pomalidomida se administra para tratar la amiloidosis.
- Terapia dirigida: se administra terapia dirigida con inhibidores del proteasoma para disminuir la cantidad de inmunoglobulina M en la sangre y tratar la amiloidosis. La terapia dirigida con daratumumab se administra sola o en combinación con otros medicamentos para tratar la amiloidosis. También puede utilizarse un anticuerpo monoclonal como terapia dirigida para retardar la pérdida ósea y reducir el dolor.
- Radioterapia: se administra radioterapia para las lesiones óseas de la columna.
- Quimioterapia: la quimioterapia se administra para reducir el dolor de espalda causado por la osteoporosis o las fracturas por compresión de la columna.
- Terapia con bisfosfonatos: La terapia con bisfosfonatos se administra para frenar la pérdida ósea y reducir el dolor óseo. Para obtener más información sobre los bisfosfonatos y los problemas relacionados con su uso, consulte Complicaciones orales de las terapias contra el cáncer .
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Pueden ser necesarias pruebas de seguimiento.
A medida que avanza el tratamiento, se le realizarán pruebas o controles de seguimiento. Es posible que se repitan algunas pruebas para diagnosticar o estadificar el cáncer con el fin de evaluar cómo está funcionando el tratamiento. Las decisiones sobre si continuar, modificar o suspender el tratamiento pueden basarse en los resultados de estas pruebas.
Algunas pruebas seguirán realizándose de manera periódica después de terminar el tratamiento. Los resultados pueden indicar si su afección ha cambiado o si el cáncer ha redicivado (regresado).
Tratamiento de gammapatía monoclonal de significado indeterminado
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento de la gammapatía monoclonal de significado indeterminado (GMSI) suele consistir en la observación cuidadosa. Se realizarán análisis de sangre periódicos para verificar el nivel de proteína M en la sangre y reconocimientos físicos para detectar signos o síntomas de cáncer.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del plasmacitoma óseo aislado
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento del plasmocitoma óseo aislado suele ser radioterapia dirigida a la lesión ósea.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del plasmacitoma extramedular
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento del plasmocitoma extramedular puede consistir en:
- Radioterapia dirigida al tumor y a los ganglios linfáticos cercanos
- Cirugía, generalmente seguida de radioterapia
- Observación cuidadosa después del tratamiento inicial, seguida de radioterapia, cirugía o quimioterapia si el tumor crece o produce signos o síntomas.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del mieloma múltiple
For information about the treatments listed below, see the Treatment Option Overview section.
Es posible que los pacientes sin signos ni síntomas no necesiten tratamiento. Estos pacientes pueden permanecer en observación cuidadosa hasta que aparezcan signos o síntomas.
Cuando aparecen signos o síntomas, hay dos categorías de pacientes que reciben tratamiento:
- Pacientes más jóvenes y en buen estado físico que son candidatos a un trasplante de células madre.
- Pacientes mayores que no están en buen estado físico que no son candidatos a un trasplante de células madre.
Los pacientes menores de 65 años generalmente se consideran más jóvenes y en forma. Los pacientes mayores de 75 años no suelen ser elegibles para un trasplante de células madre. En el caso de los pacientes entre las edades de 65 y 75 años, el estado físico está determinado por su salud general y otros factores.
El tratamiento del mieloma múltiple suele realizarse en fases:
- Terapia de inducción: esta es la primera fase del tratamiento. Su objetivo es reducir la presencia de la enfermedad y puede incluir uno o más de los siguientes:
- Para pacientes más jóvenes y en forma (elegibles para un trasplante):
- Quimioterapia.
- Terapia dirigida con un inhibidor del proteasoma (bortezomib) y un anticuerpo monoclonal (daratumumab)
- Inmunoterapia (lenalidomida).
- Terapia con corticosteroides (dexametasona)
- Para pacientes mayores que no están en forma (no elegibles para un trasplante):
- Chemotherapy.
- Terapia dirigida con un inhibidor del proteasoma (bortezomib o carfilzomib) o un anticuerpo monoclonal (daratumumab)
- Inmunoterapia (lenalidomida)
- Terapia con corticosteroides (dexametasona)
- Para pacientes más jóvenes y en forma (elegibles para un trasplante):
- Terapia de consolidación: esta es la segunda fase del tratamiento. El tratamiento en la fase de consolidación consiste en eliminar cualquier resto de El cáncer células. Quimioterapia de dosis alta es seguido por:
- Un trasplante de células madre autólogo, en el que se utilizan las células madre de la sangre o la médula ósea del paciente.
- Dos trasplantes autólogos de células madre seguidos de un trasplante de células madre autólogo o alogénico, en el que el paciente recibe células madre de la sangre o la médula ósea de un donante.
- Un trasplante alogénico de células madre
- Terapia de mantenimiento: después del tratamiento inicial, la terapia de mantenimiento a menudo se administra para ayudar a mantener la enfermedad en remisión por más tiempo. Se están estudiando varios tipos de tratamiento para este uso, incluidos los siguientes:
- Chemotherapy.
- Inmunoterapia (lenalidomida)
- Terapia con corticosteroides (prednisona o dexametasona)
- Terapia dirigida con un inhibidor del proteasoma (bortezomib o ixazomib) o un anticuerpo monoclonal (daratumumab)
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del mieloma múltiple recidivante o refractario
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento del mieloma múltiple en recaída o refractario puede consistir en:
- Observación cuidadosa para pacientes cuya enfermedad se encuentre estable
- Un tratamiento diferente al ya administrado, para pacientes cuyo tumor siguió creciendo durante el tratamiento. Consulte las opciones de tratamiento del mieloma múltiple.
- Se pueden usar los mismos medicamentos utilizados antes de la recaída si esta se produce uno o más años después del tratamiento inicial. Consulte las opciones de tratamiento del mieloma múltiple.
Los medicamentos utilizados pueden ser los siguientes:
- Terapia dirigida con anticuerpos monoclonales (daratumumab, elotuzumab o isatuximab)
- Terapia dirigida con inhibidores del proteasoma (bortezomib, carfilzomib o ixazomib)
- Inmunoterapia (pomalidomida, lenalidomida o talidomida)
- Quimioterapia.
- Terapia con corticosteroides
- Ensayo clínico de terapia con células CAR-T
- Un ensayo clínico de terapia dirigida con un inhibidor de molécula pequeña (selinexor) y terapia con corticosteroides
- Un ensayo clínico de terapia dirigida con un inhibidor de BCL2 (venetoclax)
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Más información sobre las neoplasias de células plasmáticas
Para obtener más información del National Cancer Institute sobre el mieloma múltiple y otras neoplasias de células plasmáticas, consulte las siguientes páginas web:
- Página principal de mieloma múltiple/otras neoplasias de células plasmáticas
- Medicamentos aprobados para el mieloma múltiple y otras neoplasias de células plasmáticas
- Terapia dirigida para tratar el cáncer
- Trasplantes de células madre en el tratamiento del cáncer
- Immunotherapy to Treat Cancer
For general cancer information and other resources from the National Cancer Institute, visit:
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen del PDQ sobre el cáncer contiene información actualizada sobre el tratamiento de las neoplasias de células plasmáticas (incluido el mieloma múltiple). Su propósito es informar y ayudar a los pacientes, las familias y los cuidadores. No da pautas ni recomendaciones formales para tomar decisiones relacionadas con la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre tratamiento para adultos. Tratamiento de las neoplasias de células plasmáticas (incluido el mieloma múltiple) (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA].
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Fecha de actualización:
URL de origen: https://www.cancer.gov/node/5250/syndication
Agencia de origen: National Cancer Institute (NCI)
Captured Date: 2013-09-14 09:02:43.0