








Tratamiento del linfoma no Hodgkin
Obtenga una atención integral y compasiva para el linfoma no Hodgkin pediátrico (un tipo de cáncer que afecta el sistema linfático, parte del sistema inmunitario) en el Montefiore Einstein Comprehensive Cancer Center de Children’s Hospital at Montefiore Einstein (CHAM). El CHAM es un hospital pediátrico académico de primer nivel, reconocido en todo el país por su excelencia clínica y sus investigaciones innovadoras. Familias del área metropolitana de Nueva York, del país y del mundo confían en nosotros para que sus hijos reciban los tratamientos del cáncer más avanzados en un entorno de apoyo y cuidado.
Ofrecemos una gama completa de tratamientos para el linfoma no Hodgkin, incluidas opciones como la terapia de células CAR-T y el trasplante de células madre, para cánceres difíciles de tratar y cánceres recidivantes. Para ofrecer la mejor atención posible, hemos reunido un equipo de médicos, especialistas y personal de apoyo excepcionales, con algunos de los expertos más destacados del país en trasplante de médula ósea (TMO) pediátrico. Nuestro programa de TMO está certificado por la Fundación para la Acreditación de Terapia Celular y el Programa Nacional de Donantes de Médula Ósea. Además, el CHAM es miembro activo del Consorcio de Trasplante de Sangre y Médula Ósea Pediátrica, el Grupo de Oncología Infantil y el Centro de Investigación Internacional de Trasplante de Sangre y Médula Ósea.
Nuestros esfuerzos de investigación están destinados a probar nuevas terapias prometedoras y los ensayos clínicos ofrecen las opciones de tratamiento más avanzadas y actualizadas.
Si lo que usted desea es lo mejor para su hijo, acuda a los especialistas del Centro Oncológico Integral Montefiore Einstein en CHAM, quienes se dedican con pasión a erradicar el cáncer y a atender todas las necesidades de salud de su hijo.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Tratamiento del linfoma no Hodgkin infantil (PDQ®): versión para pacientes
Información general sobre el linfoma no Hodgkin infantil
Puntos clave
- El linfoma no Hodgkin infantil es una enfermedad por la que se forman células malignas (cancerosas) en el sistema linfático, que es una parte del sistema inmunitario del cuerpo.
- Hay tres tipos principales de linfoma no Hodgkin infantil.
- Linfoma no Hodgkin de células B maduras agresivo
- Linfoma linfoblástico
- Linfoma anaplásico de células grandes
- Algunos tipos de linfoma no Hodgkin son poco frecuentes en niños.
- Tener el sistema inmunitario debilitado aumenta el riesgo de linfoma no Hodgkin en los niños.
- Entre los síntomas del linfoma no Hodgkin infantil se incluyen problemas para respirar y ganglios linfáticos inflamados.
- Para diagnosticar y estadificar el linfoma no Hodgkin infantil, se utilizan pruebas que examinan el cuerpo y el sistema linfático.
- Es posible que quiera una segunda opinión para confirmar el diagnóstico de cáncer de su hijo o hija.
- Hay ciertos factores que afectan al pronóstico (probabilidad de recuperación) y a las opciones de tratamiento.
El linfoma no Hodgkin infantil es una enfermedad por la que se forman células malignas (cancerosas) en el sistema linfático, que es una parte del sistema inmunitario del cuerpo.
El sistema inmunológico protege al cuerpo de infecciones y enfermedades.
El sistema linfático se compone de las siguientes partes:
- Linfa: líquido acuoso e incoloro que recorre los Vasos linfaticos y transporta los linfocitos (glóbulos blancos).
- Los linfocitos B, también llamados células B, producen anticuerpos para combatir las infecciones. La mayoría de los linfomas no Hodgkin se originan en los linfocitos B.
- Los linfocitos T, también llamados células T, ayudan a los linfocitos B a producir los anticuerpos que ayudan a combatir las infecciones.
- Los linfocitos citolíticos naturales, también llamadas células NK, atacan las células cancerosas y los virus.
- Vasos linfáticos: red de tubos delgados que recogen la linfa de diferentes partes del cuerpo y la devuelven al torrente sanguíneo.
- Ganglios linfáticos: estructuras pequeñas en forma de frijol que filtran la linfa y almacenan glóbulos blancos que ayudan a combatir infecciones y enfermedades. Los ganglios linfáticos se encuentran a lo largo de la red de vasos linfáticos por todo el cuerpo. Hay grupos de ganglios linfáticos en el cuello, la axila, el mediastino (el área entre los pulmones), el abdomen, la pelvis y la ingle.
- Bazo: órgano que produce linfocitos, almacena glóbulos rojos y linfocitos, filtra la sangre y destruye los glóbulos sanguíneos viejos. El bazo se encuentra en el lado izquierdo del abdomen, cerca del estómago.
- Timo: órgano en el que los linfocitos T maduran y se multiplican. El timo está en el tórax detrás del esternón.
- Amígdalas: son dos pequeñas masas de tejido linfático en la parte posterior de la garganta. Hay una amígdala a cada lado de la garganta.
- Médula ósea: tejido blando y esponjoso que se encuentra en el centro de ciertos huesos, como el de la cadera y el esternón. Los glóbulos blancos, los glóbulos rojos y las plaquetas se producen en la médula ósea.
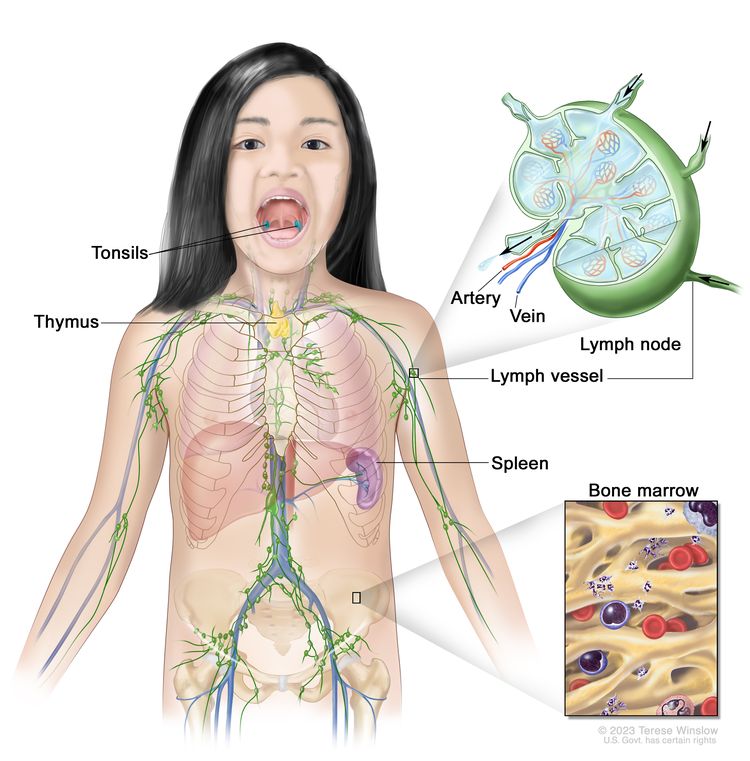
El sistema linfático forma parte del sistema inmunitario y está compuesto por tejidos y órganos que ayudan a proteger al cuerpo de infecciones y enfermedades, entre ellos, las amígdalas, el timo, el bazo, la médula ósea, los vasos linfáticos y los ganglios linfáticos. La linfa (líquido transparente y acuoso) y los linfocitos (glóbulos blancos) circulan por los vasos linfáticos hasta llegar a los ganglios linfáticos, donde destruyen las sustancias nocivas. La linfa ingresa al torrente sanguíneo a través de una vena grande cerca del corazón.
El tejido linfático también se encuentra en otras partes del cuerpo, como el estómago, la glándula tiroidea, el cerebro y la piel.
El linfoma no Hodgkin puede comenzar en los linfocitos B, en los linfocitos T o en los linfocitos citolíticos naturales.
Existen dos tipos generales de linfomas: linfoma de Hodgkin y linfoma no Hodgkin. En este resumen se describe el tratamiento del linfoma no Hodgkin infantil. Obtenga información sobre el Tratamiento del linfoma de Hodgkin infantil.
El tratamiento del linfoma no Hodgkin es diferente para niños y adultos. Para obtener información sobre el tratamiento en adultos, los siguientes sitios web:
Hay tres tipos principales de linfoma no Hodgkin infantil.
El tipo de linfoma se determina por el aspecto de las células al microscopio. Los tres tipos principales de linfoma no Hodgkin infantil son los siguientes:
Linfoma no Hodgkin de células B maduras agresivo
Los linfomas no Hodgkin de células B maduras agresivos incluyen los siguientes tipos:
- Linfoma de Burkitt: se trata de un cáncer agresivo (de crecimiento rápido) que se desarrolla a partir de los linfocitos B y es más común en niños, adolescentes y adultos jóvenes. Se forma en el abdomen, El anillo de Waldeyer, los testículos, los huesos, la médula ósea, la piel o el sistema nervioso central (SNC).
Se ha establecido una relación entre el linfoma de Burkitt y la infección por el virus de Epstein-Barr (VEB). Es más común en personas blancas que en hispanas. Se diagnostica cuando se analiza una muestra de tejido y se detecta una mutación específica en el gen MYC.
- Linfoma difuso de células B grandes: es el tipo más común de linfoma no Hodgkin. Se trata de un tipo de linfoma no Hodgkin de células B de crecimiento rápidamente en los ganglios linfáticos. También suele afectar el bazo, el hígado, la médula ósea u otros órganos. El linfoma difuso de células B grandes se presenta con mayor frecuencia en adolescentes que en niños.
- Linfoma mediastínico primario de células B: tipo de linfoma que se desarrolla a partir de las células B en el mediastino (la zona entre los pulmones). Puede propagarse a órganos cercanos, como los pulmones y la membrana que rodea el corazón. También puede propagarse a los ganglios linfáticos y órganos alejados, como los riñones. El linfoma mediastínico primario de células B se presenta más frecuentemente en adolescentes mayores que en niños.
Linfoma linfoblástico
El linfoma linfoblástico es un tipo de linfoma que afecta principalmente a los linfocitos T. Generalmente se forma en el mediastino (la zona entre los pulmones). Esto causa dificultad para respirar, sibilancias, dificultad para tragar o hinchazón de la cabeza y el cuello. Puede extenderse a los ganglios linfáticos, los huesos, la médula ósea, la piel, el sistema nervioso central (SNC), los órganos abdominales y otras áreas. El linfoma linfoblástico es muy similar a la leucemia linfoblástica aguda (LLA).
Linfoma anaplásico de células grandes
El linfoma anaplásico de células grandes es un tipo de linfoma que afecta sobre todo a los linfocitos T. Generalmente se forma en los ganglios linfáticos, la piel o los huesos, y a veces se forma en el tracto gastrointestinal, los pulmones, el tejido que recubre los pulmones y los músculos. Los pacientes con linfoma anaplásico de células grandes tienen un receptor llamado CD30 en la superficie de las células T. En muchos niños, el linfoma anaplásico de células grandes se caracteriza por cambios en el gen ALK, que produce una proteína llamada quinasa del linfoma anaplásico. Un patólogo analiza estos cambios celulares y genéticos para ayudar a diagnosticar el linfoma anaplásico de células grandes.
Algunos tipos de linfoma no Hodgkin son poco frecuentes en niños.
Algunos tipos de linfoma no Hodgkin infantil son menos comunes. Estos incluyen:
- Linfoma folicular de tipo pediátrico: en los niños, el linfoma folicular se presenta con mayor frecuencia en los varones. Es más probable que se encuentre en un área y no se disemine a otras partes del cuerpo. Suele formarse en las amígdalas y los ganglios linfáticos del cuello, pero también puede formarse en los testículos, los riñones, el tracto gastrointestinal y la glándula parótida.
- Linfoma de zona marginal: tipo de linfoma que tiende a crecer y propagarse lentamente, por lo que suele detectarse en un estadio temprano. Puede encontrarse en los ganglios linfáticos o en áreas fuera de ellos. El linfoma de zona marginal que se encuentra fuera de los ganglios linfáticos en niños se denomina linfoma de tejido linfoide asociado a mucosas (MALT). Este tipo de linfoma a veces se asocia con una infección por Helicobacter pylori en el tubo digestivo o una infección por Chlamydophila psittaci en la membrana conjuntiva que recubre los ojos. El linfoma de zona marginal es poco frecuente en niños y adultos.
- Linfoma primario del sistema nervioso central (SNC): se trata de un linfoma muy poco frecuente en niños. La mayoría de los linfomas primarios del SNC son linfomas difusos de células B grandes.
- Linfoma periférico de células T: el linfoma periférico de células T es un linfoma no Hodgkin agresivo (de crecimiento rápido) que se origina en los linfocitos T maduros. Otros tipos de linfoma periférico de células T incluyen el linfoma de células T maduras/linfocitos citolíticos naturales, el linfoma extranodal de células NK/T y el linfoma hepatoesplénico de células T gamma-delta. El linfoma periférico de células T es poco frecuente en niños.
- Linfoma cutáneo de células T: se origina en la piel y puede causar engrosamiento o la formación de un tumor. Es muy infrecuente en niños, pero es más común en adolescentes y adultos jóvenes. Hay diferentes tipos de linfoma cutáneo de células T, como el linfoma anaplásico de células grandes cutáneo, el linfoma subcutáneo de células T similar a la paniculitis, el linfoma de células T gamma-delta, la micosis fungoide y la papulosis linfomatoide. La micosis fungoide casi nunca se presenta en niños y adolescentes.
Tener el sistema inmunitario debilitado aumenta el riesgo de linfoma no Hodgkin en los niños.
Cualquier cosa que aumenta la probabilidad de tener una enfermedad es un factor de riesgo. No todos los niños con uno o más de estos factores de riesgo desarrollarán linfoma no Hodgkin (LNH), y algunos niños sin factores de riesgo conocidos desarrollarán la enfermedad.
Los siguientes son algunos de los problemas del sistema inmunitario que pueden aumentar el riesgo de LNH infantil:
- Una infección por el virus de Epstein-Barr o por el VIH
- Un sistema inmunológico debilitado después de un trasplante o por los medicamentos administrados después de un trasplante
- Ciertas enfermedades hereditarias (como los síndrome de deficiencia en la reparación del ADN, que incluyen la ataxia-telangiectasia, el síndrome de rotura de Nijmegen y la deficiencia en la reparación de errores de emparejamiento constitucionales)
- Tratamientos anteriores contra el cáncer
Si el linfoma o la enfermedad linfoproliferativa se relaciona con un sistema inmunitario débil a ciertas enfermedades hereditarias, la infección por el VIH, un trasplante o medicamentos administrados luego de un trasplante, la afección se denomina enfermedad linfoproliferativa asociada a la inmunodeficiencia. Los diferentes tipos de enfermedad linfoproliferativa asociada a la inmunodeficiencia incluyen:
- Enfermedad linfoproliferativa relacionada con inmunodeficiencia primaria
- Linfoma no Hodgkin asociado al VIH
- Enfermedad linfoproliferativa postrasplante
- Enfermedad linfoproliferativa a causa de la quimioterapia
Hable con el médico de su hijo si cree que su hijo puede estar en riesgo.
Entre los síntomas del linfoma no Hodgkin infantil se incluyen problemas para respirar y ganglios linfáticos inflamados.
Los síntomas del linfoma no Hodgkin infantil dependen de la zona del cuerpo donde se origina el cáncer. Consulte con el médico si su hijo o hija tiene alguno de los siguientes signos o síntomas:
- dificultad para respirar
- sibilancias
- Tos
- Ruidos agudos al respirar
- Hinchazón en la cabeza, el cuello, la parte superior del cuerpo o los brazos
- dificultad para tragar
- Hinchazón indolora de los ganglios linfáticos en el cuello, las axilas, el estómago o la ingle
- Hinchazón o bulto indoloro en un testículo
- Fiebre sin razón conocida
- Pérdida de peso sin causa aparente
- Sudores nocturnos excesivos
- dolor o hinchazón en el abdomen
- Debilidad, entumecimiento o dolor en la espalda o las piernas
- Un cambio en el control de los intestinos o la vejiga
- dolor de huesos o articulaciones
- Fatiga
La causa de estos síntomas podría no ser un linfoma no Hodgkin. La única forma de saberlo es consultar con el médico de su hijo o hija.
Para diagnosticar y estadificar el linfoma no Hodgkin infantil, se utilizan pruebas que examinan el cuerpo y el sistema linfático.
Si el niño presenta síntomas que sugieren un linfoma no Hodgkin, el médico deberá determinar si se deben a cáncer u a otro problema. El médico le preguntará sobre el comienzo y la frecuencia de los síntomas. También le preguntará sobre el historial de salud personal y familiar de su hijo o hija y le hará un reconocimiento físico. Dependiendo de estos resultados, podría recomendar otras pruebas. Si al niño le diagnostican linfoma no Hodgkin, los resultados de las pruebas ayudarán a planificar el tratamiento.
Las siguientes son algunas de las pruebas utilizadas para diagnosticar y estadificar el linfoma no Hodgkin:
- Los estudios bioquímicos de la sangre utilizan una muestra de sangre para medir la cantidad de ciertas sustancias que los órganos y tejidos del cuerpo liberan en la sangre, como electrolitos, lactato deshidrogenasa (LDH), ácido úrico, nitrógeno ureico sanguíneo (NUS), creatinina y valores de la función hepática. Una cantidad anormal de una sustancia puede ser un signo de enfermedad.
- Las pruebas del funcionamiento hepático miden la cantidad de ciertas sustancias que el hígado libera en la sangre. Una cantidad superior a la normal de una sustancia puede ser un signo de cáncer.
- Tomografía computarizada (TC) utiliza una computadora conectada a una máquina de rayos X para generar una serie de imágenes detalladas de áreas internas del cuerpo, como el cuello, el tórax, el abdomen y la pelvis. Las imágenes se toman desde diferentes ángulos y se utilizan para crear vistas tridimensionales de tejidos y órganos. Se puede administrar un tinte que se inyecta por vía intravenosa o se ingiere para que los órganos o tejidos se vean con mayor claridad. Este procedimiento también se denomina tomografía computadorizada, tomografía computarizadao tomografía axial computarizada. Obtenga más información sobre Tomografía computarizada para el cáncer.
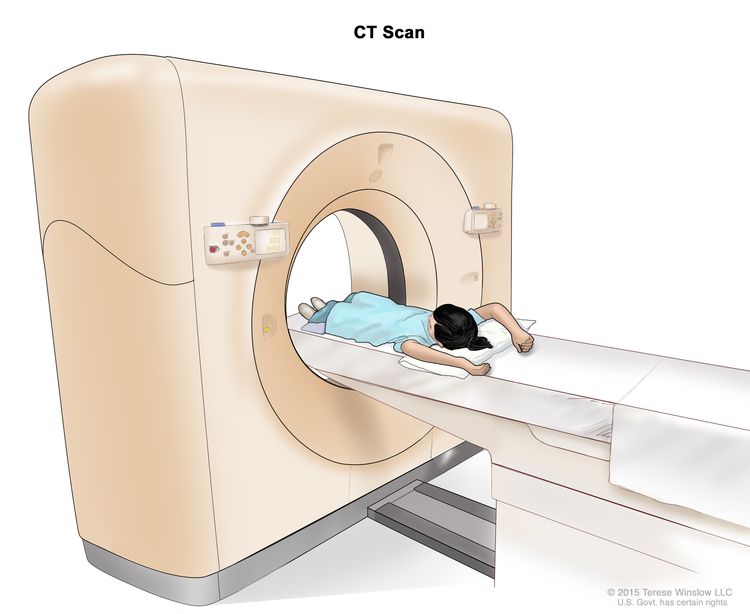
Tomografía computarizada (TC): el niño se recuesta sobre una camilla que se desliza a través del escáner, el cual toma una serie de radiografías detalladas de zonas internas del cuerpo.
- Tomografía por emisión de positrones (PET) utiliza una pequeña cantidad de radioactivo Azúcar (también llamada glucosa radiactiva) que se inyecta en una vena. El escáner PET gira alrededor del cuerpo y toma imágenes de las áreas internas donde el cuerpo utiliza el azúcar. Las células cancerosas se ven más brillantes en las imágenes porque son más activas y absorben más azúcar que las células normales. En ocasiones, se realizan simultáneamente una PET y una tomografía computarizada.
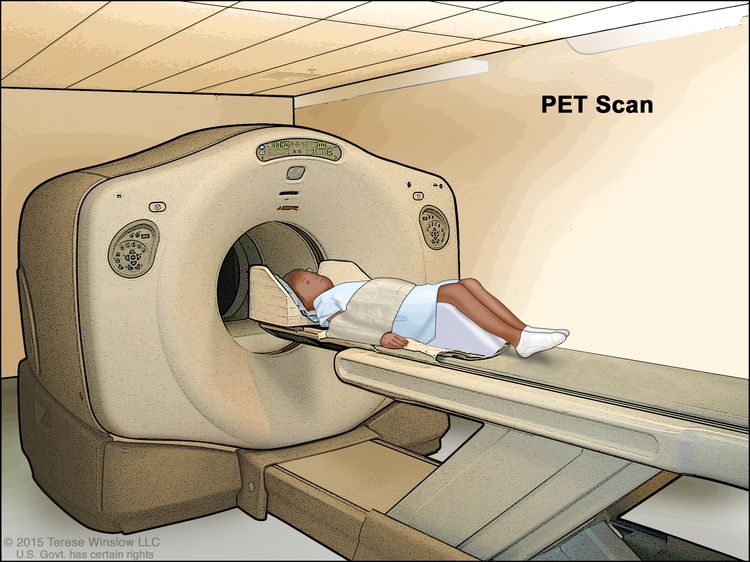
Tomografía por emisión de positrones (PET, por sus siglas en inglés): el niño se recuesta sobre una camilla que se desliza a través del escáner PET. El reposacabezas y la correa blanca ayudan al niño a permanecer inmóvil. Se inyecta una pequeña cantidad de glucosa radiactiva (azúcar) en la vena del niño y el escáner genera una imagen de las zonas del cuerpo donde se utiliza la glucosa. Las células cancerosas se ven más brillantes en la imagen porque absorben más glucosa que las células normales.
- Imágenes por resonancia magnética (IRM): se utiliza un imán, ondas de radio y una computadora para generar una serie de imágenes detalladas de áreas internas del cuerpo. Este procedimiento también se denomina resonancia magnética nuclear (RMN).
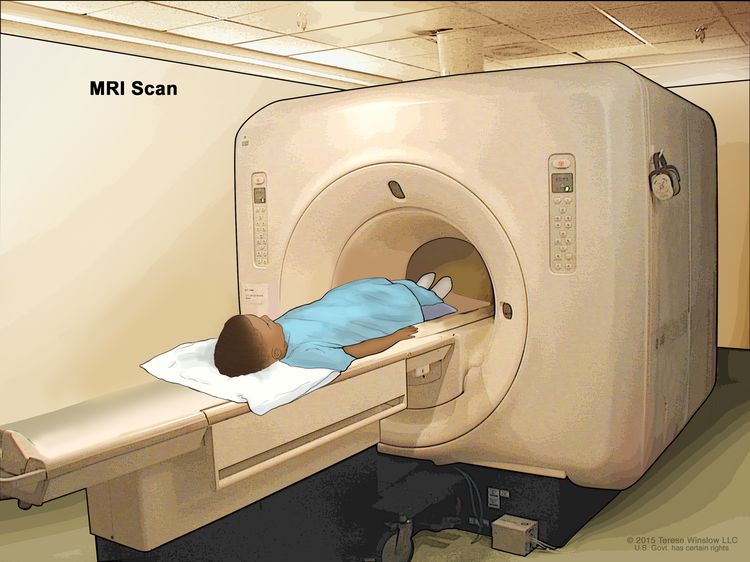
Resonancia magnética (RM): el niño se recuesta en una camilla que se desliza a través del equipo de resonancia magnética, que toma una serie de imágenes detalladas del interior del cuerpo. La posición del niño en la camilla depende de la parte del cuerpo que se va a examinar.
- Punción lumbar es un procedimiento utilizado para recolectar una muestra de líquido cefalorraquídeo (LCR) de la columna vertebral. Esto se hace colocando una aguja entre dos huesos de la columna vertebral y en el revestimiento alrededor de la médula espinal Para extraer una muestra de LCR, se examina la muestra al microscopio para detectar cáncer.
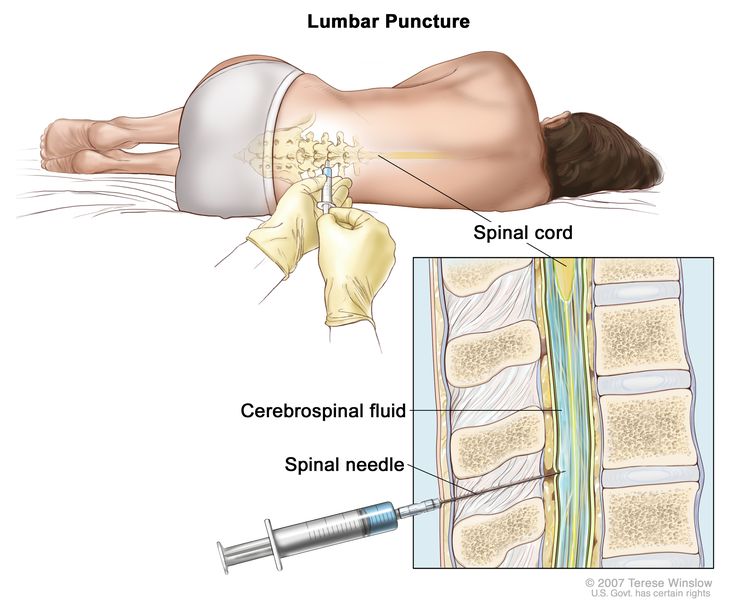
Punción lumbar. El paciente se recuesta en una camilla. Tras adormecer una pequeña zona de la parte baja de la espalda, se inserta una aguja espinal (una aguja larga y delgada) en la parte inferior de la columna vertebral para extraer líquido cefalorraquídeo (LCR, mostrado en azul). El líquido puede enviarse a un laboratorio para su análisis.
- Chest x-ray is a type of radiation that can go through the body and make pictures of the organs and bones inside the chest.
- Ecografía usa ondas de sonido de alta energía (ultrasonidos) que rebotan en los tejidos u órganos internos y producen ecos. Estos ecos forman una imagen de los tejidos corporales llamada ecograma.
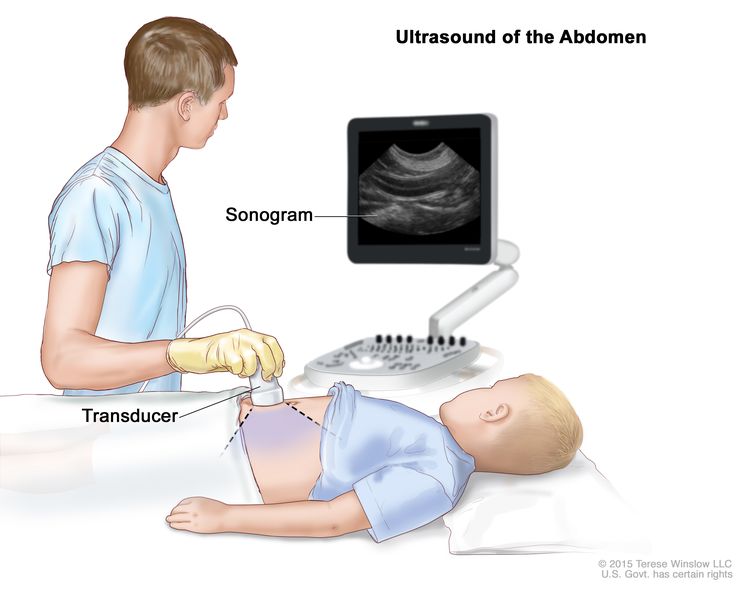
Ultrasonido abdominal: se presiona un transductor de ultrasonido conectado a una computadora contra la piel del abdomen. El transductor hace rebotar ondas de sonido en los órganos y tejidos internos para producir ecos que forman un ecograma (imagen de computadora).
- Biopsia es la extracción de una muestra de células o tejido del tumor para que el patólogo pueda observarlo bajo un microscopio y comprobar si hay cáncer.
Se pueden realizar uno de los siguientes tipos de biopsias:
El procedimiento que se use para extraer la muestra de tejido dependerá de la parte del cuerpo donde se encuentra el tumor.
- Aspiración y biopsia de médula ósea extrae médula ósea y un trozo de hueso insertando una aguja hueca en el hueso de la cadera o esternón. Un patólogo examina la médula ósea y el hueso bajo un microscopio para buscar signos de cáncer.
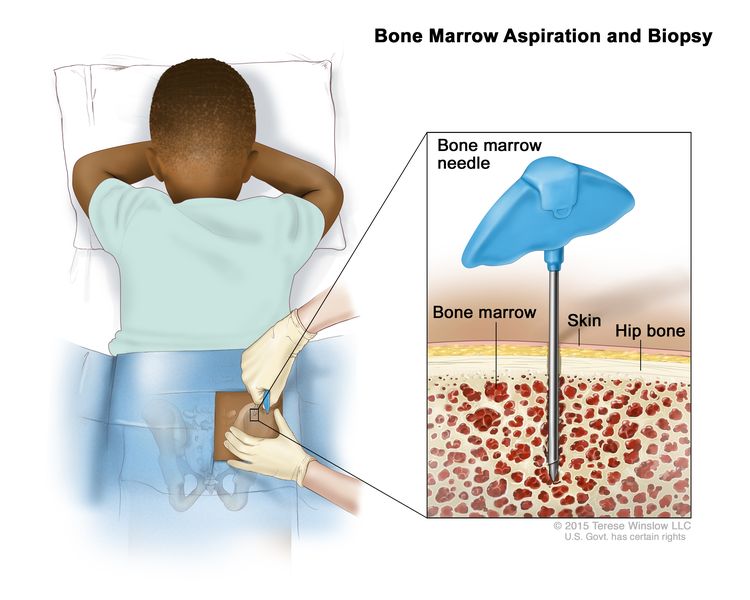
Aspiración y biopsia de médula ósea: tras anestesiar una pequeña zona de la piel, se introduce una aguja para médula ósea en el hueso de la cadera del niño. Se extraen muestras de sangre, hueso y médula ósea para examinarlas con un microscopio.
- La mediastinoscopia es un procedimiento quirúrgico para examinar los órganos, tejidos y ganglios linfáticos entre los pulmones en busca de áreas anómalas. Se realiza una incisión en la parte superior del esternón y se inserta un mediastinoscopio en el tórax. Un mediastinoscopio es un instrumento delgado, similar a un tubo, con una luz y una lente para observar. También cuenta con una herramienta para extraer muestras de tejido o ganglios linfáticos, que se examinan al microscopio para detectar cáncer.
- La mediastinotomía anterior es un procedimiento quirúrgico para examinar los órganos y tejidos ubicados entre los pulmones y entre el esternón y el corazón en busca de áreas anómalas. Se realiza una incisión junto al esternón y se inserta un mediastinoscopio en el tórax. Un mediastinoscopio es un instrumento delgado, similar a un tubo, con una luz y una lente para observar. También cuenta con una herramienta para extraer muestras de tejido o ganglios linfáticos, que se examinan al microscopio para detectar cáncer. Este procedimiento también se llama procedimiento de Chamberlain.
- La toracocentesis consiste en extraer el líquido que se encuentra en el espacio entre el revestimiento del tórax y el pulmón mediante una aguja. Un patólogo observa el líquido al microscopio para detectar células cancerosas.
Si se detecta cáncer, se pueden realizar las siguientes pruebas para analizar las células cancerosas:
- La prueba inmunohistoquímica utiliza anticuerpos para detectar ciertos antígenos (marcadores) en una muestra de células o tejido de un paciente. Por lo general, los anticuerpos se unen a una enzima o a un tinte fluorescente. Una vez que los anticuerpos se unen a un antígeno específico en la muestra de tejido, la enzima o el tinte se activan y se observa el antígeno al microscopio. Este tipo de prueba se usa para diagnosticar el cáncer y diferenciarlo de otros tipos de cáncer.
- La citometría de flujo se usa para medir el número de células de una muestra, el porcentaje de células vivas de una muestra y determinar ciertas características de las células, como el tamaño, la forma y la presencia de marcadores tumorales (o de otro tipo) en la superficie celular. Las células de una muestra de sangre, médula ósea u otro tejido del paciente se tiñen con un tinte sensible a la luz y se colocan en un líquido. Luego, se pasan estas células, de en una, por un rayo de luz. Los resultados de la prueba dependen de la forma en que las células con el tinte reaccionan frente al rayo de luz. Esta prueba se usa para diagnosticar y tratar ciertos tipos de cáncer, como la leucemia y el linfoma.
- El análisis citogenético examina los cromosomas de las células en una muestra de médula ósea, sangre, tumor u otro tejido para detectar cromosomas rotos, en otro orden, faltantes o sobrantes. Los cambios en ciertos cromosomas pueden ser un signo de cáncer. El análisis citogenético se utiliza para diagnosticar el cáncer, planificar el tratamiento o determinar su eficacia.
- La hibridación fluorescente in situ (FISH) examina y cuenta los genes o los cromosomas en las células y los tejidos. En el laboratorio, se preparan trozos de ADN con un tinte fluorescente que se agregan a una muestra de células o tejidos de un paciente. Cuando se observan al microscopio con una luz especial, estos trozos de ADN brillan si se unen a genes o áreas específicas de los cromosomas en la muestra. La prueba FISH se usa para diagnosticar el cáncer y planificar el tratamiento.
- En la inmunofenotipificación se utilizan anticuerpos para identificar células cancerosas según los tipos de antígenos o marcadores presentes en su superficie. Esta prueba se utiliza para diagnosticar tipos específicos de linfoma.
Es posible que quiera una segunda opinión para confirmar el diagnóstico de cáncer de su hijo o hija.
Quizás quiera una segunda opinión para confirmar el diagnóstico y el plan de tratamiento de su hijo o hija. Si busca una segunda opinión, deberá obtener los resultados de las pruebas médicas y los informes del primer médico para mostrárselos al segundo. Este revisará el informe de patología, las diapositivas y las exploraciones. Tal vez, el segundo médico esté de acuerdo con el primero, sugiera cambios en el plan de tratamiento o proporcione más información sobre el cáncer de su hijo o hija.
Para más información sobre cómo elegir un médico y obtener una segunda opinión, visite Búsqueda de tratamiento para el cáncer. Si se comunica con el Servicio de Información sobre de Cáncer del NCI por chat, correo electrónico o teléfono (en inglés y español), obtendrá ayuda para encontrar un médico u hospital que pueda ofrecerle una segunda opinión. Si tiene alguna pregunta que desee hacer en las citas con el médico de su hijo o hija, visite Preguntas para el médico sobre el cáncer.
Hay ciertos factores que afectan al pronóstico (probabilidad de recuperación) y a las opciones de tratamiento.
Si a su hijo o hija le han diagnosticado linfoma no Hodgkin, probablemente tenga preguntas sobre la gravedad del cáncer y las posibilidades de supervivencia. La evolución o curso probable de una enfermedad se llama pronóstico.
El pronóstico depende de:
- El tipo de linfoma
- El lugar del cuerpo donde está el tumor al momento del diagnóstico
- El estadio del cáncer
- La presencia de ciertos cambios en los cromosomas
- El tipo de tratamiento inicial
- La respuesta del linfoma al tratamiento inicial
- La edad y el estado general de salud del niño
No hay dos personas iguales y la respuesta al tratamiento puede variar considerablemente. El equipo de atención médica del cáncer de su hijo o hija es el más indicado para hablar con usted sobre el pronóstico.
Estadios del linfoma no Hodgkin infantil
Puntos clave
- Una vez diagnosticado el linfoma no Hodgkin infantil, se realizan pruebas para determinar si las células cancerosas se han extendido dentro del sistema linfático o a otras partes del cuerpo.
- Se utilizan los siguientes estadios para describir el linfoma no Hodgkin infantil:
- Estadio I
- Estadio II
- Estadio III
- Estadio IV
- A veces, el linfoma no Hodgkin infantil no responde al tratamiento o recidiva (vuelve) después del tratamiento.
Una vez diagnosticado el linfoma no Hodgkin infantil, se realizan pruebas para determinar si las células cancerosas se han extendido dentro del sistema linfático o a otras partes del cuerpo.
El estadio del cáncer describe la extensión del cáncer en el cuerpo, por ejemplo, el tamaño del tumor, si se propagó y qué tan lejos se propagó desde donde se originó. Es importante conocer el estadio del linfoma no Hodgkin para planificar el mejor tratamiento.
Para obtener una descripción de las pruebas y procedimientos utilizados para diagnosticar el linfoma no Hodgkin, consulte la sección de Información general.
Se utilizan los siguientes estadios para describir el linfoma no Hodgkin infantil:
Estadio I
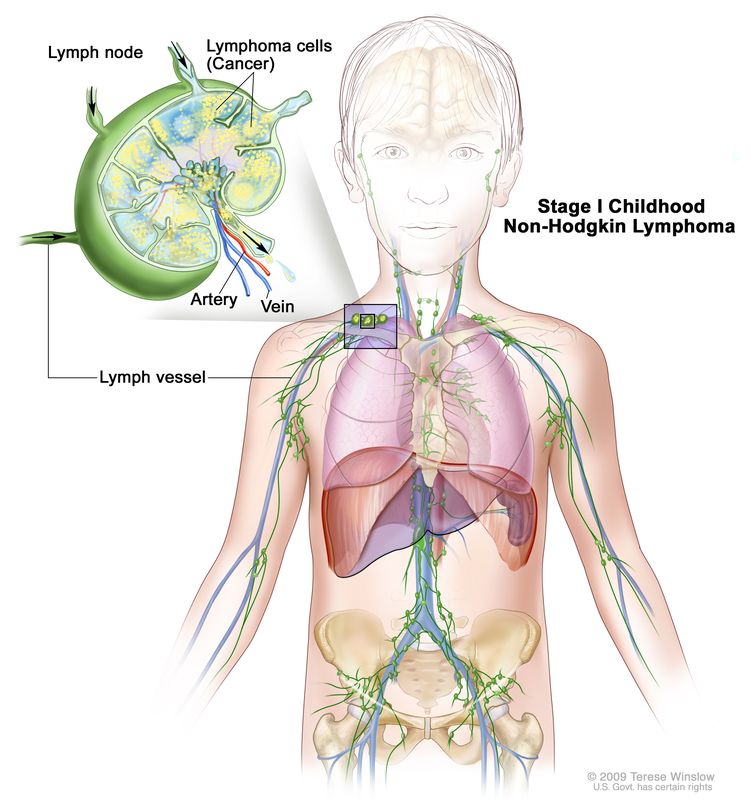
Linfoma no Hodgkin infantil en estadio I. Se encuentra cáncer en un grupo de ganglios linfáticos o en un área fuera de los ganglios linfáticos, pero no en el abdomen ni en el mediastino (zona entre los pulmones).
En el linfoma no Hodgkin infantil en estadio I, se encuentra cáncer en uno de los siguientes sitios:
- Un grupo de ganglios linfáticos
- Un área fuera de los ganglios linfáticos
No se encuentra cáncer en el abdomen ni en el mediastino (área entre los pulmones).
Estadio II
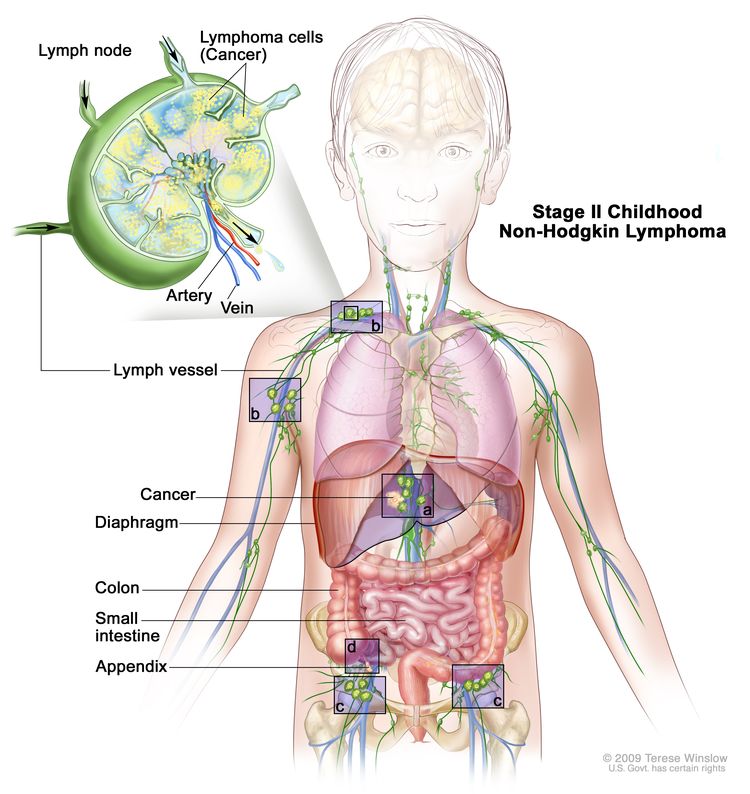
Linfoma no Hodgkin infantil en estadio II. El cáncer se encuentra en una zona fuera de los ganglios linfáticos y en los ganglios linfáticos adyacentes (a); o en dos o más zonas por encima (b) o por debajo (c) del diafragma; o el cáncer se originó en el estómago, el apéndice o los intestinos (d) y puede extirparse quirúrgicamente.
En el linfoma no Hodgkin infantil en estadio II, se presenta una de las siguientes situaciones:
- Se encuentra cáncer en un área fuera de los ganglios linfáticos y en los ganglios linfáticos cercanos.
- Se encuentra cáncer en dos o más áreas por encima o debajo del diafragma, y es posible que se haya diseminado a los ganglios linfáticos cercanos.
- El cáncer se originó en el estómago o los intestinos y se puede extirpar por completo mediante cirugía. El cáncer puede haberse propagado a algunos ganglios linfáticos cercanos.
Estadio III
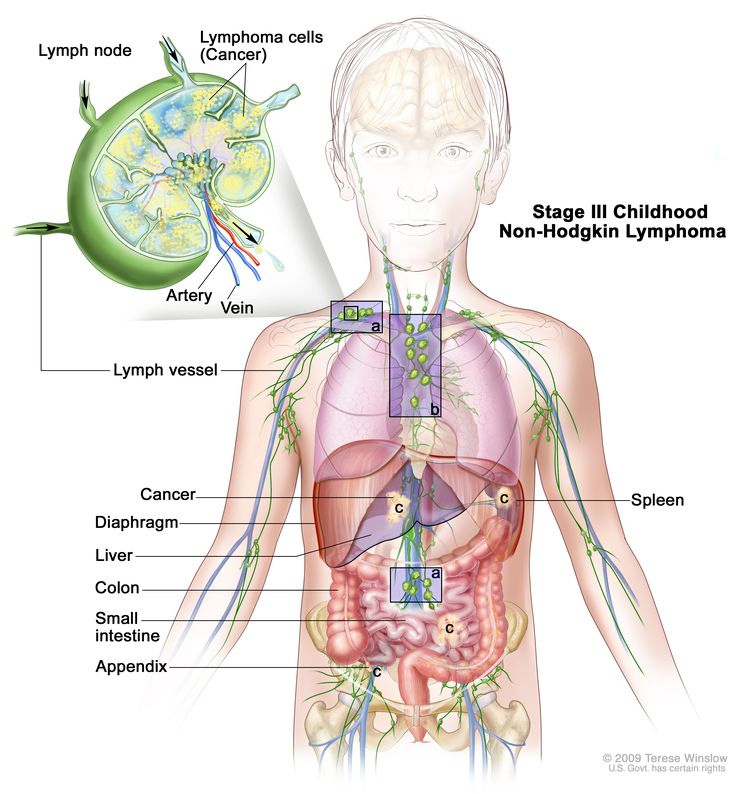
Linfoma no Hodgkin infantil en estadio 3. El cáncer se encuentra en al menos una zona por encima y por debajo del diafragma (a); o el cáncer se ha originado en el tórax (b); o el cáncer se ha originado en el abdomen y se ha extendido por todo el abdomen (c); o en la zona que rodea la columna vertebral (no se muestra).
En el linfoma no Hodgkin infantil en estadio 3, se presenta una de las siguientes situaciones:
- Se encuentra cáncer en al menos un área por encima del diafragma y en al menos un área por debajo del diafragma.
- El cáncer comenzó en el tórax.
- El cáncer comenzó en el abdomen, se diseminó por todo el abdomen y no se puede extirpar por completo mediante cirugía.
- Se encuentra cáncer en el área que rodea la columna vertebral.
Estadio IV
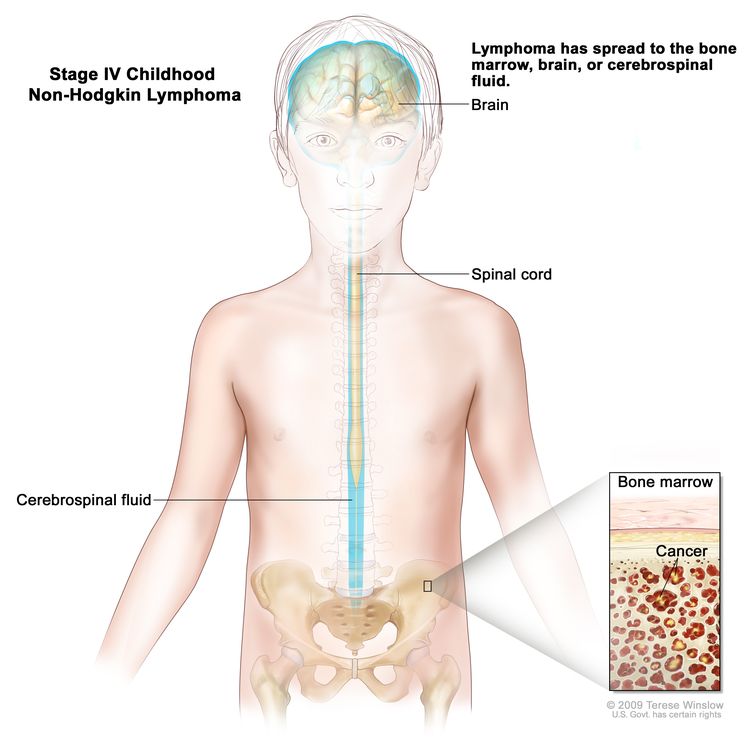
Linfoma no Hodgkin infantil en estadio 4. El cáncer se encuentra en la médula ósea, el cerebro o el líquido cefalorraquídeo (LCR). También es posible que se encuentre cáncer en otras partes del cuerpo.
En el linfoma no Hodgkin infantil en estadio 4, se encuentra cáncer en la médula ósea, el cerebro o el líquido cefalorraquídeo. También es posible que se encuentre cáncer en otras partes del cuerpo.
A veces, el linfoma no Hodgkin infantil no responde al tratamiento o recidiva (vuelve) después del tratamiento.
El linfoma no Hodgkin resistente al tratamiento es un cáncer que no responde al tratamiento inicial.
El linfoma no Hodgkin recidivante es un cáncer que ha reaparecido después del tratamiento. Puede reaparecer en el sistema linfático o en otras partes del cuerpo.
Descripción general de las opciones de tratamiento
Puntos clave
- Hay diferentes tipos de tratamiento para los niños con linfoma no Hodgkin.
- El tratamiento para los niños con linfoma no Hodgkin lo debe planificar un equipo de médicos experto en el tratamiento del cáncer infantil.
- Pueden emplearse los siguientes tipos de tratamiento:
- Cirugía
- Quimioterapia
- Radioterapia
- Trasplante de células madre
- Terapia dirigida
- Otras terapias farmacológicas
- Fototerapia
- Observación cuidadosa
- Inmunoterapia
- El tratamiento del linfoma no Hodgkin infantil puede provocar efectos secundarios.
- Los pacientes pueden evaluar la posibilidad de participar en un ensayo clínico.
- Es posible que se necesiten cuidados de seguimiento.
Hay diferentes tipos de tratamiento para los niños con linfoma no Hodgkin.
Usted y el equipo médico de su hijo o hija colaborarán para decidir el tratamiento. Se tendrán en cuenta muchos factores, como la ubicación del cáncer, el tipo de linfoma no Hodgkin, si el cáncer es reciente o ha recidivado, y la edad y el estado de salud general del niño.
En el plan de tratamiento de su hijo o hija se incluirá la información del tumor, los objetivos y opciones del tratamiento, y los posibles efectos secundarios. Será útil que hable con el equipo de atención de su hijo o hija antes de que comience el tratamiento sobre qué esperar. Para obtener ayuda en cada etapa del proceso, consulte nuestro folleto Niños con cáncer: una guía para padres.
El tratamiento para los niños con linfoma no Hodgkin lo debe planificar un equipo de médicos experto en el tratamiento del cáncer infantil.
El tratamiento lo supervisará un oncólogo pediatra, un médico que se especializa en el tratamiento de niños con cáncer. El oncólogo pediatra trabaja con otros proveedores de atención de la salud expertos en el tratamiento de niños con cánder y que se especializan en ciertas áreas de la medicina. Entre estos especialistas se encuentran los siguientes:
Pueden emplearse los siguientes tipos de tratamiento:
Cirugía
En algunos tipos de linfoma no Hodgkin infantil se hace una cirugía para extirpar tanto tumor como sea posible. Después de que el médico extirpa todo el cáncer que puede ver durante la cirugía, algunos pacientes reciben quimioterapia para destruir cualquier célula cancerosa que haya quedado. El tratamiento que se administra después de la cirugía para disminuir el riesgo de que el cáncer vuelva se llama terapia adyuvante.
Quimioterapia
La quimioterapia (también llamada quimio) utiliza medicamentos para detener el crecimiento de las células cancerosas, ya sea destruyéndolas o impidiendo que se dividan. La quimioterapia puede administrarse sola o con otros tipos de tratamiento.
La quimioterapia para el linfoma no Hodgkin infantil se administra por vía oral o se inyecta en una vena. Al administrarse de esta manera, los medicamentos ingresan al torrente sanguíneo y pueden llegar a las células cancerosas de todo el cuerpo. La quimioterapia para el linfoma no Hodgkin infantil también se administra directamente en el líquido cefalorraquídeo (quimioterapia intratecal), un órgano o una cavidad corporal como el abdomen. Al administrarse de esta manera, los medicamentos afectan sobre todo las células cancerosas de esas áreas.
La quimioterapia intratecal puede utilizarse para tratar el linfoma no Hodgkin infantil que se ha propagado o podría propagarse al cerebro. Cuando se utiliza para reducir la probabilidad de propagación del cáncer al cerebro, se denomina profilaxis del SNC. La quimioterapia intratecal se administra además de la quimioterapia oral o intravenosa. También se pueden utilizar dosis de quimioterapia más altas de lo habitual como profilaxis del SNC.
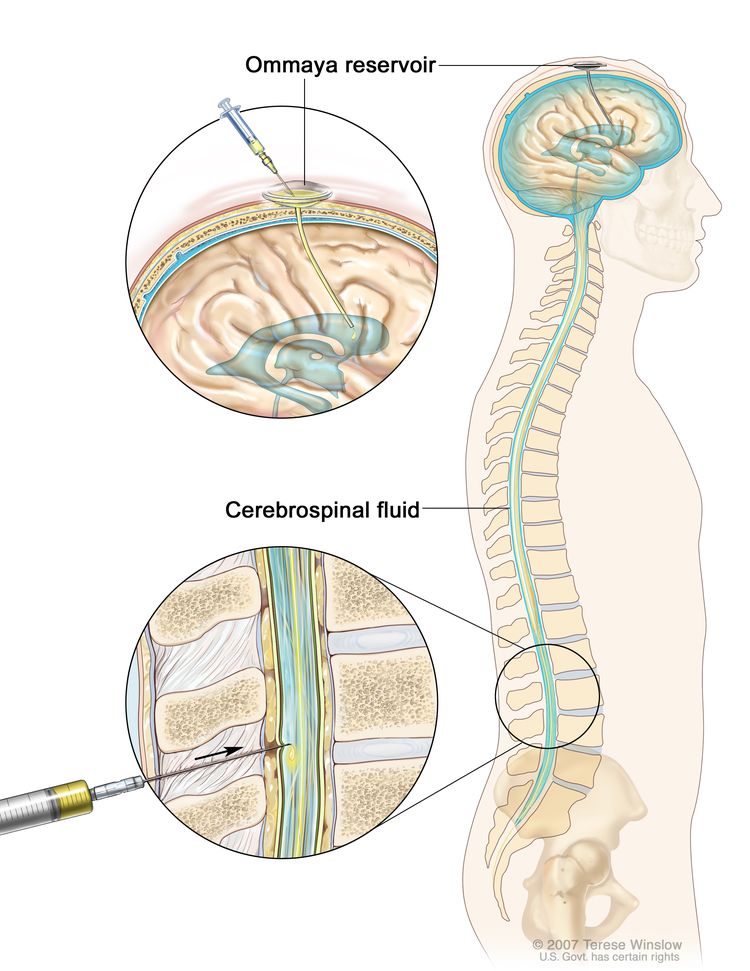
Quimioterapia intratecal. Los medicamentos contra el cáncer se inyectan en el espacio intratecal, que es el espacio que contiene el líquido cefalorraquídeo (LCR, que se muestra en azul). Hay dos formas diferentes de hacerlo. Una forma, que se muestra en la parte superior de la figura, consiste en inyectar los medicamentos en un reservorio de Ommaya (un recipiente con forma de cúpula que se coloca debajo del cuero cabelludo durante la cirugía y que contiene los medicamentos a medida que fluyen a través de un pequeño tubo hacia el cerebro). La otra forma, que se muestra en la parte inferior de la figura, consiste en inyectar los medicamentos directamente en el LCR en la parte inferior de la columna vertebral, después de adormecer una pequeña zona de la parte baja de la espalda.
Los medicamentos de quimioterapia usados solos o en combinación para tratar el linfoma no Hodgkin en niños incluyen:
- Asparaginasa
- Carboplatino
- Ciclofosfamida
- Citarabina
- dexametasona (esteroide)
- doxorrubicina
- Etopósido
- idarubicina
- Ifosfamida
- Metotrexato
- prednisona (esteroide)
- Vinblastina
- Vincristina
También pueden utilizarse otros medicamentos quimioterápicos no incluidos en esta lista.
La forma en que se administra la quimioterapia depende del tipo y estadio del cáncer que se esté tratando.
Más información sobre la quimioterapia para tratar el cáncer.
Radioterapia
La radioterapia es un tratamiento contra el cáncer para el que se usan rayos X de alta energía u otros tipos de radiación para destruir las células cancerosas o impedir que se multipliquen. En la radioterapia externa se usa una máquina que envía la radiación desde el exterior del cuerpo hacia el área en la que se encuentra el cáncer. Se puede usar la radioterapia externa en el tratamiento del linfoma no Hodgkin infantil que se diseminó o se podría diseminar al encéfalo y la la médula espinal. A veces también se usa para el tratamiento del linfoma cutáneo de células T (micosis fungoide).
Para obtener más información, consulte Radioterapia de haz externo para el cáncer y Efectos secundarios de la radioterapia.
Trasplante de células madre
Se administran dosis altas de quimioterapia para destruir las células cancerosas. Este tratamiento destruye también células sanas, incluidas las células hematopoyéticas. El trasplante de células madre es un tratamiento para reemplazar las células hematopoyéticas. Las células madre (células sanguíneas inmaduras) se extraen de la sangre o la médula ósea del paciente o de un donante, se congelan y se almacenan. Después de que el paciente termina la quimioterapia, las células madre almacenadas se descongelan y se devuelven al paciente mediante una infusión. Estas células madre reinfundidas se convierten en células sanguíneas del cuerpo y restauran las células destruidas. Las células madre del donante también pueden detectar y destruir cualquier célula cancerosa que quede en el cuerpo.
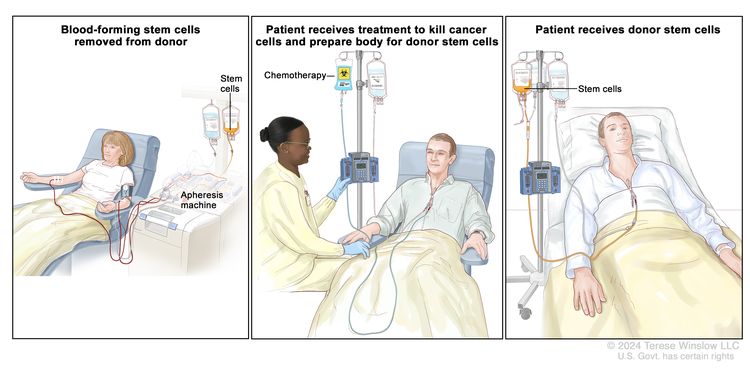
Trasplante de células madre de un donante. (Paso 1): Cuatro o cinco días antes de la recolección de células madre del donante, este recibe un medicamento para aumentar la cantidad de células madre que circulan por su torrente sanguíneo (no se muestra en la imagen). Las células madre hematopoyéticas se extraen del donante a través de una vena grande del brazo. La sangre fluye a través de una máquina de aféresis que extrae las células madre. El resto de la sangre se devuelve al donante a través de una vena del otro brazo. (Paso 2): El paciente recibe quimioterapia para destruir las células cancerosas y preparar su cuerpo para las células madre del donante. El paciente también puede recibir radioterapia (no se muestra en la imagen). (Paso 3): El paciente recibe una infusión de las células madre del donante.
Terapia dirigida
En la terapia dirigida, se usan medicamentos u otras sustancias que bloquean la acción de enzimas, proteínas y otras moléculas específicas que participan en la multiplicación y diseminación de células cancerosas. En el tratamiento del linfoma no Hodgkin infantil, se usan diferentes tipos de terapia dirigida, como los siguientes:
Obtenga más información en Terapia dirigida para tratar el cáncer.
Otras terapias farmacológicas
Los retinoides son medicamentos relacionados con la vitamina A. La terapia con retinoides con bexaroteno se utiliza para tratar varios tipos de linfoma cutáneo de células T.
Los esteroides son hormonas que el cuerpo produce de forma natural. También pueden fabricarse en un laboratorio y utilizarse como medicamentos. La terapia con esteroides de aplicación tópica se utiliza para tratar el linfoma cutáneo de células T. La dexametasona y la prednisona son esteroides que se utilizan junto con otros fármacos para tratar ciertos tipos de linfoma.
Los antibióticos son medicamentos que se utilizan para tratar infecciones y cánceres causados por bacterias u otros microorganismos. Se han utilizado para tratar el linfoma de tejido linfoide asociado a mucosas (MALT). El tratamiento con antibióticos se ha estudiado principalmente en adultos.
Fototerapia
La fototerapia es un tratamiento contra el cáncer que usa un medicamento y un tipo de luz láser para eliminar células cancerosas. Se inyecta en la vena un medicamento que se activa al exponerse a la luz. El medicamento se acumula más en las células cancerosas que en las normales. Para el cáncer de piel, se aplica luz láser sobre la piel y el fármaco se activa y destruye las células cancerosas. La fototerapia se utiliza en el tratamiento del linfoma cutáneo de células T.
Observación cuidadosa
La observación cautelosa consiste en vigilar de cerca el estado del paciente sin administrar ningún tratamiento hasta que aparezcan o cambien los signos o síntomas.
Inmunoterapia
La inmunoterapia ayuda al sistema inmunitario a combatir el cáncer. Los siguientes son tipos de inmunoterapia:
- Terapia con células CAR-T cambia el paciente células T (un tipo de célula del sistema inmunológico) del paciente para que ataquen ciertas proteínas en la superficie de las células cancerosas. Estas células se obtienen del paciente y se les añaden receptores especiales a su superficie en el laboratorio. Las células cambiadas se llaman (receptor de antígeno quimérico) Células T CAR. Estas células se cultivan en el laboratorio y se administran al paciente mediante infusión. Se multiplican en la sangre del paciente y atacan las células cancerosas. La terapia con células T CAR se está estudiando para el tratamiento del linfoma de Burkitt y del linfoma difuso de células B grandes que no ha respondido al tratamiento o ha reaparecido (recurrido).
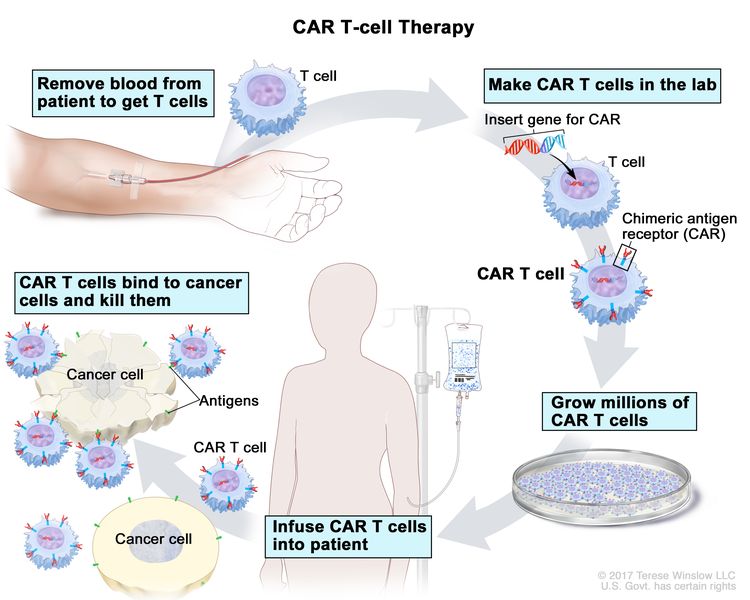
Terapia con células CAR-T: es un tratamiento en el que las células T del paciente (un tipo de célula inmunitaria) se modifican en el laboratorio para que se unan a las células cancerosas y las destruyan. La sangre del paciente fluye desde una vena del brazo a través de un tubo hacia una máquina de aféresis (no mostrada en el dibujo), que extrae los glóbulos blancos, incluidas las células T, y devuelve el resto de la sangre al paciente. En el laboratorio, se inserta un gen especial llamado receptor de antígeno quimérico (CAR) en las células T. Millones de estas células CAR-T se cultivan y se administran al paciente mediante una infusión. Una vez en el cuerpo, las células CAR-T se unen a un antígeno en las células cancerosas y las destruyen.
- La ciclosporina A se utiliza en combinación con esteroides para el tratamiento del linfoma subcutáneo de células T paniculítico.
Obtenga más información sobre la inmunoterapia para el tratamiento del cáncer .
El tratamiento del linfoma no Hodgkin infantil puede provocar efectos secundarios.
Los tratamientos contra el cáncer pueden causar efectos secundarios. La naturaleza de estos efectos dependerá del tipo de tratamiento, la dosis administrada y de cómo reaccione el cuerpo de su hijo o hija. Hable con el equipo de tratamiento del niño sobre los efectos secundarios a los que debe prestar atención y las formas de controlarlos.
Para obtener más información sobre los efectos secundarios que aparecen durante el tratamiento del cáncer, consulte la sección Efectos secundarios.
Los problemas derivados del tratamiento del cáncer que comienzan seis o más meses después del tratamiento y continúan durante meses o años se denominan efectos tardíos. A continuación se enumeran algunos efectos tardíos del tratamiento del cáncer:
- Problemas físicos, incluidos problemas en el corazón, en los huesos y de fertilidad
- Cambios en el estado de ánimo, los sentimientos, los pensamientos, el aprendizaje o la memoria
- Segundos cánceres (nuevos tipos de cáncer), como tumores cerebrales, leucemia mieloide aguda y síndrome mielodisplásico
Algunos efectos tardíos pueden tratarse o controlarse. Es importante hablar con los pediatras sobre los efectos que el tratamiento del cáncer puede tener en su hijo o hija. Para obtener más información, consulte Efectos tardíos del tratamiento anticanceroso en la niñez.
Los pacientes pueden evaluar la posibilidad de participar en un ensayo clínico.
Para algunos niños, participar en un ensayo clínico puede ser una opción. Hay distintos tipos de ensayos clínicos para el cáncer infantil. Por ejemplo, un ensayo de tratamiento prueba nuevos tratamientos o nuevas formas de utilizar los tratamientos actuales. Los ensayos de atención de apoyo y cuidados paliativos buscan formas de mejorar la calidad de vida, especialmente para quienes presentan efectos secundarios del cáncer y su tratamiento.
Puede usar la búsqueda de ensayos clínicos para encontrar ensayos clínicos sobre cáncer financiados por el NCI que aceptan participantes. Esta búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad de su hijo o hija y el lugar donde se realizan. Puede encontrar ensayos clínicos financiados por otras organizaciones en el sitio web ClinicalTrials.gov.
Para más información sobre ensayos clínicos, cómo encontrarlos y participar en uno de ellos, visite la web Información sobre estudios clínicos para pacientes y cuidadores.
Es posible que se necesiten cuidados de seguimiento.
Durante el tratamiento, su hijo/a se someterá a pruebas o revisiones de seguimiento. Algunas pruebas realizadas para diagnosticar o estadificar el cáncer podrían repetirse para evaluar la eficacia del tratamiento. Las decisiones sobre si continuar, modificar o suspender el tratamiento podrían basarse en los resultados de estas pruebas.
Algunas de las pruebas se seguirán realizando periódicamente después de que finalice el tratamiento. Los resultados de estas pruebas pueden mostrar si la afección de su hijo o hija ha cambiado o si el cáncer ha recidivado (regresado).
Opciones de tratamiento para el linfoma no Hodgkin infantil
Linfoma de Burkitt
Tratamiento del linfoma de Burkitt
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma de Burkitt recién diagnosticado incluye las siguientes opciones:
- Cirugía para extirpar la mayor cantidad posible de tumor, seguida de quimioterapia combinada
- Quimioterapia combinada con o sin terapia dirigida (rituximab)
Tratamiento del linfoma de Burkitt recidivante o resistente al tratamiento
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma de Burkitt recidivante o resistente al tratamiento incluye las siguientes opciones:
- Quimioterapia combinada con o sin terapia dirigida (rituximab)
- Terapia dirigida (rituximab), quimioterapia combinada y dexametasona
- Quimioterapia de dosis alta con trasplante de células madre con células del propio paciente o células de un donante
- Terapia con células CAR-T
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Linfoma difuso de células B grandes
Tratamiento del linfoma difuso de células B grandes
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma difuso de células B grandes recién diagnosticado incluye las siguientes opciones:
- Cirugía para extirpar la mayor cantidad posible de tumor, seguida de quimioterapia combinada
- Quimioterapia combinada con o sin terapia dirigida (rituximab)
Tratamiento del linfoma difuso de células B grandes recidivante o resistente al tratamiento
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma difuso de células B grandes recidivante o resistente al tratamiento incluye las siguientes opciones:
- Quimioterapia combinada con o sin terapia dirigida (rituximab)
- Terapia dirigida (rituximab), quimioterapia combinada y dexametasona
- Trasplante de células madre con células del propio paciente o de un donante
- Terapia con células CAR-T
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Linfoma mediastínico primario de células B
Tratamiento del linfoma mediastínico primario de células B
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma mediastínico primario de células B recién diagnosticado puede incluir quimioterapia combinada, prednisona, terapia dirigida (rituximab) y, a veces, radioterapia.
Tratamiento del linfoma mediastínico primario de células B recidivante o resistente al tratamiento
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma mediastínico primario de células B recidivante o resistente al tratamiento puede incluir terapia dirigida (pembrolizumab).
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Linfoma linfoblástico
Tratamiento del linfoma linfoblástico
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El linfoma linfoblástico y la leucemia linfoblástica aguda (LLA) a veces se clasifican como la misma enfermedad. El tratamiento del linfoma linfoblástico incluye las siguientes opciones:
- Quimioterapia combinada
- También se puede hacer profilaxis del SNC con radioterapia o quimioterapia intratecal para evitar que el cáncer se propague al encéfalo o a la médula espinal.
Tratamiento del linfoma linfoblástico recidivante o resistente al tratamiento al tratamiento
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma linfoblástico recidivante o resistente al tratamiento incluye las siguientes opciones:
- Quimioterapia
- Trasplante de células madre con células de un donante
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Linfoma anaplásico de células grandes
Tratamiento del linfoma anaplásico de células grandes
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma anaplásico de células grandes incluye las siguientes opciones:
- Cirugía seguida de quimioterapia combinada
- Quimioterapia combinada con o sin prednisona
- Quimioterapia intratecal y combinada para pacientes con cáncer en el encéfalo o en la médula espinal
Tratamiento del linfoma anaplásico de células grandes recidivante o resistente al tratamiento al tratamiento
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma anaplásico de células grandes recidivante o resistente al tratamiento incluye las siguientes opciones:
- Quimioterapia
- Terapia dirigida (brentuximab vedotin o crizotinib)
- Quimioterapia seguida de un trasplante de células madre con células del propio paciente o células de un donante
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Enfermedad linfoproliferativa asociada a inmunodeficiencia en niños
Tratamiento de la enfermedad linfoproliferativa asociada a inmunodeficiencia primaria
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento de la enfermedad linfoproliferativa en niños y adolescentes con sistemas inmunitarios debilitados incluye las siguientes opciones:
- Quimioterapia con o sin terapia dirigida (rituximab)
- Se puede usar el trasplante de células madre con células de un donante para tratar la inmunodeficiencia primaria y disminuir el riesgo de que el cáncer regrese.
Tratamiento del linfoma no Hodgkin asociado a síndromes de defectos de reparación del ADN
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma no Hodgkin asociado con síndromes de defectos de reparación del ADN en niños puede incluir quimioterapia.
Tratamiento del linfoma no Hodgkin asociado al VIH
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento con terapia antirretroviral de gran actividad o TARGA (una combinación de medicamentos antirretrovirales) reduce el riesgo de linfoma no Hodgkin en pacientes infectados con el VIH.
El tratamiento del linfoma no Hodgkin (LNH) asociado al VIH en niños puede incluir quimioterapia con o sin terapia dirigida (rituximab).
Tratamiento de la enfermedad linfoproliferativa postrasplante
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento de la enfermedad linfoproliferativa postrasplante incluye las siguientes opciones:
- Cirugía para extirpar el tumor. Si es posible, se pueden administrar dosis bajas de inmunosupresores después de un trasplante de células madre o de un órgano.
- Terapia dirigida (rituximab)
- Quimioterapia con o sin terapia dirigida (rituximab)
Linfomas no Hodgkin raros que se presentan en niños
Tratamiento del linfoma folicular de tipo pediátrico
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma folicular en niños puede incluir:
- Cirugía
- Quimioterapia combinada con o sin terapia dirigida (rituximab)
Para los niños cuyo cáncer presenta ciertas alteraciones genéticas, el tratamiento es similar al que se administra a los adultos con linfoma folicular. Para obtener información sobre el tratamiento del linfoma folicular en adultos, consulte Tratamiento del linfoma no Hodgkin.
Tratamiento del linfoma de zona marginal
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma de zona marginal (incluido el linfoma de tejido linfoide asociado a mucosas [MALT]) en niños incluye las siguientes opciones:
- Cirugía
- Radioterapia
- Terapia dirigida (rituximab) con o sin quimioterapia
- Tratamiento con antibióticos para el linfoma MALT
Tratamiento del linfoma primario del sistema nervioso central
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma primario del SNC en niños puede incluir quimioterapia y terapia dirigida (rituximab).
Tratamiento del linfoma periférico de células T
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma periférico de células T en niños incluye las siguientes opciones:
- Quimioterapia
- Radioterapia
- Trasplante de células madre con células del propio paciente o de un donante
Tratamiento del linfoma cutáneo de células T
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento del linfoma subcutáneo de células T similar a la paniculitis en niños incluye las siguientes opciones:
- Observación cautelosa
- Inmunoterapia con esteroides con o sin ciclosporina A o ruxolitinib
- Terapia dirigida (denileucina diftitox)
- Quimioterapia combinada
- Terapia con retinoides
- Trasplante de células madre
El tratamiento del linfoma anaplásico de células grandes cutáneo puede incluir cirugía, radioterapia o ambas.
Tratamiento de la micosis fungoide
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
En niños, el tratamiento de la micosis fungoide puede incluir:
- Esteroides aplicados a la piel
- Terapia con retinoides
- Radioterapia
- Fototerapia (terapia de luz con radiación ultravioleta B)
Tratamiento de la papulosis linfomatoide
Para obtener información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
En los niños, el tratamiento de la papulosis linfomatoide puede consistir en:
- Observación cautelosa
- Esteroides aplicados a la piel
- Fototerapia (terapia de luz con radiación ultravioleta B)
- Dosis bajas de quimioterapia (metotrexato)
Más información sobre el linfoma no Hodgkin infantil
Para obtener más información del National Cancer Institute sobre el linfoma no Hodgkin infantil, consulte los siguientes sitios web:
- Medicamentos aprobados para el linfoma no Hodgkin
- Trasplantes de células madre en el tratamiento del cáncer
Para obtener más información sobre el cáncer infantil y otros recursos generales sobre el cáncer, consulte los siguientes sitios web:
- El cáncer
- Cánceres infantiles
- CureSearch para el cáncer infantil
- Efectos tardíos del tratamiento del cáncer infantil
- Adolescentes y adultos jóvenes con cáncer
- Niños con cáncer: una guía para padres
- El cáncer en los niños y los adolescentes
- Estadificación del cáncer
- Cómo hacer frente al cáncer
- Preguntas para el médico sobre el cáncer
- Para supervivientes, cuidadores e intercesores
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen del PDQ sobre el cáncer contiene información actualizada sobre el tratamiento del linfoma no Hodgkin infantil. Su objetivo es informar y ayudar a los pacientes, las familias y los cuidadores. No proporciona directrices ni recomendaciones formales para tomar decisiones sobre la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
La información de este resumen para pacientes procede de la versión para profesionales de la salud, la cual es revisada y actualizada periódicamente por el comité editorial del PDQ sobre el tratamiento pediátrico según sea necesario.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre el tratamiento pediátrico. Tratamiento del linfoma no Hodgkin infantil (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Actualizado:
URL de origen: https://www.cancer.gov/node/4799/syndication
Agencia de origen: National Cancer Institute (NCI)
Fecha de captura: 2013-09-14 09:02:27.0