








Tratamiento del glioma de tronco encefálico
El Centro Oncológico Integral Montefiore Einstein del Hospital Infantil Montefiore Einstein (CHAM) ofrece un tratamiento y atención excepcionales para el glioma del tronco encefálico de su hijo. Especialistas en hematología, oncología y terapia celular brindan la mejor atención disponible y terapias de vanguardia, incluyendo ensayos clínicos, en un entorno de apoyo y cuidado.
Nuestro modelo de investigación interdisciplinaria reúne a médicos destacados con científicos reconocidos internacionalmente para desarrollar nuestras propias terapias y estrategias de tratamiento innovadoras. Contamos con un equipo de especialistas dedicado a cada paciente con el que trabajamos. Este equipo incluye oncólogos pediátricos, cirujanos oncólogos, enfermeros especializadas en oncología, oncólogos radiólogos, radiólogos de diagnóstico, patólogos, psiquiatras, psicólogos, fisioterapeutas y terapeutas ocupacionales, además de trabajadores sociales y especialistas en desarrollo infantil, entre otros. Juntos, crean un entorno afectuoso y enriquecedor para que usted y su hijo o hija se sientan lo más cómodos posible durante el proceso de atención.
Si lo que usted desea es lo mejor para su hijo, acuda a los especialistas del Centro Oncológico Integral Montefiore Einstein en CHAM, quienes se dedican con pasión a erradicar el cáncer y a atender todas las necesidades de salud de su hijo.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Tratamiento del glioma de tronco encefálico infantil (PDQ®): versión para pacientes
Información general sobre el glioma de tronco encefálico infantil
Puntos clave
- El glioma de tronco encefálico infantil es una enfermedad en la que se forman células benignas (no cancerosas) o malignas (cancerosas) en los tejidos del tronco encefálico.
- Hay dos tipos de gliomas de tronco encefálico en niños.
- Se desconoce la causa de la mayoría de los tumores cerebrales infantiles.
- Los signos y síntomas del glioma de tronco encefálico no son los mismos en todos los niños.
- Las pruebas que examinan el cerebro se utilizan para detectar (encontrar) el glioma de tronco encefálico infantil.
- Se puede realizar una biopsia para diagnosticar ciertos tipos de glioma de tronco encefálico.
- Hay ciertos factores que afectan al pronóstico (la probabilidad de recuperación).
El glioma de tronco encefálico infantil es una enfermedad en la que se forman células benignas (no cancerosas) o malignas (cancerosas) en los tejidos del tronco encefálico.
Los gliomas son tumores formados a partir de células gliales. Las células gliales del cerebro mantienen las células nerviosas en su lugar, llevan alimento y oxígeno a las células nerviosas y ayudan a protegerlas de enfermedades, como las infecciones. En el glioma de tronco encefálico, las células gliales del tronco encefálico se ven afectadas.
El tronco encefálico está formado por el mesencéfalo, la protuberancia y la médula. Es la parte más baja del cerebro y se conecta con la médula espinal, justo encima de la parte posterior del cuello. El tronco encefálico controla funciones vitales como la respiración, la frecuencia cardiaca y la presión arterial, así como los nervios y músculos utilizados para ver, oír, caminar, hablar y comer.
La mayoría de los gliomas de tronco encefálico infantiles son gliomas pontinos intrínsecos difusos (GPID), que se forman en la protuberancia. Los gliomas focales se forman en otras partes del tronco encefálico.
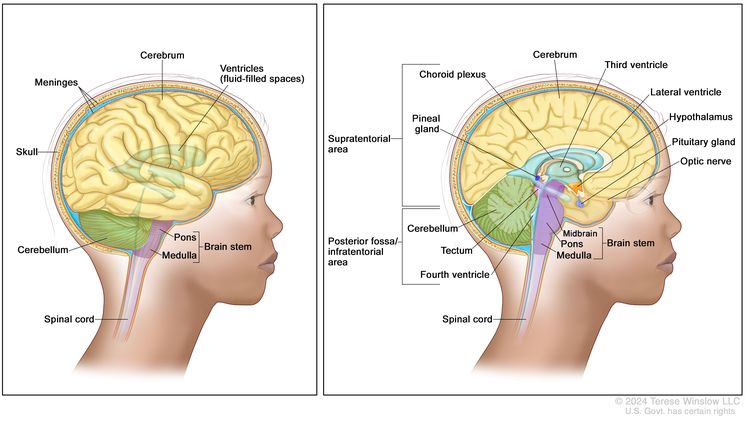
Anatomía del encéfalo. El área supratentorial (la parte superior del cerebro) contiene el cerebro, el ventrículo lateral y el tercer ventrículo (el líquido cefalorraquídeo se muestra en azul), el plexo coroideo, la glándula pineal, el hipotálamo, la glándula pituitaria y el nervio óptico. La fosa posterior/área infratentorial (la parte posterior inferior del encéfalo) contiene el cerebelo, el techo, el cuarto ventrículo y el tronco encefálico (mesencéfalo, protuberancia y bulbo raquídeo). El tentorio separa el área supratentorial del área infratentorial (panel derecho). El cráneo y las meninges protegen el cerebro y la médula espinal (panel izquierdo).
Los tumores cerebrales son el segundo tipo de cáncer más común en los niños.
Este resumen aborda el tratamiento de los tumores cerebrales primarios, es decir, tumores que se originan en el cerebro. En contraste, el tratamiento de los tumores cerebrales metastásicos, que son aquellos formados por células cancerosas que surgen en otras partes del cuerpo y se propagan al cerebro, no se trata en este documento.
Los tumores cerebrales pueden presentarse tanto en niños como en adultos; sin embargo, el tratamiento en niños puede diferir del aplicado en adultos. Para obtener información sobre el tratamiento de los tumores cerebrales en adultos, consulte el resumen del PDQ Tratamiento de los tumores del sistema nervioso central en adultos.
Hay dos tipos de gliomas de tronco encefálico en niños.
Aunque el glioma pontino intrínseco difuso (GPID) y el glioma de tronco encefálico focal se forman en el mismo tipo de célula, actúan de manera diferente:
- GPID: el GPID es un tumor de rápido crecimiento que se desarrolla en la protuberancia. Es difícil de tratar y tiene un pronóstico desfavorable (posibilidad de recuperación) debido a lo siguiente:
- No es un tumor bien definido y se disemina entre las células sanas del tronco encefálico.
- Las funciones vitales, como la respiración y el ritmo cardiaco, pueden verse afectadas.
- Glioma focal de tronco encefálico: un glioma focal es un tumor de crecimiento lento que se forma fuera de la protuberancia, afectando solo una zona del tronco encefálico. Es más fácil de tratar y tiene un mejor pronóstico que el GPID.
Se desconoce la causa de la mayoría de los tumores cerebrales infantiles.
Cualquier elemento que aumente el riesgo de desarrollar una enfermedad se denomina factor de riesgo. Tener un factor de riesgo no implica necesariamente que se vaya a desarrollar cáncer; de igual forma, no tener factores de riesgo tampoco garantiza que no se desarrollará la enfermedad. Consulte con el médico de su hijo o hija si cree que podría estar en riesgo. Los posibles factores de riesgo del glioma de tronco encefálico son:
- Tener ciertos trastornos genéticos, como neurofibromatosis tipo 1 (NF1)
Los signos y síntomas del glioma de tronco encefálico no son los mismos en todos los niños.
Los signos y síntomas dependen de los siguiente facores:
- Dónde se forma el tumor en el cerebro
- El tamaño del tumor y si se ha diseminado por todo el tronco encefálico
- La rapidez con la que crece el tumor
- La edad del niño y su etapa de desarrollo
Los signos y síntomas pueden deberse a gliomas del tronco encefálico infantiles u otras afecciones. Consulte con el médico de su hijo o hija si presenta alguno de los siguientes síntomas:
- Problemas con el movimiento de los ojos (el ojo permanece vuelto hacia adentro)
- Problemas de la vista
- Dolor de cabeza matinal o dolor de cabeza que desaparece después de vomitar
- Náuseas y vómitos
- Somnolencia inusual
- Pérdida de la capacidad de mover un lado de la cara o del cuerpo
- Pérdida del equilibrio y dificultad para caminar
- Menor o mayor energía de lo habitual
- Cambios en el comportamiento
- Problemas de aprendizaje en la escuela
Las pruebas que examinan el cerebro se utilizan para detectar (encontrar) el glioma de tronco encefálico infantil.
Se pueden utilizar las siguientes pruebas y procedimientos:
- Reconocimiento físico e historial de salud: un examen del cuerpo para evaluar el estado general de salud, incluida la detección de signos de enfermedad, como bultos o cualquier otra anomalía. También se toma nota de los hábitos de salud del paciente y de sus enfermedades y tratamientos previos.
- Examen neurológico: una serie de preguntas y pruebas para evaluar el cerebro, la médula espinal y la función nerviosa. El examen verifica el estado mental, la coordinación, la capacidad de una persona para caminar con normalidad y lo bien que funcionan los músculos, los sentidos y los reflejos. También se conoce como evaluación neurológica.
- Resonancia magnética (RM) con gadolinio: un procedimiento que utiliza un imán, ondas de radio y una computadora para generar una serie de imágenes detalladas de las áreas internas del cerebro. Se inyecta una sustancia llamada gadolinio en una vena. El gadolinio se acumula alrededor de las células cancerosas, haciéndolas más brillantes en la imagen. Este procedimiento también se denomina resonancia magnética nuclear (RMN).
Se puede realizar una biopsia para diagnosticar ciertos tipos de glioma de tronco encefálico.
Si en la resonancia magnética se observa que el tumor es un GPID, generalmente no se realiza una biopsia ni se extirpa el tumor. Cuando los resultados de la resonancia magnética son inciertos, se puede optar por realizar una biopsia.
Si la resonancia magnética sugiere la presencia de un glioma focal de tronco encefálico, se puede realizar una biopsia. Se extrae una parte del cráneo y se utiliza una aguja para extraer una muestra del tejido cerebral. A veces, la aguja se guía por una computadora. Un patólogo observa el tejido bajo un microscopio para buscar células cancerosas. Si se encuentran células cancerosas, el médico puede extirpar la mayor cantidad de tumor posible de forma segura durante la misma cirugía.
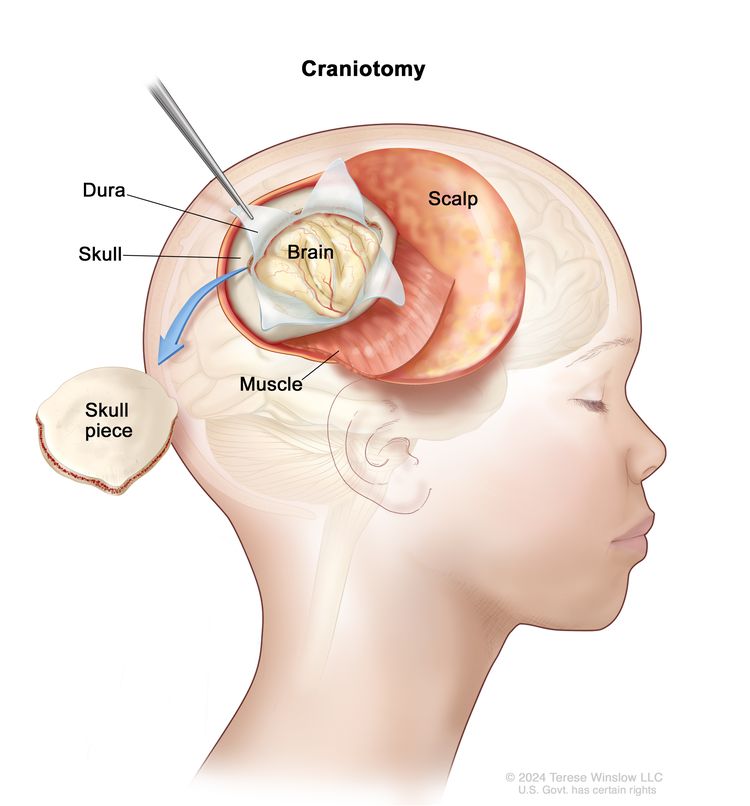
Craneotomía. Se realiza una abertura y se extrae una pieza del cráneo para exponer una parte del cerebro.
La siguiente prueba se puede realizar en la muestra de tejido extraída durante la biopsia o la cirugía:
- La inmunohistoquímica es una prueba de laboratorio que emplea anticuerpos para identificar determinados antígenos (marcadores) en una muestra de tejido de un paciente. Los anticuerpos suelen estar ligados a una enzima o tinte fluorescente. Una vez que los anticuerpos se unen a un antígeno específico en la muestra de tejido, la enzima o el colorante se activan, lo que permite visualizar el antígeno con un microscopio. Este tipo de prueba se utiliza para diagnosticar el cáncer y diferenciar distintos tipos de cáncer.
Hay ciertos factores que afectan al pronóstico (la probabilidad de recuperación).
El pronóstico del niño depende de los siguientes factores:
- El tipo de glioma de tronco encefálico (GPID o glioma focal)
- La ubicación del tumor en el cerebro y si se ha propagado dentro del tronco encefálico
- La edad del niño en el momento del diagnóstico
- El tiempo que el niño ha presentado síntomas antes del diagnóstico
- La presencia o ausencia de una enfermedad llamada neurofibromatosis tipo 1
- La existencia de cambios específicos en el gen H3 K27m
- Si el tumor acaba de ser diagnosticado o ha recidivado (regresado)
La mayoría de los niños con GPID viven menos de 18 meses después del diagnóstico. Los niños con un glioma focal suelen vivir más de 5 años.
Estadios del glioma de tronco encefálico infantil
Puntos clave
- El plan de tratamiento del cáncer depende de si el tumor se encuentra en una área específica del cerebro o si se ha diseminado por todo el órgano.
El plan de tratamiento del cáncer depende de si el tumor se encuentra en una área específica del cerebro o si se ha diseminado por todo el órgano.
La estadificación es el proceso que se utiliza para determinar la extensión del cáncer y si se ha propagado. Es importante conocer el estadio para planificar el tratamiento.
No existe un sistema de estadificación estándar para el glioma de tronco encefálico infantil. El tratamiento se basa en los siguientes factores:
- Si el tumor es de reciente diagnóstico, progresivo (continúa creciendo) o recurrente (ha regresado después del tratamiento)
- El tipo de tumor (ya sea un glioma pontino intrínseco difuso o un glioma focal)
Un glioma focal de tronco encefálico puede reaparecer muchos años después del primer tratamiento. El tumor puede volver a manifestarse en el cerebro o en otras partes del sistema nervioso central. Antes de administrar el tratamiento contra el cáncer, se pueden realizar pruebas de imágenes, una biopsia o una cirugía para confirmar la presencia de células cancerosas y determinar su extensión.
Treatment Option Overview
Puntos clave
- Existen diferentes tipos de tratamiento para los niños con glioma de tronco encefálico.
- Los niños con glioma del tronco encefálico deben tener su tratamiento planificado por un equipo de profesionales de la salud que sean expertos en el tratamiento de tumores cerebrales infantiles.
- Se utilizan cinco tipos de tratamiento estándar:
- Cirugía
- Radioterapia
- Quimioterapia
- Desviación de líquido cefalorraquídeo
- Observation
- New types of treatment are being tested in clinical trials.
- Terapia dirigida
- El tratamiento para el glioma de tronco encefálico infantil puede causar efectos secundarios.
- Patients may want to think about taking part in a clinical trial.
- Patients can enter clinical trials before, during, or after starting their cancer treatment.
- Pueden ser necesarias pruebas de seguimiento.
Existen diferentes tipos de tratamiento para los niños con glioma de tronco encefálico.
Existen diferentes tipos de tratamientos disponibles para niños con glioma de tronco encefálico. Algunos son estándar (es decir, los tratamientos que se utilizan actualmente) y otros se están evaluando en ensayos clínicos. Un ensayo clínico de tratamiento es un estudio de investigación cuyo objetivo es mejorar los tratamientos existentes y obtener información sobre nuevos tratamientos para pacientes con cáncer. Cuando los ensayos clínicos demuestran que un tratamiento nuevo supera al estándar, este puede adoptarse como el nuevo tratamiento habitual.
Because cancer in children is rare, taking part in a clinical trial should be considered. Some clinical trials are open only to patients who have not started treatment.
Los niños con glioma del tronco encefálico deben tener su tratamiento planificado por un equipo de profesionales de la salud que sean expertos en el tratamiento de tumores cerebrales infantiles.
El oncólogo pediátrico, un médico que se especializa en el tratamiento de niños con cáncer, supervisa el tratamiento. El oncólogo pediátrico trabaja con otros proveedores de atención médica pediátrica que son expertos en el tratamiento de niños con tumores cerebrales, cada uno con conocimientos específicos en diferentes áreas de la medicina. El equipo también puede incluir a otros especialistas, como:
Se utilizan cinco tipos de tratamiento estándar:
Cirugía
Por lo general, no se realiza una biopsia o cirugía para extirpar el GPID debido a lo siguiente:
- El GPID no es una masa única. Se propaga entre las células cerebrales sanas del tronco encefálico.
- Las funciones vitales, como la respiración y el ritmo cardiaco, pueden verse afectadas.
Se puede utilizar una biopsia para diagnosticar o una cirugía para extirpar el tumor en el glioma focal de tronco encefálico infantil.
Radioterapia
La radioterapia es un tratamiento contra el cáncer que utiliza rayos X de alta energía u otros tipos de radiación para matar las células cancerosas o evitar que crezcan. Hay dos tipos de radioterapia:
- La radioterapia externa utiliza una máquina que envía radiación desde el exterior del cuerpo hacia la zona donde se encuentra el cáncer.
- La radioterapia interna utiliza una sustancia radiactiva sellada en agujas, semillas, cables o catéteres que se colocan directamente en el cáncer o cerca de él.
La administración de la radioterapia varía según el tipo de cáncer que se esté tratando. Para el GPID, se emplea radioterapia externa. En el caso de los gliomas focales de tronco encefálico, se puede recurrir tanto a radioterapia externa como interna.
Varios meses después de la radioterapia dirigida al cerebro, los diagnósticos por imágenes pueden revelar cambios en el tejido cerebral. Estos cambios pueden ser consecuencia de la radioterapia o indicar que el tumor está creciendo. Es fundamental confirmar el crecimiento tumoral antes de administrar más tratamiento.
Quimioterapia
La quimioterapia es un tratamiento contra el cáncer que utiliza medicamentos para detener el crecimiento de las células cancerosas, ya sea matándolas o impidiendo que se dividan. Cuando la quimioterapia se toma por vía oral o se inyecta en una vena o músculo, los medicamentos entran en el torrente sanguíneo y pueden llegar a las células cancerosas de todo el cuerpo (quimioterapia sistémica).
Dado que la radioterapia dirigida al cerebro puede afectar el crecimiento y desarrollo cerebral en niños pequeños, se puede administrar quimioterapia para retrasar o reducir la necesidad de radioterapia.
Desviación de líquido cefalorraquídeo
La desviación del líquido cefalorraquídeo es un método que se utiliza para drenar el líquido que se ha acumulado en el cerebro. Se coloca una derivación (tubo largo y delgado) en un ventrículo (espacio lleno de líquido) del cerebro y se pasa debajo de la piel hasta otra parte del cuerpo, generalmente el abdomen. La derivación transporta el exceso de líquido fuera del cerebro para que pueda absorberse en otras partes del cuerpo.
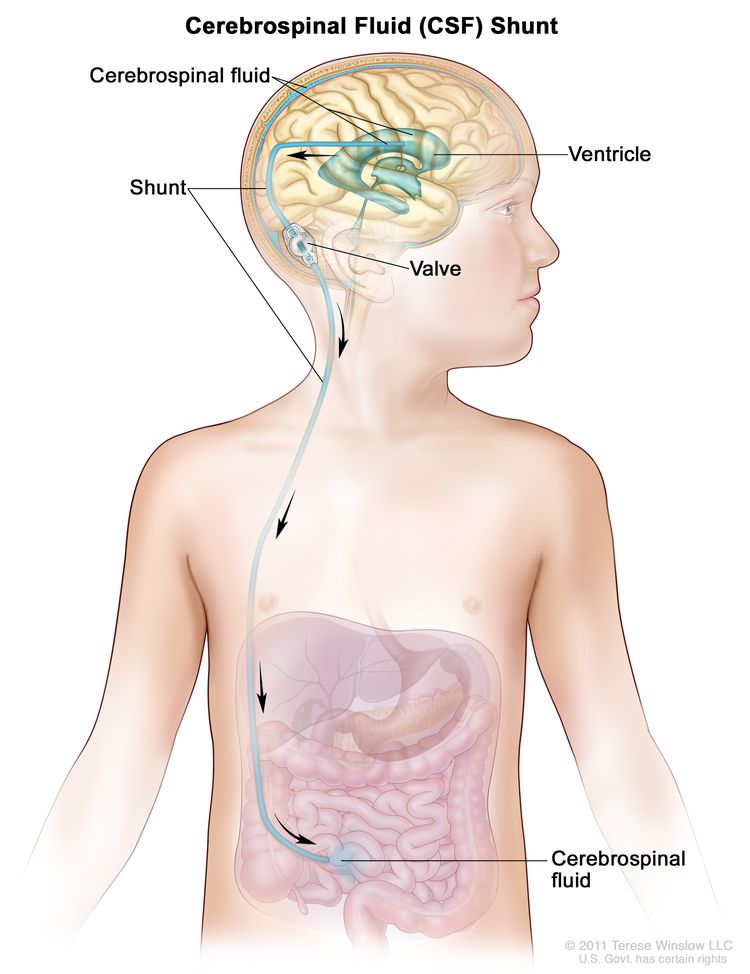
Una desviación o derivación de líquido cefalorraquídeo (LCR) es un tubo largo y delgado que transporta el exceso de LCR fuera del cerebro para que pueda ser absorbido en otras partes del cuerpo. Se coloca en un ventrículo (espacio lleno de líquido) del cerebro y se pasa debajo de la piel hasta otra parte del cuerpo, generalmente el abdomen. La derivación incluye una válvula que controla el flujo del LCR.
Observation
La observación consiste en la supervisión cercana de un paciente y su afección sin dar ningún tratamiento hasta que los signos o síntomas aparezcan o cambien.
New types of treatment are being tested in clinical trials.
En esta sección se resumen los tratamientos que se están estudiando en ensayos clínicos. Es posible que no se mencionen todos los tratamientos nuevos que se están estudiando. La información sobre los ensayos clínicos está disponible en el sitio web del NCI.
Terapia dirigida
La terapia dirigida es un tipo de tratamiento que utiliza medicamentos u otras sustancias para identificar y atacar células cancerosas específicas. Las terapias dirigidas suelen causar menos daño a las células normales que la quimioterapia o la radioterapia.
Se están estudiando diferentes tipos de terapia dirigida para el tratamiento de los gliomas de tronco encefálico:
- La terapia con inhibidores de quinasa bloquea ciertas proteínas, como BRAF y MEK, lo que puede ayudar a impedir el crecimiento y la división de las células cancerosas. Actualmente, se están estudiando el dabrafenib (inhibidor de la quinasa BRAF) y el trametinib (inhibidor de la quinasa MEK) para el tratamiento del glioma focal recién diagnosticado y el glioma recurrente del tronco encefálico.
- La terapia con inhibidores de histona desacetilasa (HDI) puede detener el crecimiento de las células tumorales al bloquear ciertas enzimas necesarias para el crecimiento celular. También actúa como un agente de angiogénesis. Se está investigando el panobinostat para el tratamiento del GPID que no ha respondido a las terapias previas o ha reaparecido.
- Anticuerpo monoclonal usa sistema inmunitario proteínas producidas en el laboratorio para tratar muchas enfermedades, entre ellas el cáncer. Como tratamiento contra el cáncer, estos anticuerpos pueden unirse a un objetivo específico en las células cancerosas u otras células que pueden ayudar a que las células cancerosas crezcan. Los anticuerpos son capaces de matar las células cancerosas, bloquear su crecimiento o evitar que se propaguen. Los anticuerpos monoclonales son administrados por infusión. Pueden utilizarse solos o para transportar medicamentos, toxinas, o material radiactivo directamente a las células cancerosas.
El anticuerpo monoclonal APX005M se une al CD40, un receptor de superficie celular que se encuentra en determinadas células inmunitarias y en algunas células cancerosas. Puede combatir el cáncer reforzando el sistema inmunitario y frenando el crecimiento de las células cancerosas. Se está estudiando en el tratamiento de tumores cerebrales pediátricos que crecen, se extienden o empeoran (progresivos), o en DIPG recién diagnosticados.
¿Cómo actúan los anticuerpos monoclonales para tratar el cáncer? En este video se explica cómo los anticuerpos monoclonales, como el trastuzumab, el pembrolizumab y el rituximab, bloquean moléculas que las células cancerosas necesitan para multiplicarse, marcan células cancerosas para que el sistema inmunitario las destruya o transportan sustancias que dañan estas células.
El tratamiento para el glioma de tronco encefálico infantil puede causar efectos secundarios.
Para obtener más información sobre los efectos secundarios que comienzan durante el tratamiento del cáncer, consulte la página Efectos secundarios.
Los efectos secundarios del tratamiento del cáncer que comienzan después del tratamiento y continúan durante meses o años se denominan efectos tardíos. Los efectos tardíos pueden ser:
- Problemas físicos
- Changes in mood, feelings, thinking, learning, or memory.
- Second cancers (new types of cancer).
Algunos efectos tardíos pueden tratarse o controlarse. Es importante hablar con los pediatras sobre los efectos que el tratamiento del cáncer puede tener en su hijo o hija. Para obtener más información, consulte el resumen del PDQ Efectos tardíos del tratamiento anticanceroso en la niñez.
Patients may want to think about taking part in a clinical trial.
Information about clinical trials is available from the NCI website.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Algunos ensayos clínicos solo incluyen pacientes que aún no han recibido tratamiento. Otros ensayos prueban tratamientos para pacientes cuyo cáncer no ha mejorado. También hay ensayos clínicos que prueban nuevas formas de evitar que el cáncer reaparezca (regrese) o reduzcan los efectos secundarios del tratamiento del cáncer.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Pueden ser necesarias pruebas de seguimiento.
Es posible que se repitan algunas pruebas realizadas para diagnosticar el cáncer o determinar su estadio. Algunas pruebas se repetirán para evaluar la eficacia del tratamiento. Las decisiones sobre continuar, modificar o suspender el tratamiento pueden basarse en los resultados de estas pruebas.
Ciertas pruebas se seguirán realizando periódicamente después de que finalice el tratamiento. Los resultados pueden indicar si la afección de su hijo o hija ha cambiado o si el cáncer ha reaparecido (regresado). Estas pruebas a menudo se denominan pruebas de seguimiento o controles.
Si los resultados de las pruebas de diagnóstico por imágenes realizadas después del tratamiento del GPID muestran una masa en el cerebro, se puede realizar una biopsia para determinar si está compuesta por células tumorales muertas o si están proliferando nuevas células cancerosas. En los niños con expectativa de vida prolongada, se pueden realizar resonancias magnéticas periódicas para monitorear una posible recurrencia del cáncer.
Tratamiento de GPID
For information about the treatments listed below, see the Treatment Option Overview section.
El glioma intrínseco difuso del tronco encefálico (GIPD) infantil recién diagnosticado es un tumor que aún no ha recibido tratamiento. Es posible que el niño haya recibido medicamentos o algún tipo de tratamiento para aliviar los signos o síntomas causados por el tumor.
El tratamiento estándar del GIPD puede consistir en:
- Radioterapia externa.
- Quimioterapia (en bebés)
- Participación en el ensayo clínico de un tratamiento nuevo
Tratamiento del glioma de tronco encefálico focal
For information about the treatments listed below, see the Treatment Option Overview section.
El glioma focal infantil recién diagnosticado es un tumor que aún no ha recibido tratamiento. Es posible que el niño haya recibido medicamentos o algún tipo de tratamiento para aliviar los signos o síntomas causados por el tumor.
El tratamiento del glioma focal puede consistir en:
- Cirugía para extirpar el tumor seguida de quimioterapia y/o radioterapia externa
- Observación de tumores pequeños que crecen lentamente. La desviación del líquido cefalorraquídeo se puede realizar cuando hay exceso de líquido en el cerebro.
- Radioterapia interna con semillas radiactivas, con o sin quimioterapia, cuando el tumor no puede extirparse mediante cirugía
- Un ensayo clínico de terapia dirigida con un inhibidor de la quinasa BRAF (dabrafenib) combinado con un inhibidor de MEK (trametinib), para ciertos tumores que no se pueden extirpar mediante cirugía
El tratamiento del glioma del tronco encefálico en niños con neurofibromatosis tipo 1 puede consistir en la observación, ya que los tumores suelen crecer lentamente en estos casos y es posible que no requieran un tratamiento específico durante años.
Tratamiento del glioma de tronco encefálico infantil progresivo o recurrente
Cuando el cáncer no mejora con el tratamiento o vuelve a aparecer, los cuidados paliativos son una parte importante del plan de tratamiento del niño. Incluyen apoyo físico, psicológico, social y espiritual tanto para el niño como para la familia. El objetivo de los cuidados paliativos es ayudar a controlar los síntomas y darle al niño la mejor calidad de vida posible. Los padres pueden tener dudas sobre si continuar con el tratamiento o qué tipo de tratamiento es el mejor para su hijo o hija. El equipo médico puede ofrecer información para ayudarles a tomar estas decisiones.
For information about the treatments listed below, see the Treatment Option Overview section.
Se puede administrar más radioterapia a niños con glioma pontino intrínseco difuso (GPID) progresivo o recurrente que respondieron favorablemente a la radioterapia inicial. El tratamiento del GPID progresivo o recurrente también puede consistir en:
- Un ensayo clínico que examina una muestra del tumor del paciente para identificar posibles cambios genéticos. El tipo de terapia dirigida que se administrará dependerá del tipo de alteración genética detectada.
- Un ensayo clínico de terapia dirigida que evalúa el uso de un inhibidor de la histona desacetilasa (panobinostat) o un anticuerpo monoclonal (APX005M)
El tratamiento del glioma focal de tronco encefálico infantil recurrente puede consistir en:
- Una segunda cirugía para extirpar el tumor
- Radioterapia externa.
- Quimioterapia.
- Un ensayo clínico que examina una muestra del tumor del paciente para identificar posibles cambios genéticos. El tipo de terapia dirigida que se administrará dependerá del tipo de alteración genética detectada.
Más información sobre los tumores cerebrales infantiles
Para obtener más información sobre los tumores cerebrales infantiles, consulte:
- Terapias dirigidas contra el cáncer
- Consorcio de tumores cerebrales pediátricos (PBTC)
- Comunicación en la atención del cáncer
- Planificación de la transición a los cuidados paliativos en el cáncer avanzado
Para obtener más información sobre el cáncer infantil y otros recursos generales sobre el cáncer, consulte:
- El cáncer
- Cánceres infantiles
- CureSearch para el cáncer infantil
- Efectos tardíos del tratamiento del cáncer infantil
- Adolescentes y adultos jóvenes con cáncer
- Niños con cáncer: una guía para padres
- El cáncer en los niños y los adolescentes
- Estadificación
- Cómo hacer frente al cáncer
- Preguntas para el médico sobre el cáncer
- Para sobrevivientes y cuidadores
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen del PDQ sobre el cáncer contiene información actualizada del tratamiento del glioma de tronco encefálico infantil. El propósito es informar y ayudar a los pacientes, sus familiares y cuidadores. No da pautas ni recomendaciones formales para tomar decisiones relacionadas con la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
La información de este resumen para pacientes procede de la versión para profesionales de la salud, la cual es revisada y actualizada periódicamente por el comité editorial del PDQ sobre el tratamiento pediátrico según sea necesario.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre el tratamiento pediátrico. Tratamiento del glioma de tronco encefálico infantil (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Actualizado:
URL de origen: https://www.cancer.gov/node/4266/syndication
Agencia de origen: National Cancer Institute (NCI)
Fecha de captura: 2013-09-14 09:02:07.0