








Tratamiento del astrocitoma
If your child is diagnosed with astrocytoma, a tumor that affects cells of the brain’s supportive tissue, you want experienced, compassionate experts providing their care. You’ll find it at Montefiore Einstein Comprehensive Cancer Center at the Children’s Hospital at Montefiore Einstein (CHAM). CHAM provides state-of-the-art care for children from the New York metropolitan area, across the nation and around the world.
We are a premier academic children’s hospital known for our clinical excellence and innovative research. Our multidisciplinary and collaborative approach to patient care across CHAM and our Comprehensive Cancer Center ensures your child will receive the best care in a supportive and nurturing environment. This care includes the most advanced therapies, access to the latest ensayos clínicos and comprehensive psychosocial support, not only for your child, but for your entire family.
We bring a team of specialists to each patient we work with. It includes pediatric oncologists, surgical oncologists, oncology nurses, radiation oncologists, diagnostic radiologists, pathologists, psychiatrists, psychologists, physical and occupational therapists, social workers, child life specialists and others. They create a caring, nurturing environment that makes you and your child as comfortable as possible.
Si lo que usted desea es lo mejor para su hijo, acuda a los especialistas del Centro Oncológico Integral Montefiore Einstein en CHAM, quienes se dedican con pasión a erradicar el cáncer y a atender todas las necesidades de salud de su hijo.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Childhood Astrocytomas Treatment (PDQ®)–Patient Version
General Information About Childhood Astrocytomas
Puntos clave
- Childhood astrocytomas are tumors that start in the star-shaped brain cells called astrocytes.
- Astrocytomas may be low-grade or high-grade.
- The central nervous system controls many important body functions.
- The cause of most childhood brain tumors is not known.
- The signs and symptoms of astrocytomas are not the same in every child.
- Tests that examine the brain and spinal cord are used to detect (find) childhood astrocytomas.
- Childhood astrocytomas are usually diagnosed and removed in surgery.
- Certain factors affect prognosis (chance of recovery) and treatment options.
Childhood astrocytomas are tumors that start in the star-shaped brain cells called astrocytes.
An astrocyte is a type of glial cell. Glial cells hold nerve cells in place, bring food and oxygen to them, and help protect them from disease, such as infection. Gliomas are tumors that form from glial cells. An astrocytoma is a type of glioma.
Astrocytoma is the most common type of glioma diagnosed in children. It can form anywhere in the central nervous system (brain and spinal cord).
This summary is about the treatment of tumors that begin in astrocytes in the brain (primary brain tumors). Metastatic brain tumors are formed by cancer cells that begin in other parts of the body and spread to the brain. Treatment of metastatic brain tumors is not discussed here.
Brain tumors can occur in both children and adults. However, treatment for children may be different than treatment for adults. See the following PDQ summaries for more information about other types of brain tumors in children and adults:
Astrocytomas may be low-grade or high-grade.
Low-grade brain tumors grow and press on nearby areas of the brain. They rarely spread into other tissues. High-grade brain tumors are likely to grow quickly and spread into other brain tissue. When a tumor grows into or presses on an area of the brain, it may stop that part of the brain from working the way it should. Both low-grade and high-grade brain tumors can cause signs and symptoms and almost all need treatment.
The central nervous system controls many important body functions.
Astrocytomas are most common in these parts of the central nervous system (CNS):
- Cerebrum: The largest part of the brain, at the top of the head. The cerebrum controls thinking, learning, problem-solving, speech, emotions, reading, writing, and voluntary movement.
- Cerebellum: The lower, back part of the brain (near the middle of the back of the head). The cerebellum controls voluntary movement, balance, and posture.
- Brain stem: The part that connects the brain to the spinal cord, in the lowest part of the brain (just above the back of the neck). The brain stem controls breathing, heart rate, and the nerves and muscles used in seeing, hearing, walking, talking, and eating.
- Hypothalamus: The area in the middle of the base of the brain. It controls body temperature, hunger, and thirst.
- Visual pathway: The group of nerves that connect the eye with the brain.
- Spinal cord: The column of nerve tissue that runs from the brain stem down the center of the back. It is covered by three thin layers of tissue called membranes. The spinal cord and membranes are surrounded by the vertebrae (back bones). Spinal cord nerves carry messages between the brain and the rest of the body, such as a message from the brain to cause muscles to move or a message from the skin to the brain to feel touch.
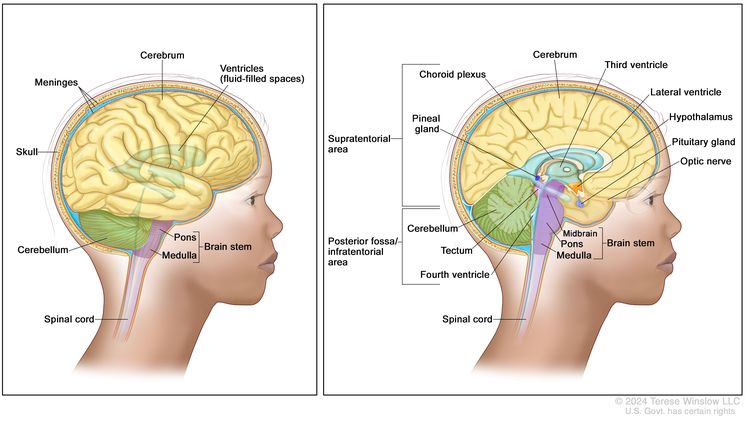
Anatomía del encéfalo. El área supratentorial (la parte superior del cerebro) contiene el cerebro, el ventrículo lateral y el tercer ventrículo (el líquido cefalorraquídeo se muestra en azul), el plexo coroideo, la glándula pineal, el hipotálamo, la glándula pituitaria y el nervio óptico. La fosa posterior/área infratentorial (la parte posterior inferior del encéfalo) contiene el cerebelo, el techo, el cuarto ventrículo y el tronco encefálico (mesencéfalo, protuberancia y bulbo raquídeo). El tentorio separa el área supratentorial del área infratentorial (panel derecho). El cráneo y las meninges protegen el cerebro y la médula espinal (panel izquierdo).
The cause of most childhood brain tumors is not known.
Anything that increases your risk of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer. Talk with your child's doctor if you think your child may be at risk. Possible risk factors for astrocytoma include:
- Past radiation therapy to the brain.
- Having certain genetic disorders, such as neurofibromatosis type 1 (NF1) or tuberous sclerosis.
The signs and symptoms of astrocytomas are not the same in every child.
Signs and symptoms depend on the following:
- Where the tumor forms in the brain or spinal cord.
- El tamaño del tumor
- La rapidez con la que crece el tumor
- The child's age and development.
Some tumors do not cause signs or symptoms. Signs and symptoms may be caused by childhood astrocytomas or by other conditions. Check with your child's doctor if your child has any of the following:
- Dolor de cabeza matinal o dolor de cabeza que desaparece después de vomitar
- Náuseas y vómitos
- Vision, hearing, and speech problems.
- Pérdida del equilibrio y dificultad para caminar
- Worsening handwriting or slow speech.
- Weakness or change in feeling on one side of the body.
- Somnolencia inusual
- Menor o mayor energía de lo habitual
- Change in personality or behavior.
- Convulsiones.
- Weight loss or weight gain for no known reason.
- Increase in the size of the head (in infants).
Tests that examine the brain and spinal cord are used to detect (find) childhood astrocytomas.
Se pueden utilizar las siguientes pruebas y procedimientos:
- Examen físico and health history: An exam of the body to check general signs of health. This includes checking for signs of disease, such as lumps or anything else that seems unusual. A history of the patient’s health habits and past illnesses and treatments will also be taken.
- Examen neurológico: una serie de preguntas y pruebas para evaluar el cerebro, la médula espinal y la función nerviosa. El examen verifica el estado mental, la coordinación, la capacidad de una persona para caminar con normalidad y lo bien que funcionan los músculos, los sentidos y los reflejos. También se conoce como evaluación neurológica.
- Visual field exam: An exam to check a person’s field of vision (the total area in which objects can be seen). This test measures both central vision (how much a person can see when looking straight ahead) and peripheral vision (how much a person can see in all other directions while staring straight ahead). The eyes are tested one at a time. The eye not being tested is covered.
- Resonancia magnética (magnetic resonance imaging) with gadolinio: A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of the brain and spinal cord. A substance called gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI). Sometimes magnetic resonance spectroscopy (MRS) is done during the same MRI scan to look at the chemical makeup of the brain tissue.
Childhood astrocytomas are usually diagnosed and removed in surgery.
If doctors think there may be an astrocytoma, a biopsy may be done to remove a sample of tissue. For tumors in the brain, a part of the skull is removed and a needle is used to remove tissue. Sometimes, the needle is guided by a computer. A pathologist views the tissue under a microscope to look for cancer cells. If cancer cells are found, the doctor may remove as much tumor as safely possible during the same surgery. Because it can be hard to tell the difference between types of brain tumors, you may want to have your child's tissue sample checked by a pathologist who has experience in diagnosing brain tumors.
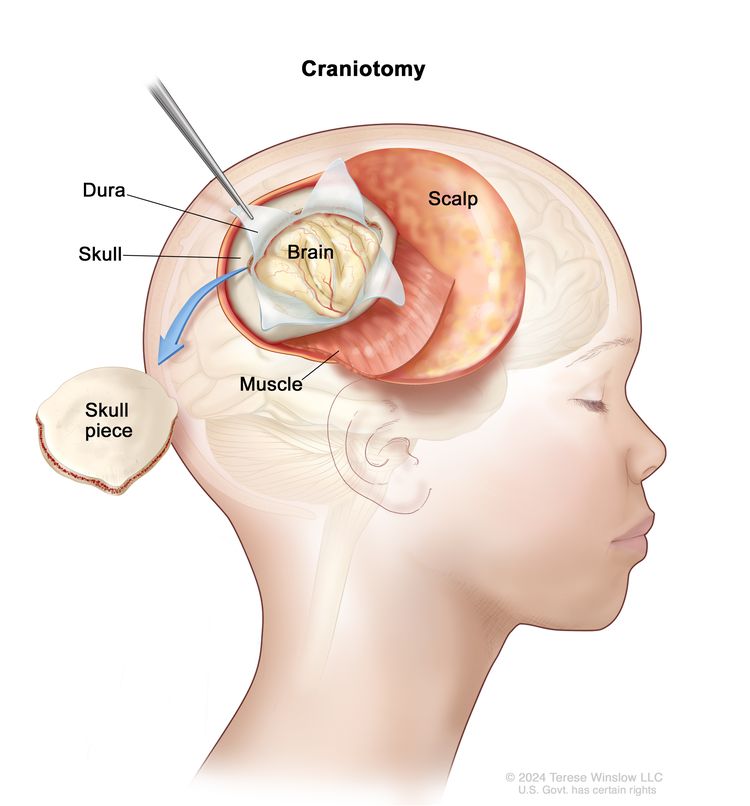
Craneotomía. Se realiza una abertura y se extrae una pieza del cráneo para exponer una parte del cerebro.
The following test may be done on the tissue that was removed:
- Inmunohistoquímica: A laboratory test that uses antibodies to check for certain antigens (markers) in a sample of a patient’s tissue. The antibodies are usually linked to an enzyme or a fluorescent dye. After the antibodies bind to a specific antigen in the tissue sample, the enzyme or dye is activated, and the antigen can then be seen under a microscope. This type of test is used to help diagnose cancer and to help tell one type of cancer from another type of cancer. An MIB-1 test is a type of immunohistochemistry that checks tumor tissue for an antigen called MIB-1. This may show how fast a tumor is growing.
- Las pruebas moleculares: A laboratory test to check for certain genes, proteins, or other molecules in a sample of blood or bone marrow. Molecular tests also check for certain changes in a gene or chromosome that may cause or affect the chance of developing a brain tumor. A molecular test may be used to help plan treatment, find out how well treatment is working, or make a prognosis.
Sometimes tumors form in a place that makes them hard to remove. If removing the tumor may cause severe physical, emotional, or learning problems, a biopsy is done and more treatment is given after the biopsy.
Children who have a rare genetic condition called NF1 may form a low-grade astrocytoma in the area of the brain that controls vision and may not need a biopsy. If the tumor does not continue to grow or symptoms do not occur, surgery to remove the tumor may not be needed.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis and treatment options depend on the following:
- Whether the tumor is a low-grade or high-grade astrocytoma.
- Where the tumor has formed in the CNS and if it has spread to nearby tissue or to other parts of the body.
- La rapidez con la que está creciendo el tumor
- The child's age.
- Whether cancer cells remain after surgery.
- Whether there are changes in certain genes.
- Whether the child has NF1 or tuberous sclerosis.
- Whether the child has diencephalic syndrome (a condition which slows physical growth).
- Whether the astrocytoma has just been diagnosed or has recurred (come back).
For recurrent astrocytoma, prognosis and treatment depend on how much time passed between the time treatment ended and the time the astrocytoma recurred.
Stages of Childhood Astrocytomas
Puntos clave
- The grade of the tumor is used to plan cancer treatment.
- Low-grade astrocytomas
- High-grade astrocytomas
- Sometimes childhood astrocytomas continue to grow or come back after treatment.
The grade of the tumor is used to plan cancer treatment.
La estadificación es el proceso que se utiliza para determinar la extensión del cáncer y si se ha propagado. Es importante conocer el estadio para planificar el tratamiento.
However, there is no standard staging system for childhood astrocytoma. Instead, treatment is based on the following:
- Whether the tumor is low grade or high grade.
- Whether the tumor is newly diagnosed or recurrent (has come back after treatment).
The grade of the tumor describes how abnormal the cancer cells look under a microscope and how quickly the tumor is likely to grow and spread.
The following grades are used:
Low-grade astrocytomas
Low-grade astrocytomas are slow-growing and rarely spread to other parts of the brain and spinal cord or other parts of the body. There are many types of low-grade astrocytomas. Low-grade astrocytomas can be either:
- Grade I tumors–pilocytic astrocytoma, subependymal giant cell astrocytoma, or angiocentric glioma.
- Grade II tumors–diffuse astrocytoma, pleomorphic xanthoastrocytoma, or choroid glioma of the third ventricle.
Children who have neurofibromatosis type 1 (NF1) may have more than one low-grade tumor in the brain. Children who have tuberous sclerosis have an increased risk of subependymal giant cell astrocytoma.
High-grade astrocytomas
High-grade astrocytomas are fast-growing and often spread within the brain and spinal cord. There are several types of high-grade astrocytomas. High grade astrocytomas can be either:
- Grade III tumors–anaplastic astrocytoma or anaplastic pleomorphic xanthoastrocytoma.
- Grade IV tumors–glioblastoma or diffuse midline glioma.
Childhood astrocytomas usually do not spread to other parts of the body.
Sometimes childhood astrocytomas continue to grow or come back after treatment.
Progressive childhood astrocytoma is cancer that continues to grow, spread, or get worse. Progressive disease may be a sign that the cancer has become refractory (does not respond) to treatment.
A recurrent childhood astrocytoma is cancer that has recurred (come back) after it has been treated. The cancer may come back in the same place as the first tumor or in other parts of the body. High-grade astrocytomas often recur within 3 years either in the place where the cancer first formed or somewhere else in the CNS.
Treatment Option Overview
Puntos clave
- There are different types of treatment for patients with childhood astrocytoma.
- Children with astrocytomas should have their treatment planned by a team of health care providers who are experts in treating childhood brain tumors.
- Childhood brain tumors may cause signs or symptoms that begin before the cancer is diagnosed and continue for months or years.
- Six types of treatment are used:
- Cirugía
- Observation
- Radioterapia
- Quimioterapia
- Quimioterapia de dosis alta con trasplante de células madre
- Terapia dirigida
- New types of treatment are being tested in clinical trials.
- Inmunoterapia
- If fluid builds up around the brain and spinal cord, a cerebrospinal fluid diversion procedure may be done.
- Treatment for childhood astrocytomas may cause side effects.
- Patients may want to think about taking part in a clinical trial.
- Patients can enter clinical trials before, during, or after starting their cancer treatment.
- Pueden ser necesarias pruebas de seguimiento.
There are different types of treatment for patients with childhood astrocytoma.
Different types of treatment are available for children with astrocytomas. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment.
Because cancer in children is rare, taking part in a clinical trial should be considered. Some clinical trials are open only to patients who have not started treatment.
Children with astrocytomas should have their treatment planned by a team of health care providers who are experts in treating childhood brain tumors.
Treatment will be overseen by a pediatric oncologist, a doctor who specializes in treating children with cancer. The pediatric oncologist works with other healthcare providers who are experts in treating children with brain tumors and who specialize in certain areas of medicine. These may include the following specialists:
Childhood brain tumors may cause signs or symptoms that begin before the cancer is diagnosed and continue for months or years.
Signs or symptoms caused by the tumor may begin before diagnosis. These signs or symptoms may continue for months or years. It is important to talk with your child's doctors about signs or symptoms caused by the tumor that may continue after treatment.
Six types of treatment are used:
Cirugía
Surgery is used to diagnose and treat childhood astrocytoma, as discussed in the General Information section of this summary. After surgery an MRI (magnetic resonance imaging) is done to see if any cancer cells remain. If cancer cells are found, further treatment depends on:
- Where the remaining cancer cells are.
- El grado del tumor
- Edad del niño
After the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given chemotherapy or radiation therapy after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
Observation
Observation is closely monitoring a patient’s condition without giving any treatment until signs or symptoms appear or change. Observation may be used:
- If the patient has no symptoms, such as patients with neurofibromatosis type1.
- If the tumor is small and is found when a different health problem is being diagnosed or treated.
- After the tumor is removed by surgery until signs or symptoms appear or change.
Radioterapia
La radioterapia es un tratamiento contra el cáncer que utiliza rayos X de alta energía u otros tipos de radiación para matar las células cancerosas o evitar que crezcan. Para la radioterapia externa se usa una máquina que envía la radiación hacia la zona con cáncer desde el exterior del cuerpo.
Certain ways of giving radiation therapy can help keep radiation from damaging nearby healthy tissue. These types of radiation therapy include the following:
- Conformal radiation therapy: Conformal radiation therapy is a type of external radiation therapy that uses a computer to make a 3-dimensional (3-D) picture of the tumor and shapes the radiation beams to fit the tumor.
- Intensity-modulated radiation therapy (IMRT): IMRT is a type of 3-dimensional (3-D) external radiation therapy that uses a computer to make pictures of the size and shape of the tumor. Thin beams of radiation of different intensities (strengths) are aimed at the tumor from many angles.
- Stereotactic radiation therapy: Stereotactic radiation therapy is a type of external radiation therapy. A rigid head frame is attached to the skull to keep the head still during the radiation treatment. A machine aims radiation directly at the tumor. The total dose of radiation is divided into several smaller doses given over several days. This procedure is also called stereotactic external-beam radiation therapy and stereotaxic radiation therapy.
- Radioterapia con haz de protones: la radioterapia con haz de protones es un tipo de radioterapia externa de alta energía que utiliza corrientes de protones (partículas diminutas con carga positiva) para destruir las células tumorales. Este tipo de tratamiento puede reducir la cantidad de daño por radiación al tejido sano cerca de un tumor.
The way the radiation therapy is given depends on the type of tumor and where the tumor formed in the brain or spinal cord. External radiation therapy is used to treat childhood astrocytomas.
Radiation therapy to the brain can affect growth and development, especially in young children. For children younger than 3 years, chemotherapy may be given instead, to delay or reduce the need for radiation therapy.
Quimioterapia
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy). Combination chemotherapy is the use of more than one anticancer drug.
The way the chemotherapy is given depends on the type of tumor and where the tumor formed in the brain or spinal cord. Systemic combination chemotherapy is used in the treatment of children with astrocytoma. High-dose chemotherapy may be used in the treatment of children with newly diagnosed high-grade astrocytoma.
Quimioterapia de dosis alta con trasplante de células madre
High doses of chemotherapy are given to kill cancer cells. Healthy cells, including blood-forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the patient completes chemotherapy, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
For high-grade astrocytoma that has come back after treatment, high-dose chemotherapy with stem cell transplant is used if there is only a small amount of tumor.
Terapia dirigida
La terapia dirigida es un tipo de tratamiento que utiliza medicamentos u otras sustancias para identificar y atacar células cancerosas específicas. Las terapias dirigidas suelen causar menos daño a las células normales que la quimioterapia o la radioterapia.
There are different types of targeted therapy:
- Anticuerpos monoclonales: los anticuerpos monoclonales son proteínas del sistema inmunitario proteínas made in the laboratory to treat many diseases, including cancer. As a cancer treatment, these anticuerpos can attach to a specific target on cancer cells or other cells that may help cancer cells grow. The antibodies are able to then kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxinaso radioactivo material directamente a las células cancerosas. Bevacizumab is a monoclonal antibody and vascular endothelial growth factor inhibitor that binds to a protein called vascular endothelial growth factor (VEGF) and may prevent the growth of new vasos sanguíneos that tumors need to grow. Bevacizumab is used to treat childhood astrocytoma.
¿Cómo actúan los anticuerpos monoclonales para tratar el cáncer? En este video se explica cómo los anticuerpos monoclonales, como el trastuzumab, el pembrolizumab y el rituximab, bloquean moléculas que las células cancerosas necesitan para multiplicarse, marcan células cancerosas para que el sistema inmunitario las destruya o transportan sustancias que dañan estas células. - Protein kinase inhibitors work in different ways. There are several kinds of protein kinase inhibitors.
- mTOR inhibitors: This treatment stops the protein that helps cells divide and survive. Everolimus and sirolimus are mTOR inhibitors used to treat childhood subependymal giant cell astrocytomas.
- BRAF inhibitors: This treatment blocks the activity of proteins needed for cell growth and may kill cancer cells. The BRAF gene is found in a mutated (changed) form in some gliomas and blocking it may help keep cancer cells from growing. The combination of the BRAF inhibitors dabrafenib and trametinib are being studied to treat newly diagnosed low-grade astrocytomas or high-grade astrocytomas that have recurred or stopped responding to treatment. Dabrafenib and trametinib given after radiation are also being studied to treat newly diagnosed high-grade gliomas.
- MEK inhibitors: This treatment blocks proteins needed for cell growth and may kill cancer cells. The MEK inhibitor is being studied to treat low-grade astrocytoma that has recurred or stopped responding to treatment. It is also being studied in combination with chemotherapy to treat newly diagnosed NF1-associated low-grade gliomas.
See Drugs Approved for Brain Tumors for more information.
New types of treatment are being tested in clinical trials.
En esta sección se resumen los tratamientos que se están estudiando en ensayos clínicos. Es posible que no se mencionen todos los tratamientos nuevos que se están estudiando. La información sobre los ensayos clínicos está disponible en el sitio web del NCI.
Inmunoterapia
Immunotherapy is a treatment that uses the patient's immune system to fight cancer. Substances made by the body or made in a laboratory are used to boost, direct, or restore the body's natural defenses against cancer. This cancer treatment is a type of biologic therapy.
- Immune checkpoint inhibitor terapia: Some types of immune cells, such as células T, and some cancer cells have certain proteins, called checkpoint proteins, on their surface that keep respuestas inmunes in check. When cancer cells have large amounts of these proteins, they will not be attacked and killed by T cells. Immune checkpoint inhibitors block these proteins and the ability of T cells to kill cancer cells is increased.
- PD-1 and PD-L1 inhibitor therapy: PD-1 is a protein on the surface of T cells that helps keep the body’s immune responses in check. PD-L1 is a protein found on some types of cancer cells. When PD-1 attaches to PD-L1, it stops the T cell from killing the cancer cell. PD-1 and PD-L1 inhibitors keep PD-1 and PD-L1 proteins from attaching to each other. This allows the T cells to kill cancer cells. PD-1 inhibitors are being studied to treat high-grade astrocytoma that has recurred.
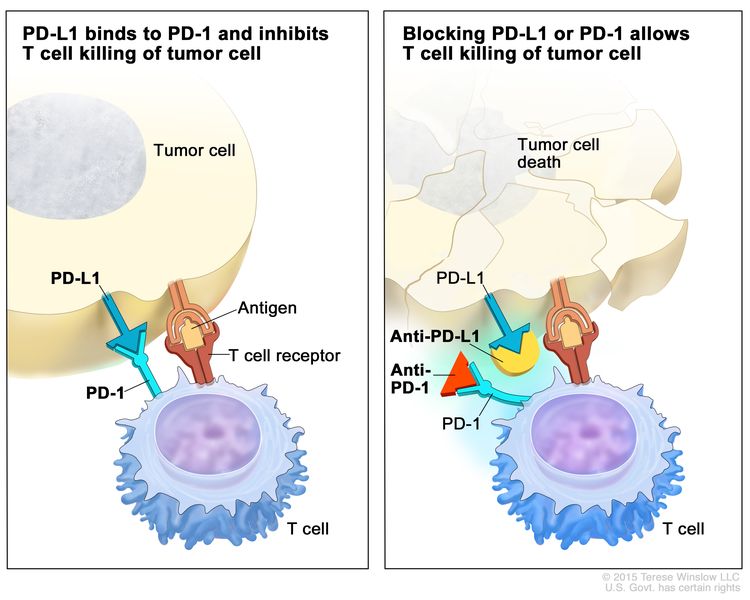
Inhibidor de puestos de control inmunitario. Las proteínas de puestos de control, como PD-L1 en las células tumorales y PD-1 en las células T, regulan las respuestas inmunitarias. La unión de PD-L1 y PD-1 evita que las células T destruyan las células tumorales en el cuerpo (panel izquierdo). El bloqueo de esta unión con un inhibidor del puesto de control inmunitario (anti-PD-L1 o anti-PD-1) permite que las células T eliminen las células tumorales (panel derecho).
If fluid builds up around the brain and spinal cord, a cerebrospinal fluid diversion procedure may be done.
Cerebrospinal fluid diversion is a method used to drain fluid that has built up around the brain and spinal cord. A shunt (long, thin tube) is placed in a ventricle (fluid-filled space) of the brain and threaded under the skin to another part of the body, usually the abdomen. The shunt carries extra fluid away from the brain so it may be absorbed elsewhere in the body.
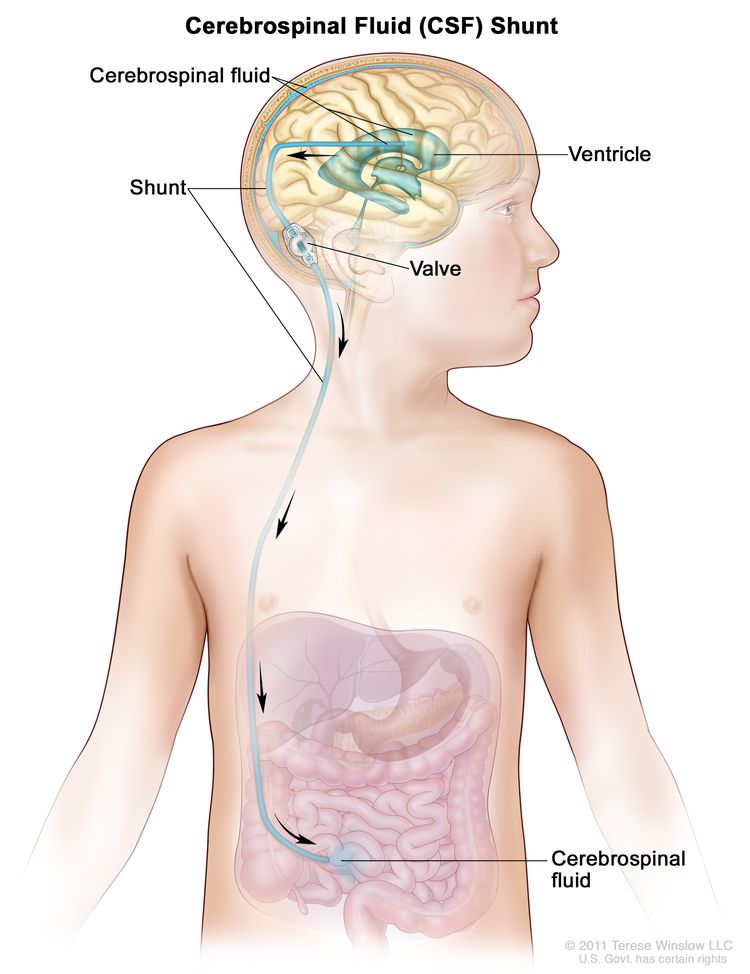
Una desviación o derivación de líquido cefalorraquídeo (LCR) es un tubo largo y delgado que transporta el exceso de LCR fuera del cerebro para que pueda ser absorbido en otras partes del cuerpo. Se coloca en un ventrículo (espacio lleno de líquido) del cerebro y se pasa debajo de la piel hasta otra parte del cuerpo, generalmente el abdomen. La derivación incluye una válvula que controla el flujo del LCR.
Treatment for childhood astrocytomas may cause side effects.
Para obtener más información sobre los efectos secundarios que comienzan durante el tratamiento del cáncer, consulte la página Efectos secundarios.
Side effects from cancer treatment that begin after treatment and continue for months or years are called late effects. Late effects of cancer treatment may include the following:
- Physical problems that affect the following:
- Vision problems, including blindness.
- Blood vessel problems.
- Endocrine function.
- Changes in mood, feelings, thinking, learning, or memory.
- Second cancers (new types of cancer).
Some late effects may be treated or controlled. It is important to talk with your child's doctors about the effects cancer treatment can have on your child. (See the PDQ summary on Late Effects of Treatment for Childhood Cancer for more information.)
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Algunos ensayos clínicos solo incluyen pacientes que aún no han recibido tratamiento. Otros ensayos prueban tratamientos para pacientes cuyo cáncer no ha mejorado. También hay ensayos clínicos que prueban nuevas formas de evitar que el cáncer reaparezca (regrese) o reduzcan los efectos secundarios del tratamiento del cáncer.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Pueden ser necesarias pruebas de seguimiento.
Some of the tests that were done to diagnose the cancer or to find out the stage of the cancer may be repeated. (See the General Information section for a list of tests.) Some tests will be repeated in order to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Regular MRIs will continue to be done after treatment has ended. The results of the MRI can show if your child's condition has changed or if the astrocytoma has recurred (come back). If the results of the MRI show a mass in the brain, a biopsy may be done to find out if it is made up of dead tumor cells or if new cancer cells are growing.
Treatment of Childhood Low-Grade Astrocytomas
For information about the treatments listed below, see the Treatment Option Overview section.
When the tumor is first diagnosed, treatment for childhood low-grade astrocytoma depends on where the tumor is, and is usually surgery. An MRI is done after surgery to see if there is tumor remaining.
If the tumor was completely removed by surgery, more treatment may not be needed and the child is closely watched to see if signs or symptoms appear or change. This is called observation.
If there is tumor remaining after surgery, treatment may include the following:
- Observation.
- Combination chemotherapy with or without radiation therapy.
- Radiation therapy, which may include conformal radiation therapy, intensity-modulated radiation therapy, proton beam radiation therapy, or stereotactic radiation therapy, when the tumor begins to grow again.
- Targeted therapy with mTOR inhibitors (everolimus and sirolimus) to treat subependymal giant cell astrocytoma.
- A clinical trial of targeted therapy with a MEK inhibitor (selumetinib).
In some cases, observation is used for children who have a visual pathway glioma. In other cases, treatment may include surgery to remove the tumor, radiation therapy, or chemotherapy. A goal of treatment is to save as much vision as possible. In most patients who receive radiation therapy, the tumor is controlled, but changes in vision may develop. These changes are most likely to occur within 2 years after radiation therapy. The effect of tumor growth on the child's vision will be closely followed during and after treatment.
Children with neurofibromatosis type 1 (NF1) may not need treatment unless the tumor grows or signs or symptoms, such as vision problems, appear. When the tumor grows or signs or symptoms appear, treatment may include surgery to remove the tumor, radiation therapy, and/or chemotherapy.
Children with tuberous sclerosis may develop low-grade tumors in the brain called subependymal giant cell astrocytoma (SEGAs). Targeted therapy with everolimus or sirolimus may be used instead of surgery, to shrink the tumors.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Treatment of Progressive or Recurrent Childhood Low-Grade Astrocytomas
For information about the treatments listed below, see the Treatment Option Overview section.
When low-grade astrocytoma recurs after treatment, it usually comes back where the tumor first formed. Before more cancer treatment is given, imaging tests, biopsy, or surgery are done to find out if there is cancer and how much there is.
Treatment of progressive or recurrent childhood low-grade astrocytoma may include the following:
- A second surgery to remove the tumor, if surgery was the only treatment given when the tumor was first diagnosed.
- Radiation therapy to the tumor only, if radiation therapy was not used when the tumor was first diagnosed. Conformal radiation therapy may be given.
- Chemotherapy, if the tumor recurred where it cannot be removed by surgery.
- Targeted therapy with a monoclonal antibody (bevacizumab) with or without chemotherapy.
- A clinical trial that checks a sample of the patient's tumor for certain gene changes. The type of targeted therapy that will be given to the patient depends on the type of gene change.
- A clinical trial of targeted therapy with a BRAF inhibitor (dabrafenib) or a MEK inhibitor (selumetinib).
- A clinical trial of targeted therapy with an mTOR inhibitor (everolimus).
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Treatment of Childhood High-Grade Astrocytomas
For information about the treatments listed below, see the Treatment Option Overview section.
Treatment of newly diagnosed childhood high-grade astrocytoma may include the following:
- Surgery to remove the tumor, followed by chemotherapy and/or radiation therapy.
- A clinical trial of targeted therapy with a combination of BRAF inhibitors (dabrafenib and trametinib) after radiation therapy to treat newly diagnosed high-grade glioma that has mutations in the BRAF gene.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Treatment of Recurrent Childhood High-Grade Astrocytomas
For information about the treatments listed below, see the Treatment Option Overview section.
When high-grade astrocytoma recurs after treatment, it usually comes back where the tumor first formed. Before more cancer treatment is given, imaging tests, biopsy, or surgery are done to find out if there is cancer and how much there is.
Treatment of recurrent childhood high-grade astrocytoma may include the following:
- Cirugía para extirpar el tumor
- High-dose chemotherapy with stem cell transplant.
- Radioterapia.
- Targeted therapy with a BRAF inhibitor (vemurafenib or dabrafenib).
- A clinical trial of immunotherapy with an immune checkpoint inhibitor.
- A clinical trial that checks a sample of the patient's tumor for certain gene changes. The type of targeted therapy that will be given to the patient depends on the type of gene change.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
To Learn More About Childhood Astrocytomas
For more information about childhood astrocytomas, see the following:
- Terapias dirigidas contra el cáncer
- Consorcio de tumores cerebrales pediátricos (PBTC)
- Immunotherapy to Treat Cancer
Para obtener más información sobre el cáncer infantil y otros recursos generales sobre el cáncer, consulte:
- El cáncer
- Cánceres infantiles
- CureSearch para el cáncer infantil
- Efectos tardíos del tratamiento del cáncer infantil
- Adolescentes y adultos jóvenes con cáncer
- Niños con cáncer: una guía para padres
- El cáncer en los niños y los adolescentes
- Estadificación
- Cómo hacer frente al cáncer
- Preguntas para el médico sobre el cáncer
- Para sobrevivientes y cuidadores
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
This PDQ cancer information summary has current information about the treatment of childhood astrocytomas. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
La información de este resumen para pacientes procede de la versión para profesionales de la salud, la cual es revisada y actualizada periódicamente por el comité editorial del PDQ sobre el tratamiento pediátrico según sea necesario.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre el tratamiento pediátrico. Tratamiento de los astrocitomas infantiles (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Updated:
Source URL: https://www.cancer.gov/node/6395/syndication
Agencia de origen: National Cancer Institute (NCI)
Fecha de captura: 2013-09-14 09:03:29.0