








Tratamiento del linfoma de Hodgkin
Acceda a una atención excepcional para el linfoma de Hodgkin infantil, un tipo de cáncer que afecta al sistema linfático, en el Centro Oncológico Integral Montefiore Einstein del Hospital Infantil Montefiore Einstein (CHAM) . Ofrecemos una amplia gama de terapias oncológicas avanzadas en un entorno afectuoso y de apoyo.
Para brindar la mejor atención posible, contamos con un equipo de médicos, especialistas y personal de apoyo de renombre mundial, incluyendo expertos reconocidos a nivel nacional en trasplante de médula ósea pediátrico. Como hospital de investigación, trabajamos para mejorar la seguridad y la eficacia del trasplante de médula ósea. Nuestros médicos, científicos e investigadores realizan activamente investigaciones para optimizar la eficacia de este procedimiento. Gracias a su trabajo, los niños tienen acceso a los ensayos clínicos más recientes. Nuestro equipo también aplica los avances más innovadores en biología del cáncer, inmunología, farmacología y otras áreas para tratar a nuestros pacientes con la mayor eficacia.
Si lo que busca es lo mejor para su hijo, acuda a los especialistas atentos y experimentados del Centro Oncológico Integral Montefiore Einstein en CHAM, quienes se dedican con pasión a erradicar el cáncer y a atender todas las necesidades de salud de su hijo.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Tratamiento del linfoma de Hodgkin infantil (PDQ®): versión para pacientes
Información general sobre el linfoma de Hodgkin infantil
Puntos clave
- El linfoma de Hodgkin infantil es un cáncer que se desarrolla en el sistema linfático.
- Los dos tipos principales de linfoma de Hodgkin infantil son el clásico y el nodular con predominio linfocítico.
- La infección por el virus de Epstein-Barr y un historial de linfoma de Hodgkin en la familia pueden aumentar el riesgo de desarrollar linfoma de Hodgkin infantil.
- Los signos del linfoma de Hodgkin infantil son inflamación de los ganglios linfáticos, fiebre, sudores nocturnos profusos y pérdida de peso.
- Para diagnosticar y estadificar el linfoma de Hodgkin infantil se utilizan pruebas que examinan el sistema linfático y otras partes del cuerpo.
- Es posible que desee obtener una segunda opinión.
- Certain factors affect prognosis (chance of recovery) and treatment options.
El linfoma de Hodgkin infantil es un cáncer que se desarrolla en el sistema linfático.
El sistema linfático forma parte del sistema inmunitario. Ayuda a proteger el cuerpo de infecciones y enfermedades.
El sistema linfático está formado por:
- Linfa: es un líquido incoloro y acuoso que viaja a través de los vasos linfáticos y transporta linfocitos B y T. Los linfocitos son un tipo de glóbulo blanco.
- Vasos linfáticos: red de tubos delgados que recogen la linfa de diferentes partes del cuerpo y la devuelven al torrente sanguíneo.
- Ganglios linfáticos: son pequeñas estructuras con forma de frijol que filtran la linfa y almacenan glóbulos blancos que ayudan a combatir infecciones y enfermedades. Los ganglios linfáticos se ubican a lo largo de una red de vasos linfáticos que recorre todo el cuerpo. Hay grupos de ganglios linfáticos en el cuello, las axilas, el mediastino (el área entre los pulmones), el abdomen, la pelvis y la ingle. El linfoma de Hodgkin se forma con mayor frecuencia en los ganglios linfáticos que están por encima del diafragma.
- Bazo: es un órgano que produce linfocitos, almacena glóbulos rojos y linfocitos, filtra la sangre y destruye las células sanguíneas viejas. El bazo se encuentra en el lado izquierdo del abdomen, cerca del estómago.
- Timo: órgano en el que los linfocitos T maduran y se multiplican. El timo está en el tórax detrás del esternón.
- Médula ósea: tejido blando y esponjoso que se encuentra en el centro de ciertos huesos, como el de la cadera y el esternón. Los glóbulos blancos, los glóbulos rojos y las plaquetas se producen en la médula ósea.
- Amígdalas: son dos pequeñas masas de tejido linfático en la parte posterior de la garganta. Hay una amígdala a cada lado de la garganta.
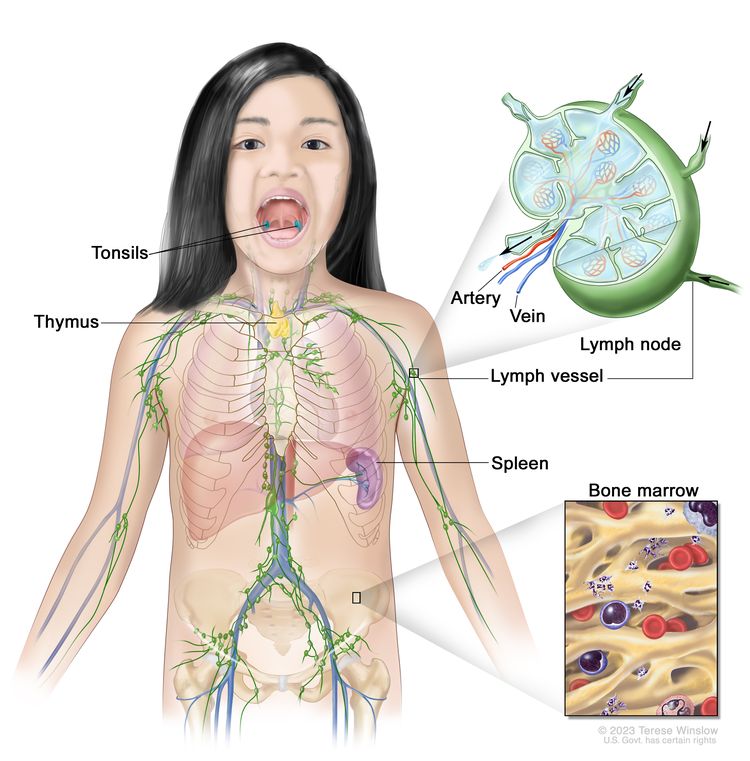
El sistema linfático forma parte del sistema inmunitario y está compuesto por tejidos y órganos que ayudan a proteger al cuerpo de infecciones y enfermedades, entre ellos, las amígdalas, el timo, el bazo, la médula ósea, los vasos linfáticos y los ganglios linfáticos. La linfa (líquido transparente y acuoso) y los linfocitos (glóbulos blancos) circulan por los vasos linfáticos hasta llegar a los ganglios linfáticos, donde destruyen las sustancias nocivas. La linfa ingresa al torrente sanguíneo a través de una vena grande cerca del corazón.
También hay fragmentos de tejido linfático en otras partes del cuerpo, como en el revestimiento del tracto gastrointestinal, los bronquios y la piel.
Existen dos tipos generales de linfoma: linfoma de Hodgkin y linfoma no Hodgkin. Este resumen trata sobre el tratamiento del linfoma de Hodgkin infantil.
El linfoma de Hodgkin se presenta con mayor frecuencia en adolescentes de 15 a 19 años. El tratamiento para niños y adolescentes es diferente al que se utiliza en adultos.
A continuación se enumeran otros resúmenes del PDQ con información relacionada con el linfoma:
Los dos tipos principales de linfoma de Hodgkin infantil son el clásico y el nodular con predominio linfocítico.
- Linfoma de Hodgkin clásico : es el tipo más común de linfoma de Hodgkin. Se presenta con mayor frecuencia en adolescentes. Se puede detectar al examinar una muestra de tejido de ganglio linfático al microscopio. Las células de El cáncer , llamadas células de Reed-Sternberg, son visibles.
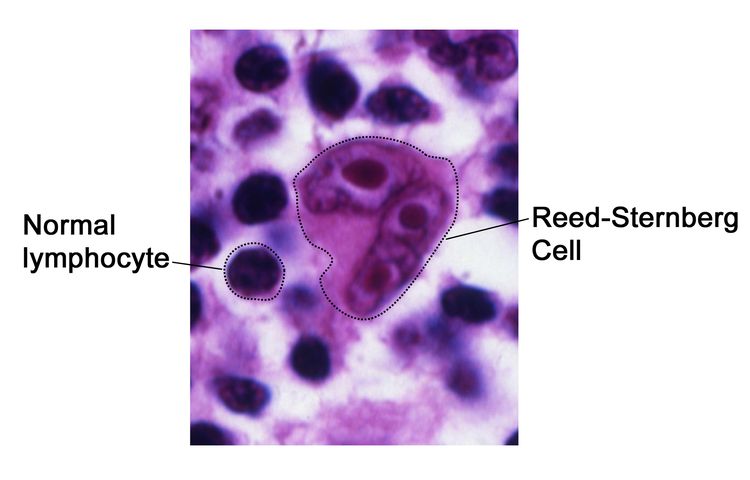
Célula de Reed-Sternberg. Las células de Reed-Sternberg son linfocitos grandes y anómalos (un tipo de glóbulo blanco) que pueden contener más de un núcleo. Estas células se hallan en personas con linfoma de Hodgkin. Las células de Reed-Sternberg también se denominan células de Hodgkin y Reed-Sternberg.
El linfoma de Hodgkin clásico se divide en cuatro subtipos, según el aspecto de las células cancerosas en el microscopio:
- El linfoma de Hodgkin esclerosante nodular se presenta con mayor frecuencia en niños mayores y adolescentes. Es común tener una masa torácica al momento del diagnóstico.
- El linfoma de Hodgkin de celularidad mixta se presenta con mayor frecuencia en niños menores de 10 años. Está relacionado con un historial de infección por el virus de Epstein-Barr (VEB) y suele desarrollarse en los ganglios linfáticos del cuello.
- El linfoma de Hodgkin con predominio linfocítico es poco frecuente en niños. Al examinar una muestra de tejido ganglionar al microscopio, se observan células de Reed-Sternberg y numerosos linfocitos normales y otras células sanguíneas.
- El linfoma de Hodgkin con depleción linfocítica es poco común en niños y se presenta con mayor frecuencia en adultos mayores y adultos con VIH. Al examinar una muestra de tejido de ganglio linfático al microscopio, se observan numerosas células cancerosas grandes y de forma irregular, y pocos linfocitos y otras células sanguíneas normales.
- El linfoma de Hodgkin con predominio linfocítico nodular es menos común que el linfoma de Hodgkin clásico. Se presenta con mayor frecuencia en niños menores de 10 años. El linfoma de Hodgkin con predominio linfocítico nodular suele presentarse como un ganglio linfático inflamado en el cuello, la axila o la ingle. La mayoría de los niños no presentan otros signos ni síntomas de cáncer al momento del diagnóstico. Al examinar una muestra de tejido de un ganglio linfático al microscopio, las células cancerosas tienen forma de palomitas de maíz.
La infección por el virus de Epstein-Barr y un historial de linfoma de Hodgkin en la familia pueden aumentar el riesgo de desarrollar linfoma de Hodgkin infantil.
Cualquier factor que aumenta la probabilidad de que una persona desarrolle una enfermedad se denomina factor de riesgo. No todas las personas con uno o más de estos factores de riesgo desarrollarán linfoma de Hodgkin infantil, y este puede desarrollarse en algunos niños sin ningún factor de riesgo conocido. Hable con el médico de su hijo o hija si cree que podría estar en riesgo.
Los factores de riesgo del linfoma de Hodgkin infantil son:
- Estar infectado con el virus de Epstein-Barr (VEB)
- Estar infectado con el VIH
- Tener ciertas enfermedades del sistema inmunitario, como el síndrome linfoproliferativo autoinmune
- Tener un sistema inmunitario debilitado después de un trasplante de órgano o por medicamentos administrados después de un trasplante para evitar que el cuerpo rechace el órgano.
- Tener un padre, madre, hermano o hermana con un historial de linfoma de Hodgkin
Los cambios hereditarios en los genes pueden aumentar el riesgo de linfoma de Hodgkin infantil.
La exposición a infecciones comunes en la primera infancia puede disminuir el riesgo de linfoma de Hodgkin en los niños.
Los signos del linfoma de Hodgkin infantil son inflamación de los ganglios linfáticos, fiebre, sudores nocturnos profusos y pérdida de peso.
Los signos y síntomas del linfoma de Hodgkin dependen de la zona del cuerpo donde se origina el cáncer y de su tamaño. Es importante consultar con el médico de su hijo o hija si presenta:
- Ganglios linfáticos inflamados e indoloros cerca de la clavícula o en el cuello, el tórax, la axila o la ingle
- Fiebre sin razón conocida
- weight loss for no known reason
- Sudores nocturnos profusos
- fatigue
- Anorexia
- Picazón en la piel
- Tos
- Dificultad para respirar, especialmente al acostarse
- Dolor en los ganglios linfáticos después de beber alcohol
La fiebre o pérdida de peso sin razón conocida y los sudores nocturnos intensos se denominan síntomas B. Los síntomas B son una parte importante de la estadificación del linfoma de Hodgkin y de la comprensión de las posibilidades de recuperación del paciente.
Estos síntomas pueden deberse a problemas distintos al linfoma de Hodgkin infantil. La única manera de saberlo es consultar al médico de su hijo o hija. El médico le preguntará cuándo comenzaron los síntomas y con qué frecuencia los ha presentado como primer paso para establecer un diagnóstico.
Para diagnosticar y estadificar el linfoma de Hodgkin infantil se utilizan pruebas que examinan el sistema linfático y otras partes del cuerpo.
Si su hijo o hija presenta síntomas que sugieren la presencia de linfoma de Hodgkin, el médico deberá determinar si se deben a cáncer o a otro problema. Le preguntará sobre su historial de salud personal y familiar y le realizará un reconocimiento físico. El médico podría recomendar pruebas diagnósticas para determinar si su hijo o hija tiene linfoma de Hodgkin. Los resultados de estas pruebas también les ayudarán a usted y al médico a planificar el tratamiento.
Las pruebas utilizadas para diagnosticar el linfoma de Hodgkin pueden ser:
- Biometría hemática: es un procedimiento en el que se extrae una muestra de sangre y se analiza para determinar:
- La cantidad de glóbulos rojos, glóbulos blancos y plaquetas
- La cantidad de hemoglobina (la proteína que transporta el oxígeno) en los glóbulos rojos.
- La parte de la muestra de sangre compuesta por glóbulos rojos.
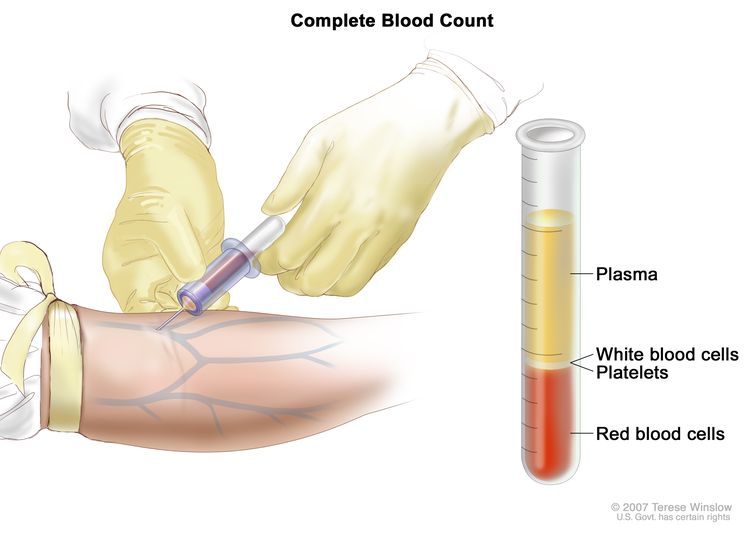
Hemograma completo (HC): la sangre se extrae insertando una aguja en una vena y dejando que fluya hacia un tubo. La muestra se envía al laboratorio y se cuentan los glóbulos rojos, los glóbulos blancos y las plaquetas. El HC se utiliza para detectar, diagnosticar y controlar diversas afecciones.
- Estudios de química sanguínea: es un procedimiento en el que se analiza una muestra de sangre para medir la cantidad de ciertas sustancias, como la albúmina, que los órganos y tejidos del cuerpo liberan en la sangre. Una cantidad inusual (superior o inferior a lo normal) de una sustancia puede ser un signo de enfermedad.
- Prueba de proteína C reactiva: es una prueba en la que se analiza una muestra de sangre para medir la cantidad de proteína C reactiva en la sangre. La proteína C reactiva es producida por el hígado y se envía al torrente sanguíneo en respuesta a la inflamación. Un nivel de proteína C reactiva en sangre superior a la normal puede ser un signo de enfermedad.
- Velocidad de sedimentación globular (VSG): es un procedimiento en el que se extrae una muestra de sangre y se analiza la velocidad con la que los glóbulos rojos se depositan en el fondo del tubo de ensayo. La VSG mide el grado de inflamación en el cuerpo. Un nivel de VSG superior a lo normal puede ser un signo de linfoma. También se denomina velocidad de sedimentación o tasa de sedimentación.
- Tomografía computarizada (TC): es un procedimiento que crea una serie de imágenes detalladas de áreas internas del cuerpo, como el cuello, el tórax, el abdomen o la pelvis, tomadas desde diferentes ángulos. Las imágenes se crean mediante una computadora conectada a una máquina de rayos X. Un dye may be inyecta por vía intravenosa o ingerirse para que los órganos o tejidos se visualicen con mayor claridad. Este procedimiento también se denomina tomografía axial computarizada. Puede obtener más información en Tomografía computarizada para el cáncer.
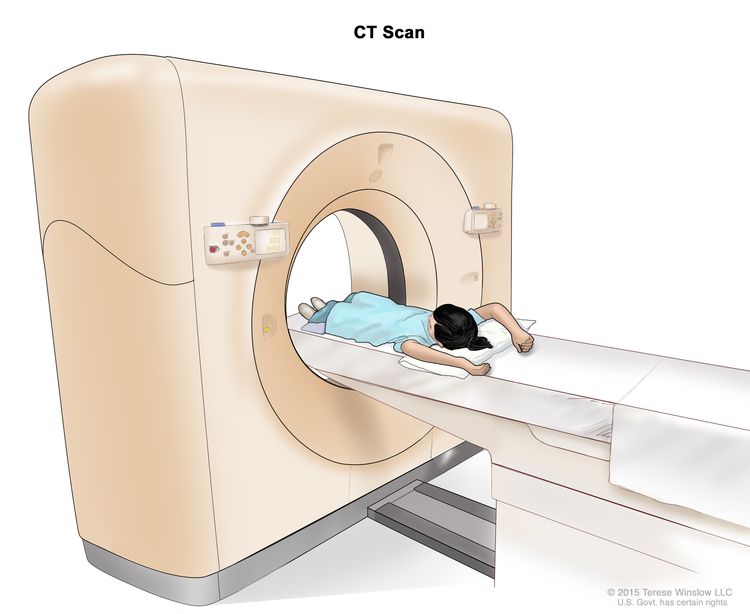
Tomografía computarizada (TC): el niño se recuesta sobre una camilla que se desliza a través del escáner, el cual toma una serie de radiografías detalladas de zonas internas del cuerpo.
- Tomografía por emisión de positrones (PET): procedimiento que se utiliza para detectar células tumorales malignas en el cuerpo. Se inyecta una pequeña cantidad de glucosa radiactiva (azúcar) en una vena. El escáner escáner gira alrededor del cuerpo y captura imágenes de las zonas donde se utiliza la glucosa. Las células tumorales malignas se ven más brillantes en la imagen porque son más activas y absorben más glucosa que las células normales.
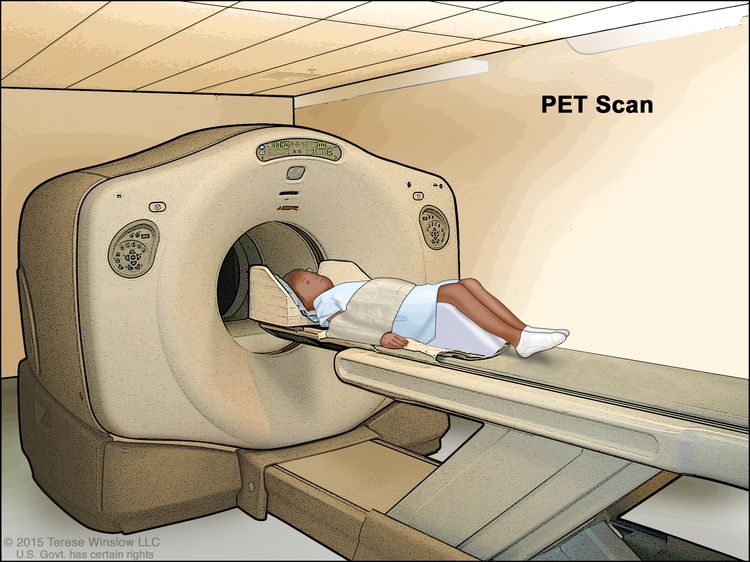
Tomografía por emisión de positrones (PET, por sus siglas en inglés): el niño se recuesta sobre una camilla que se desliza a través del escáner PET. El reposacabezas y la correa blanca ayudan al niño a permanecer inmóvil. Se inyecta una pequeña cantidad de glucosa radiactiva (azúcar) en la vena del niño y el escáner genera una imagen de las zonas del cuerpo donde se utiliza la glucosa. Las células cancerosas se ven más brillantes en la imagen porque absorben más glucosa que las células normales.
- Resonancia magnética (RM): procedimiento que utiliza un imán, ondas de radio, así como una computadora para generar una serie de imágenes detalladas de áreas internas del cuerpo, como los ganglios linfáticos. Este procedimiento también se denomina resonancia magnética nuclear (RMN).
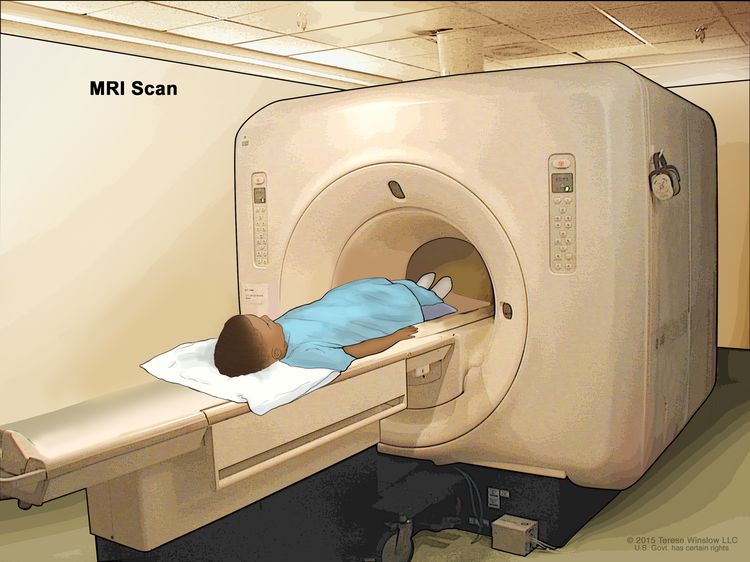
Resonancia magnética (RM): el niño se recuesta en una camilla que se desliza a través del equipo de resonancia magnética, que toma una serie de imágenes detalladas del interior del cuerpo. La posición del niño en la camilla depende de la parte del cuerpo que se va a examinar.
- Exploración PET-TC: es un procedimiento que combina las imágenes de una tomografía por emisión de positrones (PET) y una tomografía computarizada (TC). Ambos procedimientos se realizan de forma simultánea con el mismo equipo. La combinación de ambas exploraciones permite obtener imágenes más detalladas de las áreas internas del cuerpo que las que ofrece cada una por separado.
- Tomografía por emisión de positrones combinada con resonancia magnética (PET-RM): Un procedimiento que combina las imágenes de una tomografía por emisión de positrones (PET) y una resonancia magnética (RM). Una PET utiliza un trazador radiactivo para resaltar áreas anormales en el cuerpo. Una RM utiliza ondas de radio y un potente imán para obtener imágenes detalladas de los tejidos corporales. En una PET-RM, ambas exploraciones se realizan simultáneamente con el mismo equipo. Las exploraciones combinadas proporcionan imágenes más detalladas de las áreas internas del cuerpo que cualquiera de las exploraciones por separado. Además, se reduce la cantidad total de radiación a la que se expone una persona. Una PET-RM puede utilizarse para ayudar a diagnosticar enfermedades, como el cáncer, planificar tratamientos o evaluar su eficacia.
- Radiografía de tórax: es una radiografía de los órganos y huesos del interior del tórax. Un rayo X es un tipo de haz de energía que puede atravesar el cuerpo y plasmarse en una película, generando una imagen de áreas internas del cuerpo.
- Aspiración y biopsia de médula ósea: extracción de la médula ósea y un pequeño fragmento de hueso insertando una aguja hueca en el hueso de la cadera o el esternón. Un patólogo observa la médula ósea y el hueso bajo un microscopio para detectar células anómalas . La aspiración y biopsia de médula ósea se realiza en pacientes con enfermedad avanzada y/o síntomas B.
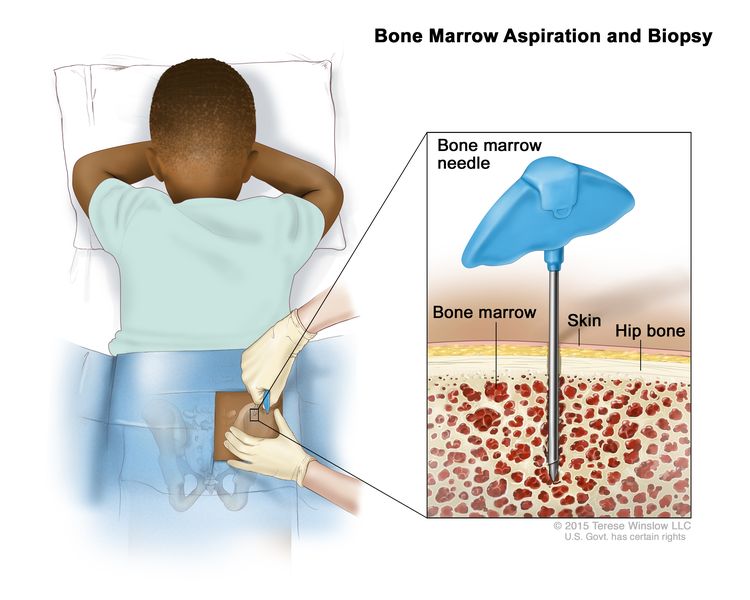
Aspiración y biopsia de médula ósea: tras anestesiar una pequeña zona de la piel, se introduce una aguja para médula ósea en el hueso de la cadera del niño. Se extraen muestras de sangre, hueso y médula ósea para examinarlas con un microscopio.
- Biopsia de ganglio linfático: es la extirpación total o parcial de uno o más ganglios linfáticos. El ganglio linfático puede extirparse mediante una tomografía computarizada guiada por imágenes o una toracoscopia, mediastinoscopiao laparoscopia. Se puede realizar uno de los siguientes tipos de biopsias:
- Biopsia por escisión: es la extirpación de un ganglio linfático completo.
- Biopsia incisional: es la extirpación de parte de un ganglio linfático.
- Biopsia central: consiste en la extracción de tejido de un ganglio linfático mediante una aguja gruesa.
Un patólogo examina el tejido del ganglio linfático con un microscopio para detectar células cancerosas llamadas células de Reed-Sternberg. Estas células son comunes en el linfoma de Hodgkin clásico.
Se puede realizar la siguiente prueba en el tejido que se extrajo:
- Inmunofenotipificación: es una prueba de laboratorio que utiliza anticuerpos para identificar células cancerosas según los tipos de antígenos o marcadores presentes en la superficie. Esta prueba se utiliza para diagnosticar tipos específicos de linfoma.
Es posible que desee obtener una segunda opinión.
Quizá desee obtener una segunda opinión para confirmar el diagnóstico y el plan de tratamiento de su hijo o hija. Si busca una segunda opinión, necesitará obtener los resultados de las pruebas médicas que realizó el primer médico para compartirlos con el segundo, que revisará el informe patológico, las diapositivas y las exploraciones antes de emitir una recomendación. Podría coincidir con el primer médico, sugerir cambios u otro enfoque u ofrecerle más información sobre el cáncer de su hijo.
Para obtener más información sobre cómo elegir un médico y obtener una segunda opinión, visite la sección Cómo encontrar atención médica para el cáncer. Puede comunicarse con el Servicio de Información sobre el Cáncer del NCI por chat, correo electrónico o teléfono (en inglés y español) para obtener ayuda para encontrar un médico u hospital que pueda ofrecerle una segunda opinión. Si tiene alguna pregunta durante sus citas, visite Preguntas para su médico sobre el cáncer.
Certain factors affect prognosis (chance of recovery) and treatment options.
Si a su hijo o hija le han diagnosticado linfoma de Hodgkin, es posible que tenga preguntas sobre la gravedad del cáncer y sus posibilidades de supervivencia. El pronóstico es el probable desenlace o evolución de una enfermedad. El pronóstico depende de:
- El estadio del cáncer (el tamaño del cáncer, incluso si se trata de una masa tumoral más grande llamada enfermedad voluminosa, y si el cáncer se ha propagado por debajo del diafragma o a más de un grupo de ganglios linfáticos).
- Si hay síntomas B (fiebre o pérdida de peso sin causa conocida o sudores nocturnos profusos) en el momento del diagnóstico.
- El tipo de linfoma de Hodgkin
- Tener un nivel de glóbulos blancos mayor a la habitual o anemia al momento del diagnóstico
- Si hay líquido alrededor del corazón o los pulmones en el momento del diagnóstico.
- La velocidad de sedimentación o el nivel de albúmina en sangre
- El sexo del niño
- Si el cáncer ha sido diagnosticado recientemente o ha recidivado (regresado).
Las opciones de tratamiento también dependen de:
- Si existe un riesgo bajo, medio o alto de que el cáncer regrese después del tratamiento.
- La edad del niño
- El riesgo de desarrollar efectos secundarios a largo plazo
La mayoría de los niños y adolescentes con linfoma de Hodgkin de diagnóstico reciente pueden curarse.
El equipo de atención médica del cáncer de su hijo o hija es el que está en la mejor posición para hablar con usted sobre su pronóstico.
Etapas del linfoma de Hodgkin infantil
Puntos clave
- Una vez diagnosticado el linfoma de Hodgkin infantil, se realizan pruebas para determinar si las células cancerosas se han propagado dentro del sistema linfático o a otras partes del cuerpo.
- There are three ways that cancer spreads in the body.
- El linfoma de Hodgkin infantil se puede estadificar de la siguiente manera:
- Estadio I
- Estadio II
- Estadio III
- Estadio IV
- Además del número de estadio, pueden indicarse las letras A, B, E o S.
- El linfoma de Hodgkin infantil se trata según los grupos de riesgo.
- A veces, el linfoma de Hodgkin infantil no responde al tratamiento o regresa después de este.
Una vez diagnosticado el linfoma de Hodgkin infantil, se realizan pruebas para determinar si las células cancerosas se han propagado dentro del sistema linfático o a otras partes del cuerpo.
El proceso para determinar si el cáncer se ha propagado se denomina estadificación. La información obtenida durante la estadificación determina el estadio de la enfermedad. Los resultados de las pruebas y procedimientos realizados para diagnosticar y estadificar el linfoma de Hodgkin se utilizan para tomar decisiones sobre el tratamiento.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
El linfoma de Hodgkin infantil se puede estadificar de la siguiente manera:
Estadio I
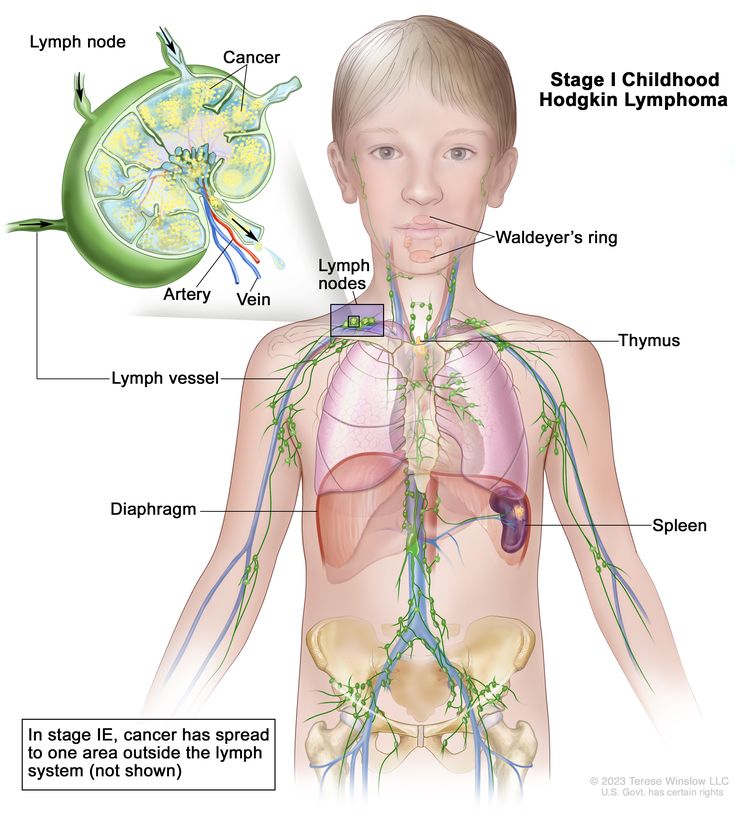
Linfoma de Hodgkin infantil en estadio I: el cáncer se encuentra en uno o más ganglios linfáticos de un grupo ganglionar o, en casos raros, en el anillo de Waldeyer, el timo o el bazo. En el estadio IE (no se muestra en el gráfico), el cáncer se ha propagado a una zona fuera del sistema linfático.
El estadio I se divide en I y IE.
- Estadio I: el cáncer se encuentra en uno de los siguientes lugares del sistema linfático:
- Uno o más ganglios linfáticos en un grupo ganglionar
- El anillo de Waldeyer.
- Timo.
- Spleen.
- Estadio IE: el cáncer se encuentra fuera del sistema linfático, en un solo órgano o área.
Estadio II
El estadio II se divide en II y IIE.
- Estadio II: el cáncer se encuentra en dos o más grupos de ganglios linfáticos por encima o por debajo del diafragma (el músculo delgado debajo del pulmones que facilita la respiración y separa el tórax del abdomen).
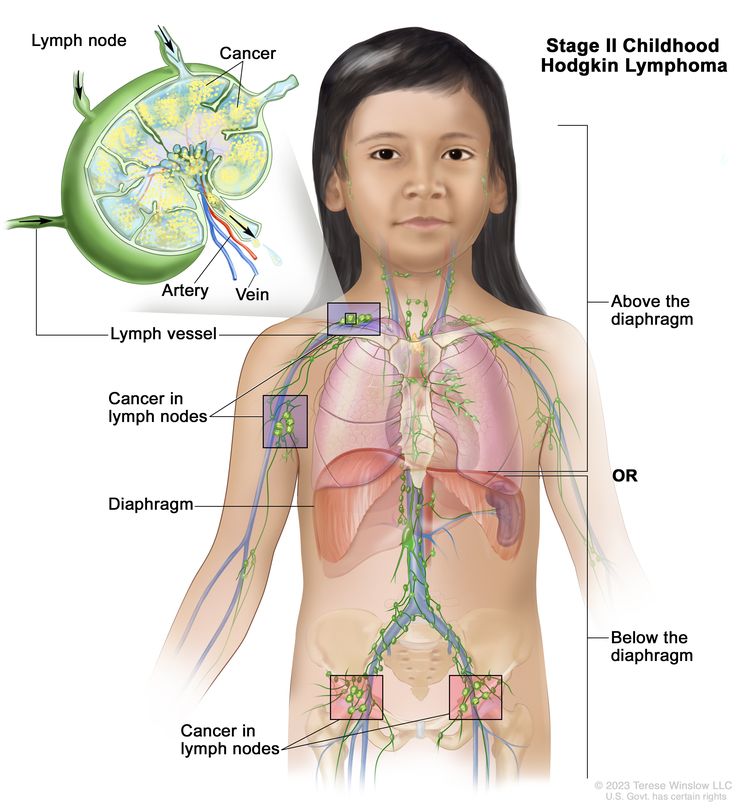
Linfoma de Hodgkin infantil en estadio II: hay cáncer en dos o más grupos de ganglios linfáticos ubicados por encima o por debajo del diafragma.
- Estadio IIE: el cáncer se ha propagado desde un grupo de ganglios linfáticos a un órgano cercano que está fuera del sistema linfático. Es posible que el cáncer se haya propagado a otros grupos de ganglios linfáticos del mismo lado del diafragma.
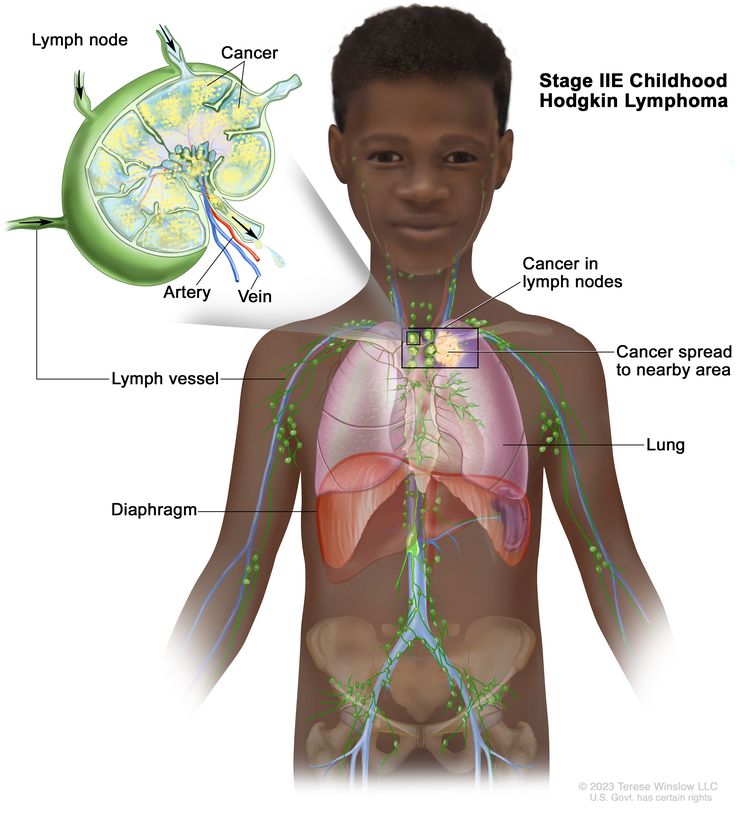
Linfoma de Hodgkin infantil en estadio IIE: el cáncer se ha propagado desde un grupo de ganglios linfáticos a un órgano o área cercana fuera del sistema linfático.
Estadio III
En el estadio III, el cáncer está en alguno de los siguientes lugares:
- En los grupos de ganglios linfáticos encima y debajo del diafragma (el músculo delgado debajo de los pulmones que facilita la respiración y separa el tórax del abdomen).
- En grupos de ganglios linfáticos por encima del diafragma y en el bazo.
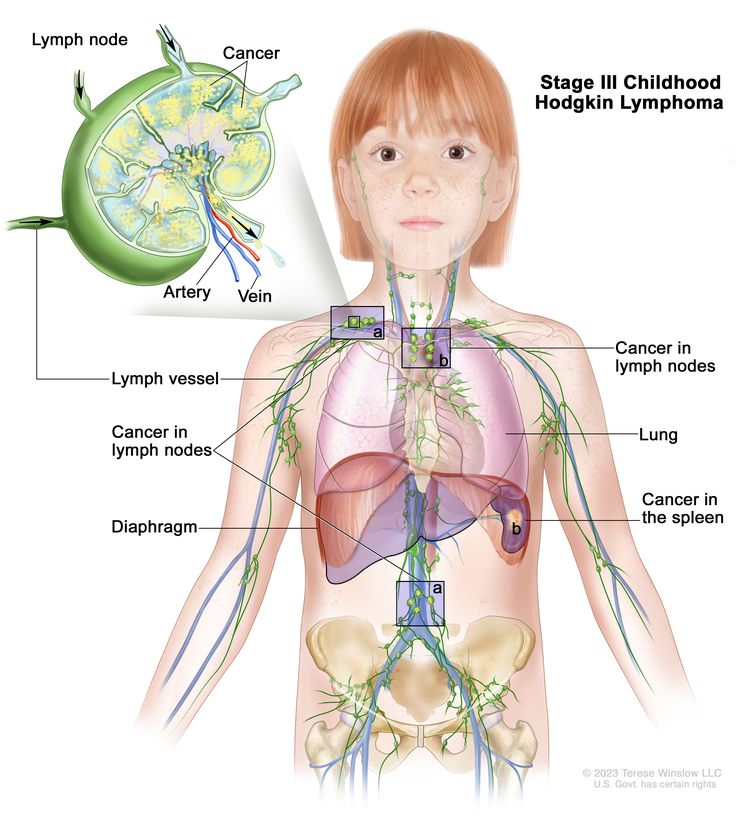
Linfoma de Hodgkin infantil en estadio III: el cáncer se encuentra (a) en los grupos de ganglios linfáticos por encima y por debajo del diafragma, o (b) en grupos de ganglios linfáticos encima del diafragma y en el bazo.
Estadio IV
En el estadio IV, se presenta alguna de estas situaciones:
- Se ha diseminado por uno o más órganos fuera del sistema linfático y puede estar presente en los ganglios linfáticos cercanos a esos órganos.
- El cáncer se encuentra en dos o más grupos de ganglios linfáticos que están en el mismo lado del diafragma (el músculo delgado debajo de los pulmones que facilita la respiración y separa el tórax del abdomen) y en un órgano que está fuera del sistema linfático y lejos de los ganglios linfáticos afectados.
- Se encuentra en grupos de ganglios linfáticos a ambos lados del diafragma y en cualquier órgano que se encuentre fuera del sistema linfático.
- Se ha extendido a los pulmones, hígadoo médula ósea desde áreas del cuerpo muy lejanas.
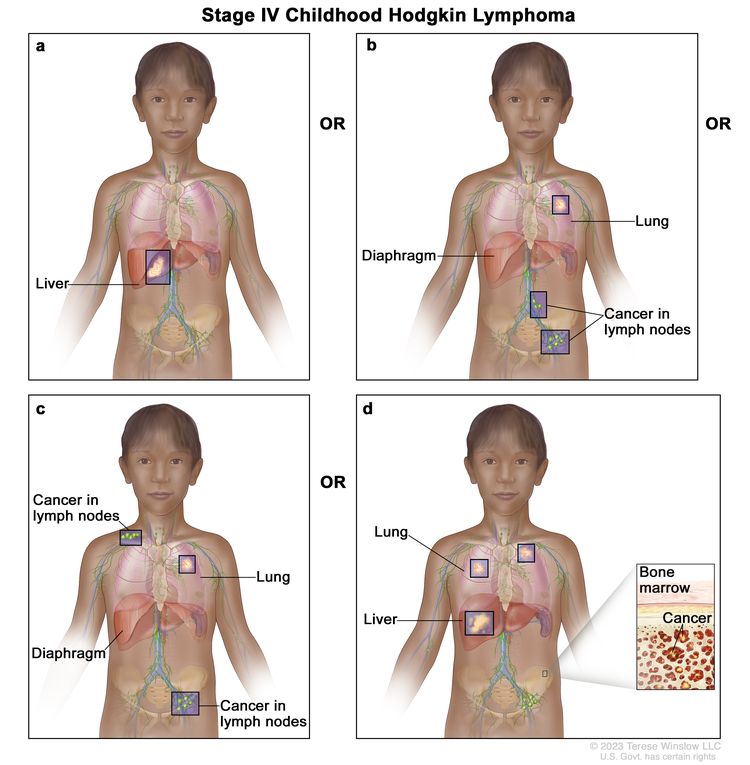
Linfoma de Hodgkin infantil en estadio IV. El cáncer (a) se ha diseminado a uno o más órganos fuera del sistema linfático, como el hígado; (b) se encuentra en dos o más grupos de ganglios linfáticos que están en el mismo lado del diafragma y en un órgano que está fuera del sistema linfático, como el pulmón, y no cerca de los ganglios linfáticos afectados; (c) se encuentra en grupos de ganglios linfáticos a ambos lados del diafragma y en cualquier órgano que esté fuera del sistema linfático, como el pulmón; o (d) se ha propagado a los pulmones, el hígado o la médula ósea desde áreas lejanas.
Además del número de estadio, pueden indicarse las letras A, B, E o S.
Las letras A, B, E o S se pueden utilizar para describir con más precisión el estadio del linfoma de Hodgkin infantil.
- A: el paciente no presenta síntomas B (fiebre, pérdida de peso o sudores nocturnos profusos).
- B: el paciente tiene síntomas B.
- E: el cáncer se encuentra en un órgano o tejido que no forma parte del sistema linfático, pero que puede estar junto a una zona del sistema linfático afectada por el cáncer.
- S: el cáncer se encuentra en el bazo.
El linfoma de Hodgkin infantil se trata según los grupos de riesgo.
El linfoma de Hodgkin infantil no tratado se divide en grupos de riesgo según el estadio, el tamaño del tumor y si el paciente presenta síntomas B (fiebre, pérdida de peso o sudores nocturnos profusos). El grupo de riesgo describe la probabilidad de que el linfoma de Hodgkin no responda al tratamiento o recidive (regrese) después del mismo. Se utiliza para planificar el tratamiento inicial.
- Linfoma de Hodgkin infantil de bajo riesgo.
- Linfoma de Hodgkin infantil de riesgo intermedio.
- Linfoma de Hodgkin infantil de alto riesgo.
El linfoma de Hodgkin de bajo riesgo requiere menos ciclos de tratamiento, una cantidad menor de medicamentos para el cáncer y dosis más bajas de los mismos que el linfoma de alto riesgo.
A veces, el linfoma de Hodgkin infantil no responde al tratamiento o regresa después de este.
El linfoma de Hodgkin primario refractario es un cáncer que no responde al tratamiento inicial.
El linfoma de Hodgkin recidivante es un cáncer que ha recidivado (regresado) después de haber sido tratado. El linfoma puede reaparecer en el sistema linfático o en otras partes del cuerpo, como los pulmones, el hígado, los huesos o la médula ósea.
Treatment Option Overview
Puntos clave
- Existen diferentes tipos de tratamiento para los niños con linfoma de Hodgkin.
- El tratamiento de los niños con linfoma de Hodgkin debe ser planificado por un equipo de proveedores de atención médica especializados en el tratamiento del cáncer infantil.
- Pueden emplearse los siguientes tipos de tratamiento:
- Quimioterapia
- Radioterapia
- Terapia dirigida
- Inmunoterapia
- Cirugía
- Quimioterapia de dosis alta con trasplante de células madre
- Ensayos clínicos
- Radioterapia con haz de protones
- El tratamiento del linfoma de Hodgkin infantil produce efectos secundarios y efectos tardíos.
- Patients may want to think about taking part in a clinical trial.
- Patients can enter clinical trials before, during, or after starting their cancer treatment.
- Es posible que se necesiten cuidados de seguimiento.
Existen diferentes tipos de tratamiento para los niños con linfoma de Hodgkin.
Existen diferentes tipos de tratamiento para niños con linfoma de Hodgkin. Usted y el equipo médico de su hijo trabajarán juntos para decidir el tratamiento. Se tendrán en cuenta muchos factores, como la salud general de su hijo y si el tumor es de reciente diagnóstico o ha reaparecido.
El tratamiento de los niños con linfoma de Hodgkin debe ser planificado por un equipo de proveedores de atención médica especializados en el tratamiento del cáncer infantil.
Un oncólogo pediátrico, médico especializado en el tratamiento de niños con cáncer, supervisa el tratamiento del linfoma de Hodgkin infantil. El oncólogo pediátrico colabora con otros profesionales de la salud pediátrica expertos en el tratamiento de niños con linfoma de Hodgkin y que se especializan en ciertas áreas de la medicina. Otros especialistas pueden ser:
- Pediatra
- Médico oncólogo y hematólogo
- Oncólogo radioterapeuta
- pathologist
- Especialista en enfermería pediátrica
- Psicólogo
- Trabajador social
- Especialista en desarrollo infantil
- Especialista en fertilidad
Es posible que el tratamiento del linfoma de Hodgkin en adolescentes y adultos jóvenes sea diferente al de los niños. Algunos adolescentes y adultos jóvenes reciben un régimen de tratamiento para adultos.
Pueden emplearse los siguientes tipos de tratamiento:
Quimioterapia
La quimioterapia es un tratamiento contra el cáncer que utiliza uno o más fármacos para detener el crecimiento de las células cancerosas, ya sea destruyéndolas o impidiendo su división. El tratamiento contra el cáncer que utiliza más de un fármaco de quimioterapia se denomina quimioterapia combinada . Cuando la quimioterapia se administra por vía oral o se inyecta en una vena o músculo, los fármacos entran en el torrente sanguíneo y pueden llegar a las células cancerosas en todo el cuerpo ( quimioterapia sistémica ).
La forma de administrar la quimioterapia depende del grupo de riesgo. Por ejemplo, los niños con linfoma de Hodgkin de bajo riesgo reciben menos ciclos de tratamiento, una menor cantidad de medicamentos dosis más bajas de estos que los niños con linfoma de alto riesgo.
Para obtener más información, visite Medicamentos aprobados para el linfoma de Hodgkin.
Radioterapia
La radioterapia es un tratamiento contra el cáncer que utiliza rayos X de alta energía u otros tipos de radiación para matar las células cancerosas o evitar que crezcan. Para la radioterapia externa se usa una máquina que envía la radiación hacia la zona con cáncer desde el exterior del cuerpo.
Ciertas formas de administrar radioterapia pueden ayudar a evitar que la radiación dañe el tejido sano cercano. Estos tipos de radioterapia externa incluyen:
- La radioterapia conformacional es un tipo de radioterapia externa que utiliza una computadora para crear una imagen tridimensional (3D) del tumor y adapta los haces de radiación para que se ajusten a la forma del tumor.
- La radioterapia de intensidad modulada (TRIM) es un tipo de radioterapia tridimensional (3D) que utiliza una computadora para generar imágenes del tamaño y la forma del tumor. Se dirigen haces delgados de radiación de diferentes intensidades al tumor desde distintos ángulos.
La radioterapia puede administrarse según el grupo de riesgo del niño y el régimen de quimioterapia. La radiación se aplica únicamente a los ganglios linfáticos u otras áreas afectadas por el cáncer.
Terapia dirigida
La terapia dirigida es un tipo de tratamiento que utiliza medicamentos u otras sustancias para identificar y atacar células cancerosas específicas. Los tipos de terapia dirigida son:
- Anticuerpo monoclonal terapia: Monoclonal anticuerpos monoclonales son sistema inmunitario proteínas producidas en el laboratorio para tratar muchas enfermedades, entre ellas el cáncer. Como tratamiento contra el cáncer, estos anticuerpos pueden unirse a un objetivo específico en las células cancerosas u otras células que pueden ayudar a que las células cancerosas crezcan. Los anticuerpos se administran mediante infusión. Pueden usarse solos o para transportar drogas, toxinas o radioactivo material directamente a las células cancerosas.
Se pueden usar rituximab o brentuximab para tratar el linfoma de Hodgkin infantil de alto riesgo, refractario o recidivante.
- Terapia con inhibidores del proteasoma : bloquea la acción de los proteasomas en las células cancerosas. Los proteasomas eliminan las proteínas que la célula ya no necesita. Cuando los proteasomas se bloquean, esas proteínas se acumulan en la célula, lo que puede provocar la muerte de la célula cancerosa.
Bortezomib es un inhibidor del proteasoma que se utiliza para tratar el linfoma de Hodgkin infantil refractario o recurrente.
Obtenga más información en Terapia dirigida para tratar el cáncer.
Inmunoterapia
La inmunoterapia utiliza el sistema inmunitario del paciente para combatir el cáncer. Se utilizan sustancias producidas por el cuerpo o en un laboratorio para reforzar, dirigir o restaurar las defensas naturales del cuerpo contra el cáncer. Los tipos de inmunoterapia son:
- Immune checkpoint inhibitor algunos tipos de immune cells, such as células T, y algunas células cancerosas tienen ciertas proteínas, llamadas proteínas de punto de control, en su superficie, las cuales mantienen las respuestas inmunes bajo control. Cuando las células cancerosas tienen grandes cantidades de estas proteínas, no serán atacadas ni destruidas por los linfocitos T. Los inhibidores de puestos de control inmunitario bloquean estas proteínas, lo que aumenta la capacidad de los linfocitos T para destruir las células cancerosas. A continuación, se describe un tipo de terapia con inhibidores de puestos de control inmunitario:
- Terapia con inhibidores de PD-1 and PD-L1 terapia con inhibidores: PD-1 es una proteína en la superficie de las células T que ayuda a mantener el cuerpo en funcionamiento. respuestas inmunes bajo control. La PD-L1 es una proteína presente en algunos tipos de células cancerosas. Cuando la PD-1 se une a la PD-L1, impide que el linfocito T destruya la célula cancerosa. Los inhibidores de PD-1 y PD-L1 impiden que las proteínas PD-1 y PD-L1 se unan entre sí, lo que permite que los linfocitos T destruyan las células cancerosas.
Pembrolizumab y nivolumab son tipos de inhibidores de PD-1 que pueden usarse en el tratamiento del linfoma de Hodgkin infantil que ha regresado después del tratamiento.
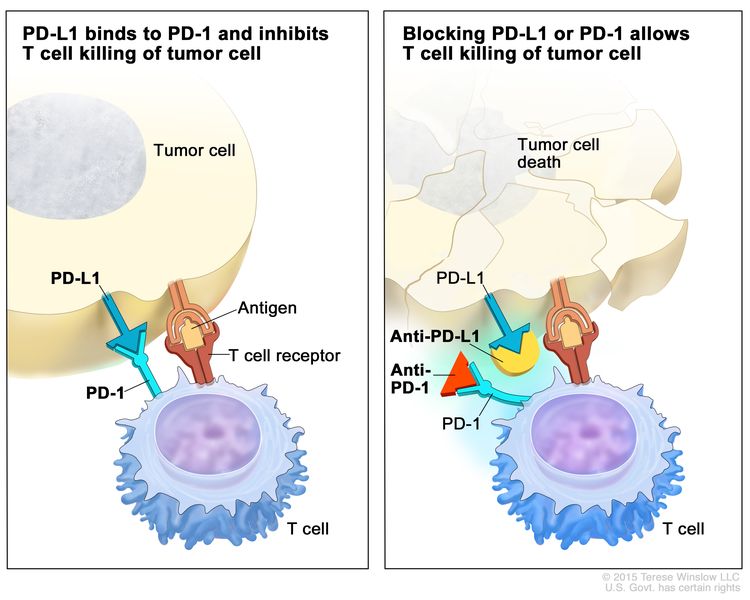
Inhibidor de puestos de control inmunitario. Las proteínas de puestos de control, como PD-L1 en las células tumorales y PD-1 en las células T, regulan las respuestas inmunitarias. La unión de PD-L1 y PD-1 evita que las células T destruyan las células tumorales en el cuerpo (panel izquierdo). El bloqueo de esta unión con un inhibidor del puesto de control inmunitario (anti-PD-L1 o anti-PD-1) permite que las células T eliminen las células tumorales (panel derecho).
- Terapia con inhibidores de PD-1 and PD-L1 terapia con inhibidores: PD-1 es una proteína en la superficie de las células T que ayuda a mantener el cuerpo en funcionamiento. respuestas inmunes bajo control. La PD-L1 es una proteína presente en algunos tipos de células cancerosas. Cuando la PD-1 se une a la PD-L1, impide que el linfocito T destruya la célula cancerosa. Los inhibidores de PD-1 y PD-L1 impiden que las proteínas PD-1 y PD-L1 se unan entre sí, lo que permite que los linfocitos T destruyan las células cancerosas.
Cirugía
En niños con linfoma de Hodgkin nodular localizado con predominio de linfocitos, se puede recurrir a la cirugía para extirpar la mayor parte posible del tumor.
Quimioterapia de dosis alta con trasplante de células madre
Se administran altas dosis de quimioterapia para destruir las células cancerosas. El tratamiento para el cáncer también destruye las células sanas, incluidas las hematopoyéticas. El trasplante de células madre es un tratamiento para reemplazar las hematopoyéticas. Las células madre (células sanguíneas inmaduras) se extraen de la sangre o de la médula ósea del paciente o de un donante, se congelan y se almacenan. Una vez que el paciente finaliza la quimioterapia, las células madre almacenadas se descongelan y se administran al paciente mediante una infusión. Estas células madre reinfundidas se convierten en (y restauran) las células sanguíneas del cuerpo.
Para obtener más información, visite Medicamentos aprobados para el linfoma de Hodgkin.
Ensayos clínicos
Un ensayo clínico de tratamiento es un estudio de investigación diseñado para mejorar los tratamientos actuales o explorar nuevas opciones para pacientes con cáncer. Dado que el cáncer infantil es una enfermedad rara, se debe considerar participar en un ensayo clínico.
Utilice nuestra herramienta de búsqueda de ensayos clínicos para encontrar ensayos clínicos sobre el cáncer respaldados por el NCI que admitan pacientes. Puede buscar ensayos según el tipo de cáncer, la edad del paciente y el lugar donde se realizan. Algunos ensayos clínicos solo están abiertos a pacientes que no han comenzado el tratamiento. Los ensayos clínicos respaldados por otras organizaciones se pueden encontrar en el sitio web ClinicalTrials.gov.
Para obtener más información, consulte la sección Información sobre ensayos clínicos para pacientes y cuidadores .
Radioterapia con haz de protones
La radioterapia con haz de protones es un tipo de radioterapia externa de alta energía que utiliza haces de protones (partículas pequeñas de materia con carga positiva) para generar radiación. Este tipo de radioterapia puede ayudar a reducir el daño al tejido sano cercano al tumor, como la mama, el corazón y los pulmones .
El tratamiento del linfoma de Hodgkin infantil produce efectos secundarios y efectos tardíos.
Para obtener más información sobre los efectos secundarios que aparecen durante el tratamiento del cáncer, consulte la sección Efectos secundarios.
Los efectos secundarios del tratamiento del cáncer que comienzan después del tratamiento y persisten durante meses o años se denominan efectos tardíos. Dado que estos efectos afectan la salud y el desarrollo, es importante realizar exámenes de seguimiento de forma periódica.
Los efectos tardíos del tratamiento contra el cáncer pueden incluir:
- Problemas físicos que afectan a:
- El desarrollo de los órganos sexuales y reproductivos
- La fertilidad (capacidad de tener hijos)
- El crecimiento y desarrollo de huesos y músculos
- La función tiroidea, cardiaca o pulmonar
- La función de los dientes, las encías y las glándulas salivales
- La función del bazo (mayor riesgo de infección)
- Cambios en el estado de ánimo, los sentimientos, los pensamientos, el aprendizaje o la memoria
- Cánceres secundarios (nuevos tipos de cáncer), como el de mama, de tiroides, de piel, de pulmón, de estómago o colorrectal
Las mujeres que sobreviven al linfoma de Hodgkin tienen un mayor riesgo de desarrollar cáncer de mama. Este riesgo depende de la cantidad de radiación recibida en la mama durante el tratamiento y del régimen de quimioterapia utilizado. El riesgo disminuye si también se administró radiación a los ovarios.
Los médicos pueden recomendar que las supervivientes que recibieron radioterapia mamaria se realicen una mamografía y una resonancia magnética una vez al año a partir de los ocho años después del tratamiento o a los 25 años, lo que ocurra más tarde. También pueden sugerir que se realicen un autoexamen de mama mensualmente a partir de la pubertad y un examen de mama realizado por un profesional de la salud anualmente desde la pubertad hasta los 25 años. Luego, este último debería hacerse cada seis meses a partir de los 25 años.
Los hombres sobrevivientes que recibieron radioterapia torácica podrían tener un mayor riesgo de desarrollar una enfermedad cardiovascular. Se recomienda limitar la radioterapia torácica, si es posible.
El dexrazoxano es un medicamento que puede reducir el riesgo de daño cardiaco a largo plazo en los supervivientes de linfoma de Hodgkin. Generalmente, se administra junto con la quimioterapia y otros tratamientos.
Algunos efectos tardíos pueden tratarse o controlarse. Es importante hablar con los médicos de su hijo sobre los posibles efectos tardíos causados por algunos tratamientos. Obtenga más información sobre los efectos tardíos del tratamiento del cáncer infantil .
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Es posible que se necesiten cuidados de seguimiento.
Durante el tratamiento, su hijo/a se someterá a pruebas o revisiones de seguimiento. Algunas pruebas realizadas para diagnosticar o estadificar el cáncer podrían repetirse para evaluar la eficacia del tratamiento. Las decisiones sobre si continuar, modificar o suspender el tratamiento podrían basarse en los resultados de estas pruebas.
Algunas de las pruebas se seguirán realizando periódicamente después de que finalice el tratamiento. Los resultados de estas pruebas pueden mostrar si la afección de su hijo o hija ha cambiado o si el cáncer ha recidivado (regresado).
En el caso de los pacientes que reciben solo quimioterapia, se puede realizar una tomografía por emisión de positrones (PET) tres semanas o más después de finalizar el tratamiento. En el caso de los pacientes que reciben radioterapia al final de su tratatamiento, no se les debe realizar una tomografía PET hasta 8 a 12 semanas después de finalizar el tratamiento.
Tratamiento del linfoma de Hodgkin clásico infantil de bajo riesgo
For information about the treatments listed below, visit the Treatment Option Overview section.
El tratamiento del linfoma de Hodgkin clásico de bajo riesgo recién diagnosticado en niños puede incluir:
- Quimioterapia combinada.
- También se puede administrar radioterapia en las zonas donde está el cáncer.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del linfoma de Hodgkin clásico infantil de riesgo intermedio
For information about the treatments listed below, visit the Treatment Option Overview section.
El tratamiento del linfoma de Hodgkin clásico de riesgo intermedio recién diagnosticado en niños puede incluir:
- Quimioterapia combinada.
- También se puede administrar radioterapia en las zonas donde está el cáncer.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del linfoma de Hodgkin clásico infantil de alto riesgo
For information about the treatments listed below, visit the Treatment Option Overview section.
El tratamiento del linfoma de Hodgkin clásico de alto riesgo recién diagnosticado en niños puede incluir:
- Quimioterapia combinada en dosis más alta
- Quimioterapia combinada con terapia dirigida (brentuximab) o inmunoterapia (nivolumab)
- También se puede administrar radioterapia en las zonas donde está el cáncer.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del linfoma de Hodgkin nodular con predominio linfocítico infantil
For information about the treatments listed below, visit the Treatment Option Overview section.
El tratamiento del linfoma de Hodgkin nodular con predominio de linfocitos recién diagnosticado en niños puede incluir:
- Cirugía, si el tumor puede extirparse por completo.
- Quimioterapia con o sin radioterapia externa de dosis baja
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del linfoma de Hodgkin primario refractario o recidivante en niños y adolescentes
For information about the treatments listed below, visit the Treatment Option Overview section.
En niños y adolescentes, el tratamiento del linfoma de Hodgkin primario refractario (cáncer que no responde al tratamiento inicial) o del linfoma de Hodgkin recurrente (cáncer que reaparece después del tratamiento) puede incluir:
- Quimioterapia con o sin esteroides, terapia dirigida (rituximab, brentuximab o bortezomib) o ambas terapias
- Inmunoterapia (pembrolizumab o nivolumab)
- Quimioterapia de dosis alta con trasplante de células madre del propio paciente. También se puede administrar terapia con anticuerpos monoclonales (brentuximab).
- Se puede administrar radioterapia después del trasplante de células madre del propio paciente o si la enfermedad no ha respondido a otros tratamientos y el área con cáncer no ha sido tratada previamente.
- Quimioterapia de dosis alta con trasplante de células madre de un donante
- Terapia dirigida (brentuximab) como terapia de mantenimiento y consolidación para pacientes que han recaído después de un trasplante de células madre con las propias células madre del paciente.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Cómo afrontar el cáncer de su hijo o hija
Cuando su hijo o hija tiene cáncer, todos los miembros de la familia necesitan apoyo. Cuidarse durante este momento difícil es importante. Busque apoyo en el equipo de tratamiento de su hijo o hija, así como en familiares y comunidades. Para obtener más información, visite la página de Apoyo para familias: cáncer infantil y Niños con cáncer: una guía para padres.
Más información sobre el linfoma de Hodgkin infantil
Para obtener más información del National Cancer Institute sobre el linfoma de Hodgkin infantil, visite:
- Tomografía computarizada para el cáncer
- Medicamentos aprobados para el linfoma de Hodgkin
- Terapia dirigida para tratar el cáncer
- Immunotherapy to Treat Cancer
- Trasplantes de células madre en el tratamiento del cáncer
Para obtener más información sobre el cáncer infantil y otros recursos generales sobre el cáncer, consulte los siguientes sitios web:
- El cáncer
- Cánceres infantiles
- CureSearch para el cáncer infantil
- Efectos tardíos del tratamiento del cáncer infantil
- Adolescentes y adultos jóvenes con cáncer
- Niños con cáncer: una guía para padres
- El cáncer en los niños y los adolescentes
- Estadificación del cáncer
- Cómo hacer frente al cáncer
- Preguntas para el médico sobre el cáncer
- Para supervivientes, cuidadores e intercesores
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen del PDQ sobre el cáncer contiene información actualizada del tratamiento del linfoma de Hodgkin infantil. El propósito es informar y ayudar a los pacientes, sus familiares y cuidadores. No da pautas ni recomendaciones formales para tomar decisiones relacionadas con la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
La información de este resumen para pacientes procede de la versión para profesionales de la salud, la cual es revisada y actualizada periódicamente por el comité editorial del PDQ sobre el tratamiento pediátrico según sea necesario.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre el tratamiento pediátrico. Tratamiento del linfoma de Hodgkin infantil (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Actualizado:
URL de origen: https://www.cancer.gov/node/4743/syndication
Agencia de origen: National Cancer Institute (NCI)
Fecha de captura: 2013-09-14 09:02:25.0