








Tratamiento de tumores de células germinales extracraneales
If your child has been diagnosed with an extracranial germ cell tumor—a cancerous or noncancerous growth that develops outside of the brain in a type of cell that normally becomes either sperm or egg—you can depend on the expert care provided at Montefiore Einstein Comprehensive Cancer Center at the Children’s Hospital at Montefiore Einstein (CHAM).
Our multidisciplinary and collaborative approach to research and treatment ensures your child will receive the best care. We offer the most advanced treatments available, including clinical trials. We’re actively engaged in defining the next generation of treatment.
Con médicos, enfermeros, especialistas y personal de apoyo excepcionales, nuestro enfoque multidisciplinario y colaborativo para el tratamiento garantiza la mejor atención para su hijo o hija en un entorno de apoyo y cariño.
Si lo que usted desea es lo mejor para su hijo, acuda a los especialistas del Centro Oncológico Integral Montefiore Einstein en CHAM, quienes se dedican con pasión a erradicar el cáncer y a atender todas las necesidades de salud de su hijo.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Childhood Extracranial Germ Cell Tumors Treatment (PDQ®)–Patient Version
General Information About Childhood Extracranial Germ Cell Tumors
Puntos clave
- Childhood extracranial germ cell tumors start in germ cells in parts of the body other than the brain.
- Childhood extracranial germ cell tumors may be benign or malignant.
- Childhood extracranial germ cell tumors are grouped as gonadal or extragonadal extracranial tumors.
- Gonadal germ cell tumors
- Extragonadal extracranial germ cell tumors
- There are three types of extracranial germ cell tumors.
- Teratomas
- Malignant germ cell tumors
- Mixed germ cell tumors
- The cause of most childhood extracranial germ cell tumors is unknown.
- Having certain inherited disorders can increase the risk of extracranial germ cell tumors.
- Signs of childhood extracranial germ cell tumors depend on where the tumor formed in the body.
- Imaging studies and blood tests are used to diagnose childhood extracranial germ cell tumors.
- Hay ciertos factores que afectan al pronóstico (probabilidad de recuperación) y a las opciones de tratamiento.
Childhood extracranial germ cell tumors start in germ cells in parts of the body other than the brain.
A germ cell is a type of cell that forms as a fetus develops. These cells later become sperm in the testicles or eggs in the ovaries.
This summary is about germ cell tumors that form in parts of the body that are extracranial (outside the brain). Extracranial germ cell tumors usually form in the following areas of the body:
- Testicles.
- Ovaries.
- Sacrum or coccyx (tailbone).
- Retroperitoneum (area in the back of the abdomen behind the tissue that lines the abdominal wall and covers most of the organs in the abdomen).
- Mediastinum (area between the lungs).
- Head and neck.
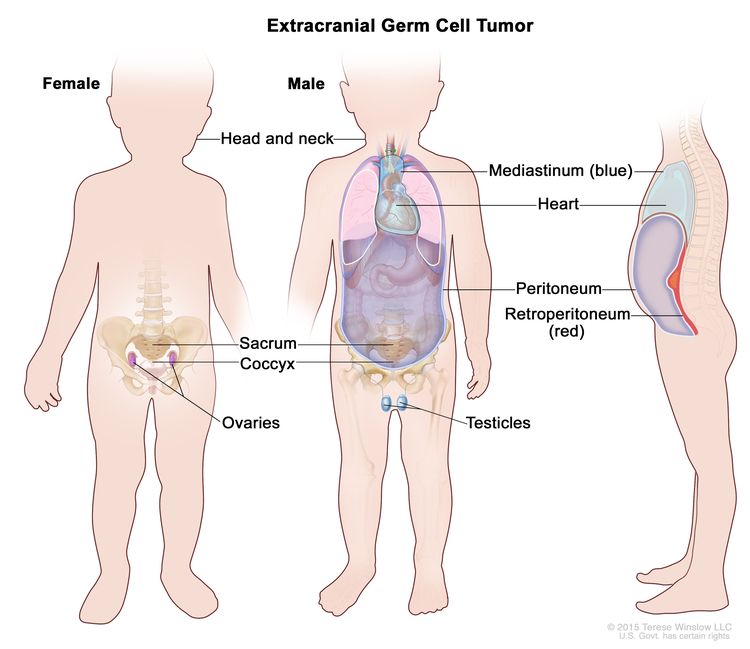
Extracranial germ cell tumors form in parts of the body other than the brain. This includes the testicles, ovaries, sacrum (lower part of the spine), coccyx (tailbone), mediastinum (area between the lungs), retroperitoneum (the back wall of the abdomen), and the head and neck.
Extracranial germ cell tumors are most common in adolescents, with rates in this age group lower for females than males.
For information on intracranial (inside the brain) germ cell tumors, see Childhood Central Nervous System Germ Cell Tumors Treatment.
Childhood extracranial germ cell tumors may be benign or malignant.
Extracranial germ cell tumors may be benign (noncancer) or malignant (cancer).
Childhood extracranial germ cell tumors are grouped as gonadal or extragonadal extracranial tumors.
Malignant extracranial germ cell tumors are tumors that form outside the brain. They are gonadal or extragonadal.
Gonadal germ cell tumors
Gonadal germ cell tumors form in the gonads (testicles and ovaries).
- Testicular germ cell tumors. Testicular germ cell tumors are divided into two main types, seminoma y nonseminoma. Nonseminomas are usually large and cause signs or síntomas of disease. They tend to grow and spread more quickly than seminomas.
Testicular germ cell tumors usually occur before the age of 5 years or in adolescents and young adults. Testicular germ cell tumors in adolescents (11 years and older) and young adults are different from those that form in early childhood.
- Ovarian germ cell tumors. Ovarian germ cell tumors are more common in adolescent girls and young women. Most ovarian germ cell tumors are benign mature teratomas (dermoid cysts). Some ovarian germ cell tumors, such as immature teratomas, dysgerminomas, yolk sac tumors, or mixed germ cell tumors, are malignant.
Extragonadal extracranial germ cell tumors
Extragonadal extracranial germ cell tumors form in areas of the body other than the brain or gonads (testicles and ovaries).
Most extragonadal extracranial germ cell tumors form along the midline of the body. This includes the following:
- Sacrum (the large, triangle-shaped bone in the lower spine that forms part of the pelvis).
- Coccyx (tailbone).
- Mediastinum (the area between the lungs).
- Back of the abdomen.
- Neck.
In children younger than 11 years, extragonadal extracranial germ cell tumors usually occur at birth or in early childhood. Most of these tumors are benign teratomas in the sacrum or coccyx.
In older children, adolescents, and young adults (11 years and older), extragonadal extracranial germ cell tumors are often in the mediastinum.
There are three types of extracranial germ cell tumors.
Extracranial germ cell tumors are also grouped into teratomas, malignant germ cell tumors, and mixed germ cell tumors:
Teratomas
There are two main types of teratomas:
- Mature teratomas. These tumors are the most common type of extracranial germ cell tumor. Mature teratomas are benign tumors and not likely to become cancer. They usually occur in the sacrum or coccyx in newborns or in the testicles or ovaries at the start of puberty. The cells of mature teratomas look almost like normal cells under a microscope. Some mature teratomas release enzymes or hormones that cause signs and symptoms of disease.
- Immature teratomas. These tumors usually occur in areas other than the gonads in young children or in the ovaries at the start of puberty. They have cells that look very different from normal cells under a microscope. Immature teratomas may be cancer and spread to other parts of the body. They often have several different types of tissue in them, such as hair, muscle, and bone. Some immature teratomas release enzymes or hormones that cause signs and symptoms of disease.
Malignant germ cell tumors
Malignant germ cell tumors are cancer. There are two main types of malignant germ cell tumors:
- Seminomatous germ cell tumors. There are three types of seminomatous germ cell tumors:
- Seminomas form in the testicle.
- Dysgerminomas form in the ovary.
- Germinomas form in areas of the body that are not the ovary or testicle, such as the mediastinum.
- Nonseminomatous germ cell tumors. There are four types of nonseminomatous germ cell tumors:
- Yolk sac tumors make a hormone called alpha-fetoprotein (AFP). They can form in the ovary, testicle, or other areas of the body.
- Choriocarcinomas make a hormone called beta-human chorionic gonadotropin (beta-hCG). They can form in the ovary, testicle, or other areas of the body.
- Embryonal carcinomas may make a hormone called beta-hCG. They can form in the testicle or other areas of the body, but not in the ovary.
- Gonadoblastomas can form in the ovary.
Mixed germ cell tumors
Mixed germ cell tumors are made up of at least two types of malignant germ cell tumor. They can form in the ovary, testicle, or other areas of the body.
The cause of most childhood extracranial germ cell tumors is unknown.
Having certain inherited disorders can increase the risk of extracranial germ cell tumors.
A risk factor is anything that increases the chance of getting a disease. Not every child with one or more of these risk factors will develop an extracranial germ cell tumor. And it will develop in some children who don't have a known risk factor.
Possible risk factors for extracranial germ cell tumors include:
- Having certain genetic syndromes:
- Klinefelter syndrome may increase the risk of germ cell tumors in the mediastinum.
- Swyer syndrome may increase the risk of gonadoblastoma and seminoma.
- Turner syndrome may increase the risk of gonadoblastoma and dysgerminoma.
- Having an undescended testicle may increase the risk of testicular cancer.
- Having an ovary or testicle that has not formed normally (gonadal dysgenesis) may increase the risk of gonadoblastoma.
Hable con el médico de su hijo si cree que su hijo puede estar en riesgo.
Signs of childhood extracranial germ cell tumors depend on where the tumor formed in the body.
Different tumors may cause the following signs and symptoms. Other conditions may cause these same signs and symptoms. It's important to check with your child's doctor if your child has:
- A lump in the neck, abdomen, or lower back.
- A painless lump in the testicle.
- Dolor en el abdomen o la espalda
- Respiratory distress, chest pain, or cough.
- Fever.
- Constipación.
- Trouble urinating.
- Early puberty.
- In females, no menstrual periods or unusual vaginal bleeding.
Imaging studies and blood tests are used to diagnose childhood extracranial germ cell tumors.
If your child has symptoms that suggest they have an extracranial germ cell tumor, their doctor will need to find out if these are due to cancer or another problem. The doctor will ask when the symptoms started and how often your child has been having them. They will also ask about your child's personal and family medical history and do a physical exam. Depending on these results, they may recommend other tests. If your child is diagnosed with an extracranial germ cell tumor, the results of these tests will help you and your child's doctor plan treatment.
The tests used to diagnose extracranial germ cell tumors may include:
- Pruebas séricas de marcadores tumorales: procedimiento en el que se toma una muestra de sangre is checked to measure the amounts of certain substances released into the blood by organs, tissues, or tumor cells in the body. Certain substances are linked to specific types of cancer when found in increased levels in the blood. These are called marcadores tumorales.
Some malignant germ cell tumors release tumor markers. The following tumor markers may be used to detect extracranial germ cell tumors:
- Alpha-fetoprotein (AFP).
- Beta-human chorionic gonadotropin (beta-hCG).
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body, including lactate dehydrogenase. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- Tomografía computarizada (TC): A procedure that makes a series of detailed pictures of areas inside the body, such as the chest or ganglios linfáticos, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A tinte puede inyecta en una vena o ser ingerido a fin de que los órganos o los tejidos se destaquen de forma más clara. Este procedimiento también se llama tomografía computadorizada, tomografía axial computarizada (TAC) o exploración por TAC.
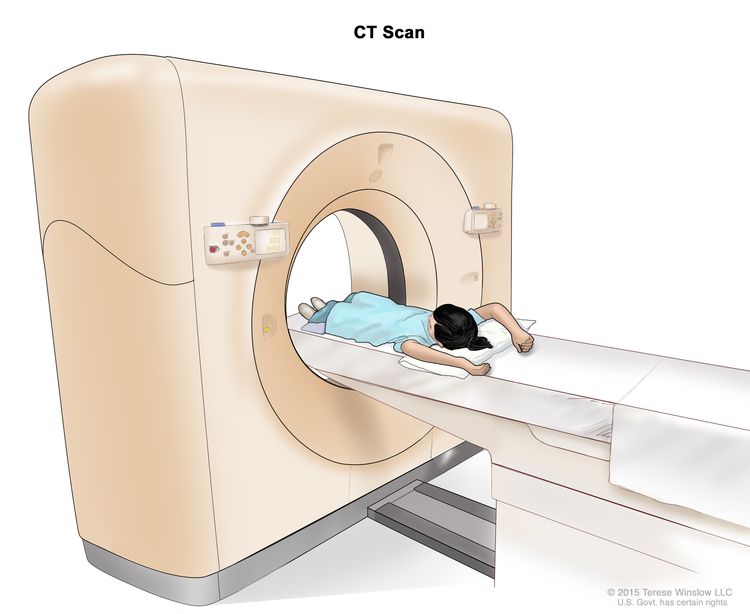
Computed tomography (CT) scan. The child lies on a table that slides through the CT scanner, which takes a series of detailed x-ray pictures of areas inside the body.
- Resonancia magnética: A procedure that uses a magnet, radio wavesy una computadora para generar una serie de imágenes detalladas de áreas internas del cuerpo. Este procedimiento también se denomina resonancia magnética nuclear (RMN).
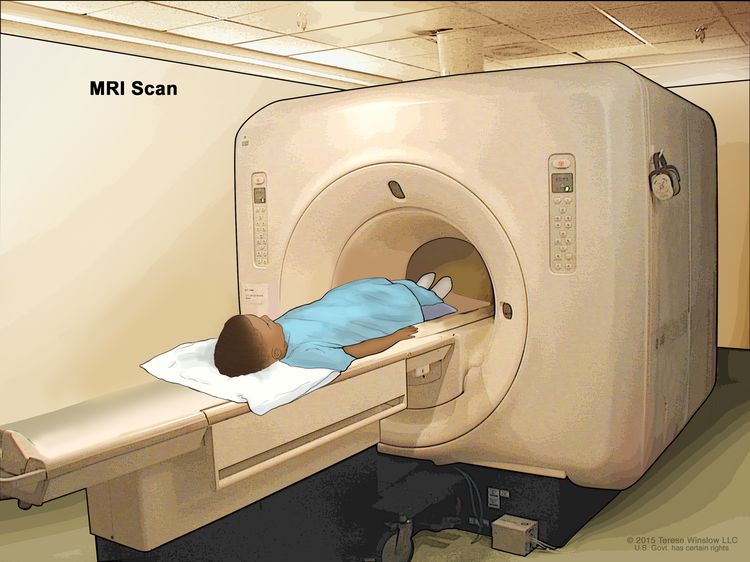
Magnetic resonance imaging (MRI) scan. The child lies on a table that slides into the MRI machine, which takes a series of detailed pictures of areas inside the body. The positioning of the child on the table depends on the part of the body being imaged.
- Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a ecograma. La imagen se puede imprimir para verla más tarde.
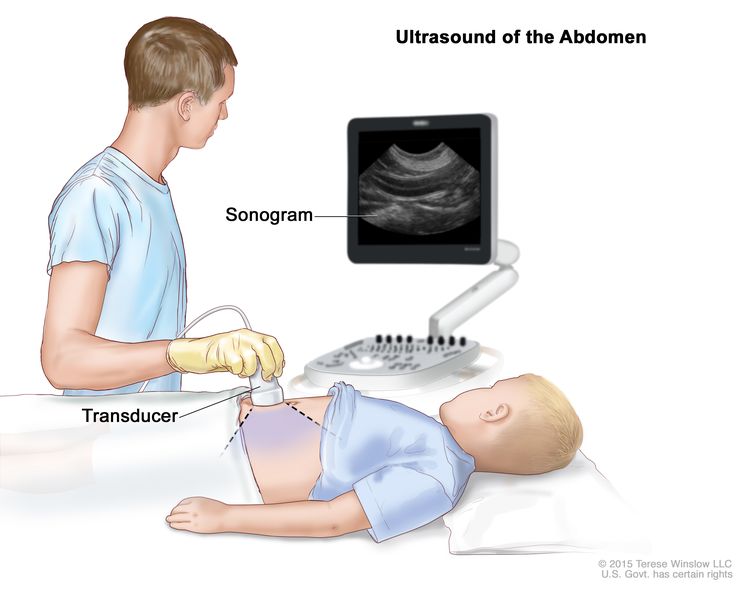
Ultrasonido abdominal: se presiona un transductor de ultrasonido conectado a una computadora contra la piel del abdomen. El transductor hace rebotar ondas de sonido en los órganos y tejidos internos para producir ecos que forman un ecograma (imagen de computadora).
- Biopsia: The removal of cells or tissues so they can be viewed under a microscope by a patólogo to check for signs of cancer. Sometimes an incisional biopsy or needle biopsy is done before Cirugía to remove a sample of tissue. Sometimes the tumor is removed during surgery and then a sample of tissue is removed from the tumor.
The following tests may be done on the sample of tissue that is removed:
- Cytogenetic analysis: A laboratory test in which the chromosomes of cells in a sample of tissue are counted and checked for any changes, such as broken, missing, rearranged, or extra chromosomes. Changes in certain chromosomes may be a sign of cancer. Cytogenetic analysis is used to help diagnose cancer, plan treatment, or find out how well treatment is working.
- Immunohistochemistry: A laboratory test that uses antibodies to check for certain antigens (markers) in a sample of a patient's tissue. The antibodies are usually linked to an enzyme or a fluorescent dye. After the antibodies bind to a specific antigen in the tissue sample, the enzyme or dye is activated, and the antigen can then be seen under a microscope. This type of test is used to help diagnose cancer and to help tell one type of cancer from another type of cancer.
Hay ciertos factores que afectan al pronóstico (probabilidad de recuperación) y a las opciones de tratamiento.
El pronóstico y las opciones de tratamiento dependen de los siguientes factores:
- The child's age and general health.
- The stage of the cancer (whether it has spread to nearby areas, lymph nodes, or to other places in the body).
- Where the tumor first began to grow.
- The type of germ cell tumor.
- How well the tumor responds to treatment.
- Whether the child has gonadal dysgenesis.
- Whether the tumor can be completely removed by surgery.
- Whether the cancer has just been diagnosed or has recurred (come back).
The prognosis for childhood extracranial germ cell tumors, especially ovarian germ cell tumors, is good.
Stages of Childhood Extracranial Germ Cell Tumors
Puntos clave
- After a childhood extracranial germ cell tumor has been diagnosed, tests are done to find out if cancer cells have spread from where the tumor started to nearby areas or to other parts of the body.
- El cáncer se propaga por el cuerpo de tres maneras.
- El cáncer puede extenderse desde donde comenzó a otras partes del cuerpo.
- Stages are used to describe the different types of extracranial germ cell tumors.
- Testicular germ cell tumors in children younger than 11 years
- Testicular germ cell tumors in adolescents and young adults 11 years and older
- Ovarian germ cell tumors
- Extragonadal extracranial germ cell tumors
- Childhood extracranial germ cell tumors usually do not come back after treatment.
After a childhood extracranial germ cell tumor has been diagnosed, tests are done to find out if cancer cells have spread from where the tumor started to nearby areas or to other parts of the body.
The process used to find out if cancer has spread from where the tumor started to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment. In some cases, staging may follow surgery to remove the tumor.
The following procedures may be used:
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body, such as the brain or lymph nodes. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the chest or lymph nodes, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- Bone scan: A procedure to check if there are rapidly dividing cells, such as cancer cells, in the bone. A very small amount of radioactive material is injected into a vein and travels through the bloodstream. The radioactive material collects in the bones with cancer and is detected by a scanner.
- Thoracentesis: The removal of fluid from the space between the lining of the chest and the lung, using a needle. A pathologist views the fluid under a microscope to look for cancer cells.
- Paracentesis: The removal of fluid from the space between the lining of the abdomen and the organs in the abdomen, using a needle. A pathologist views the fluid under a microscope to look for cancer cells.
The results from tests and procedures used to detect and diagnose childhood extracranial germ cell tumors may also be used in staging.
El cáncer se propaga por el cuerpo de tres maneras.
El cáncer puede extenderse a través de los tejidos circundantes, el sistema linfático y la sangre:
- Tejidos: el cáncer se extiende desde el lugar donde comenzó y crece hacia las zonas circundantes.
- Sistema linfático: el cáncer se extiende desde el lugar donde comenzó hacia el sistema linfático. El cáncer viaja a través de los vasos linfáticos a otras partes del cuerpo.
- Sangre: el cáncer se extiende desde el lugar donde comenzó hacia la sangre. El cáncer viaja a través de los vasos sanguíneos a otras partes del cuerpo.
El cáncer puede extenderse desde donde comenzó a otras partes del cuerpo.
Cuando el cáncer se extiende a otra parte del cuerpo se denomina metástasis. Las células cancerosas se desprenden de donde comenzaron (tumor primario) y viajan a través del sistema linfático o la sangre.
- Sistema linfático: el cáncer entra en el sistema linfático, viaja a través de los vasos linfáticos y forma un tumor (tumor metastásico) en otra parte del cuerpo.
- Sangre: el cáncer llega a la sangre, viaja a través de los vasos sanguíneos y forma un tumor (tumor metastásico) en otra parte del cuerpo.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if an extracranial germ cell tumor spreads to the liver, the cancer cells in the liver are actually cancerous germ cells. The disease is metastatic extracranial germ cell tumor, not liver cancer.
Stages are used to describe the different types of extracranial germ cell tumors.
Testicular germ cell tumors in children younger than 11 years
The following stages are from the Children's Oncology Group.
- Estadio I
In stage I, the cancer is found in the testicle only. The testicle and spermatic cord are completely removed by surgery and all of the following are true:
- the capsule (outer covering of the tumor) did not rupture (break open) and a biopsy was not done before the tumor was removed; and
- all lymph nodes are smaller than 1 centimeter in their shortest diameter on a CT scan or MRI.
- Estadio II
In stage II, the testicle and spermatic cord are removed by surgery and one of the following is true:
- the capsule (outer covering of the tumor) ruptured (broke open) or a biopsy was done before surgery; or
- cancer that can only be seen with a microscope remains in the scrotum or in the spermatic cord near the scrotum, and after surgery, tumor marker levels do not return to normal or do not decrease.
Cancer has not spread to the lymph nodes.
- Estadio III
In stage III, one of the following is true:
- the cancer has spread to one or more lymph nodes at the back of the abdomen; or
- lymph nodes are at least 2 centimeters wide or are larger than 1 centimeter but smaller than 2 centimeters in their shortest diameter and either have not changed or are growing when a CT scan or MRI is repeated within 4 to 6 weeks.
- Estadio IV
In stage IV, the cancer has spread to other parts of the body, such as the liver, lung, bone, and brain.
Testicular germ cell tumors in adolescents and young adults 11 years and older
En varones mayores de 15 años, solo existen tumores en estadio I y tumores metastásicos. Para obtener más información sobre la estadificación utilizada para los tumores de células germinales testiculares en adolescentes y adultos jóvenes de 11 años o más, consulte Estadios del cáncer testicular .
Ovarian germ cell tumors
Two staging systems are used for ovarian germ cell tumors: Children's Oncology Group and the International Federation of Gynecology and Obstetrics (FIGO).
The following stages are from the Children's Oncology Group.
- Estadio I
In stage I, the tumor in the ovary is completely removed by surgery and all of the following are true:
- the capsule (outer covering of the tumor) did not rupture (break open) and a biopsy was not done before the tumor was removed; and
- there is no sign that the cancer has spread through the capsule; and
- no cancer cells are found in fluid taken from the abdomen; and
- no cancer is seen in tissue that lines the abdomen or found in tissue samples taken during a biopsy; and
- lymph nodes are smaller than 1 centimeter in their shortest diameter on a CT scan or MRI or no cancer is found in lymph node tissue samples taken during a biopsy.
- Estadio II
In stage II, the tumor in the ovary is completely removed by surgery and a biopsy is done before surgery and one of the following is true:
- cancer has spread through part or all of the capsule (outer covering of the tumor); or
- the tumor is larger than 10 centimeters and is removed by laparoscopic surgery; or
- the tumor is removed by being broken up into small pieces and it is not known if cancer has spread through the capsule.
Cancer cells are not found in fluid taken from the abdomen. Cancer is not seen in lymph nodes or tissue that lines the abdomen and cancer is not found in tissue samples taken during a biopsy.
- Estadio III
In stage III, there is tumor in the ovary and one of the following is true:
- lymph nodes are at least 2 centimeters wide or are larger than 1 centimeter but smaller than 2 centimeters in their shortest diameter and either have not changed or are growing when a CT scan or MRI is repeated 4 to 6 weeks after surgery; or
- the tumor is not completely removed by surgery or a biopsy was done before surgery; or
- cancer cells (including immature teratoma) are found in fluid taken from the abdomen; or
- cancer (including immature teratoma) is found in lymph nodes; or
- cancer (including immature teratoma) is found in tissue that lines the abdomen.
- Stage III-X
In stage III-X, the tumor can be described as stage I or stage II, except:
- cells lining the abdomen were not collected; or
- a biopsy of lymph nodes larger than 1 centimeter in their shortest diameter was not done; or
- a biopsy of tissue from the lining of the abdomen was not done; or
- staging was not completed during surgery but will be completed during a second surgery.
- Estadio IV
In stage IV, one of the following is true:
The following stages are from the International Federation of Gynecology and Obstetrics (FIGO).
- Estadio I
In stage I, cancer is found in one or both of the ovaries and has not spread. Stage I is divided into stage IA, stage IB, and stage IC.
- Stage IA: Cancer is found in one ovary.
- Stage IB: Cancer is found in both ovaries.
- Stage IC: Cancer is found in one or both ovaries and one of the following is true:
- cancer is also found on the outside surface of one or both ovaries; or
- the capsule (outer covering) of the tumor ruptured (broke open) before or during surgery; or
- cancer cells are found in fluid taken from the abdomen or in washings of the peritoneal cavity (the body cavity that contains most of the organs in the abdomen).
- Estadio II
In stage II, cancer is found in one or both ovaries and has spread into other areas of the pelvis, or primary peritoneal cancer is found. Stage II is divided into stage IIA and stage IIB.
- Estadio III
In stage III, cancer is found in one or both ovaries or primary peritoneal cancer is found. Cancer has spread outside the pelvis to other parts of the abdomen and/or to lymph nodes at the back of the abdomen. Stage III is divided into stage IIIA, stage IIIB, and stage IIIC.
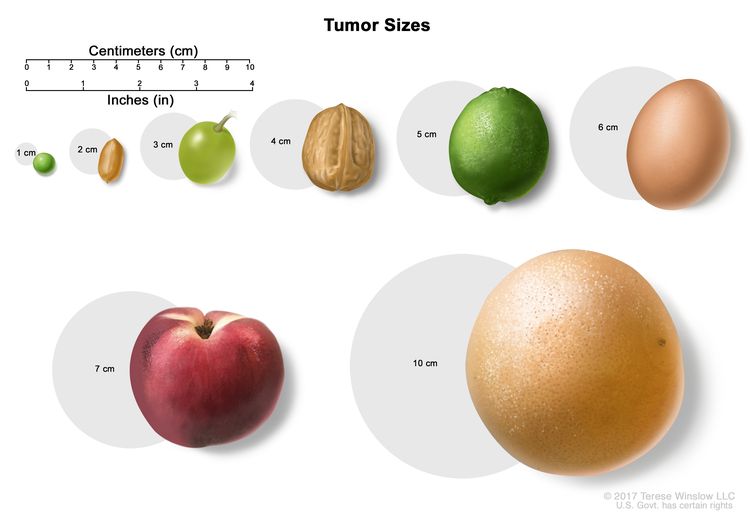
El tamaño de los tumores a menudo se mide en centímetros (cm) o pulgadas (in). A veces se usan alimentos comunes para mostrar el tamaño de un tumor en centímetros: una arveja o guisante (1 cm), un maní o cacahuate (2 cm), una uva (3 cm), una nuez (4 cm), una lima o limón verde (5 cm o 2 in), un huevo (6 cm), un durazno (7 cm) y un pomelo (10 cm o 4 in).
- En el estadio IIIA se cumple una de las siguientes condiciones:
- cancer has spread to lymph nodes at the back of the abdomen only; or
- cancer cells that can be seen only with a microscope have spread to the surface of the peritoneum outside the pelvis. Cancer may have spread to nearby lymph nodes at the back of the abdomen.
- Stage IIIB: Cancer has spread to the peritoneum outside the pelvis and the cancer in the peritoneum is 2 centimeters or smaller. Cancer may have spread to lymph nodes at the back of the abdomen.
- Stage IIIC: Cancer has spread to the peritoneum outside the pelvis and the cancer in the peritoneum is larger than 2 centimeters. Cancer may have spread to lymph nodes at the back of the abdomen or to the surface of the liver or spleen.
- En el estadio IIIA se cumple una de las siguientes condiciones:
- Estadio IV
Stage IV is divided into stage IVA and IVB.
Extragonadal extracranial germ cell tumors
The following stages are from the Children's Oncology Group.
- Estadio I
In stage I, the tumor is completely removed by surgery and all of the following are true:
- no cancer cells are found in the area where the tumor was removed; and
- the capsule (outer covering of the tumor) did not rupture (break open) and a biopsy was not done before the tumor was removed; and
- cancer cells are not found in fluid taken from the abdominal cavity, if the tumor is in the abdomen; and
- lymph nodes are smaller than 1 centimeter on a CT scan or MRI of the abdomen, pelvis, and chest.
- Estadio II
In stage II, cancer is not completely removed by surgery and one of the following is true:
- cancer that can only be seen with a microscope remains after surgery; or
- the capsule (outer covering of the tumor) ruptured (broke open) or a biopsy was done.
Cancer cells are not found in fluid taken from the abdomen. There is no sign of cancer in lymph nodes in the abdomen, pelvis, or chest on a CT scan or MRI.
- Estadio III
In stage III, one of the following is true:
- cancer is not completely removed by surgery and cancer that can be seen with the eye remains after surgery or only a biopsy was done; or
- lymph nodes are at least 2 centimeters wide or are larger than 1 centimeter but smaller than 2 centimeters in their shortest diameter and either have not changed or are growing when a CT scan or MRI is repeated within 4 to 6 weeks.
- Estadio IV
In stage IV, the cancer has spread to other parts of the body, such as the liver, lung, bone, or brain.
Childhood extracranial germ cell tumors usually do not come back after treatment.
Recurrent childhood extracranial germ cell tumor is cancer that has come back after it has been treated. The cancer may come back in the same place or in other parts of the body.
Most germ cell tumors do not recur (come back) after treatment. If they do recur, they usually come back within 3 years of surgery. About half of the teratomas that recur in the sacrum or coccyx are cancer, so follow-up is important.
Descripción general de las opciones de tratamiento
Puntos clave
- There are different types of treatment for children with extracranial germ cell tumors.
- Children with extracranial germ cell tumors should have their treatment planned by a team of health care providers who are experts in treating cancer in children.
- Se utilizan los siguientes tipos de tratamiento:
- Cirugía
- Observación
- Quimioterapia
- Se están probando nuevos tipos de tratamiento en ensayos clínicos.
- Quimioterapia de dosis alta con trasplante de células madre
- Radioterapia
- Treatment for childhood extracranial germ cell tumors may cause side effects.
- Los pacientes pueden evaluar la posibilidad de participar en un ensayo clínico.
- Los pacientes pueden participar en ensayos clínicos antes, durante o después de comenzar el tratamiento contra el cáncer.
- Pueden ser necesarias pruebas de seguimiento.
There are different types of treatment for children with extracranial germ cell tumors.
Different types of treatments are available for children with extracranial germ cell tumors. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment.
Dado que el cáncer infantil es poco frecuente, debe considerarse la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Children with extracranial germ cell tumors should have their treatment planned by a team of health care providers who are experts in treating cancer in children.
Treatment will be overseen by a pediatric oncologist, a doctor who specializes in treating children with cancer. The pediatric oncologist works with other health care providers who are experts in treating children with extracranial germ cell tumors and who specialize in certain areas of medicine. These may include the following specialists:
Se utilizan los siguientes tipos de tratamiento:
Cirugía
Surgery to completely remove the tumor is done whenever possible. If the tumor is very large, chemotherapy may be given first, to make the tumor smaller and decrease the amount of tissue that needs to be removed during surgery. A goal of surgery is to keep reproductive function. The following types of surgery may be used:
- Resection: Surgery to remove tissue or part or all of an organ.
- Radical inguinal orchiectomy: Surgery to remove one or both testicles through an incision (cut) in the groin.
- Unilateral salpingo-oophorectomy: Surgery to remove one ovary and one fallopian tube on the same side.
After the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given chemotherapy after surgery to kill any cancer cells that are left. Treatment given after surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
Observación
Observation is closely monitoring a patient's condition without giving any treatment until signs or symptoms appear or change. For children with extracranial germ cell tumors, this includes physical exams, imaging tests, and tumor marker tests.
Quimioterapia
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). Systemic chemotherapy is used to treat extracranial germ cell tumors.
Se están probando nuevos tipos de tratamiento en ensayos clínicos.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Learn more at Clinical Trials Information for Patients and Caregivers.
Quimioterapia de dosis alta con trasplante de células madre
High doses of chemotherapy are given to kill cancer cells. Healthy cells, including blood-forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the patient completes chemotherapy, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
Radioterapia
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer. External radiation therapy is being studied for the treatment of childhood extracranial germ cell tumors that have come back.
Treatment for childhood extracranial germ cell tumors may cause side effects.
Para obtener más información sobre los efectos secundarios que aparecen durante el tratamiento del cáncer, consulte la sección Efectos secundarios.
Los efectos secundarios del tratamiento del cáncer que comienzan después del tratamiento y continúan durante meses o años se denominan efectos tardíos. Los efectos tardíos del tratamiento del cáncer pueden ser:
- Physical problems, such as infertility, trouble hearing and kidney problems.
- Cambios en el estado de ánimo, los sentimientos, el pensamiento, el aprendizaje o la memoria
- Second cancers (new types of cancer), such as leukemia or malignant melanoma.
Some late effects may be treated or controlled. It is important to talk with your child's doctors about the effects cancer treatment can have on your child. For more information, see Late Effects of Treatment for Childhood Cancer.
Los pacientes pueden evaluar la posibilidad de participar en un ensayo clínico.
Para algunos pacientes, participar en un ensayo clínico puede ser la mejor opción de tratamiento. Los ensayos clínicos son parte del proceso de investigación del cáncer y se realizan para determinar si los nuevos tratamientos para el cáncer son seguros y eficaces o mejores que el tratamiento estándar.
Muchos de los tratamientos estándar actuales para el cáncer se basan en ensayos clínicos anteriores. Los pacientes que participan en un ensayo clínico pueden recibir el tratamiento estándar o ser de los primeros en recibir uno nuevo.
Los pacientes que participan en ensayos clínicos también ayudan a mejorar la forma en que se tratará el cáncer en el futuro. Incluso cuando los ensayos clínicos no conducen a nuevos tratamientos efectivos, suelen responder a preguntas clave y contribuir de forma significativa al avance de la investigación.
Los pacientes pueden participar en ensayos clínicos antes, durante o después de comenzar el tratamiento contra el cáncer.
Algunos ensayos clínicos solo incluyen a pacientes que aún no han recibido tratamiento. Otros ensayos prueban tratamientos para pacientes cuyo cáncer no ha mejorado. También hay ensayos clínicos que prueban nuevas formas de evitar que el cáncer recidive (regrese) o de reducir los efectos secundarios del tratamiento del cáncer.
Se están realizando ensayos clínicos en muchas partes del país. Puede encontrar información sobre los ensayos clínicos respaldados por el NCI en el sitio web de búsqueda de ensayos clínicos del NCI. Puede encontrar ensayos clínicos respaldados por otras organizaciones en el sitio web ClinicalTrials.gov.
Pueden ser necesarias pruebas de seguimiento.
Durante el tratamiento, su hijo/a se someterá a pruebas o revisiones de seguimiento. Algunas pruebas realizadas para diagnosticar o estadificar el cáncer podrían repetirse para evaluar la eficacia del tratamiento. Las decisiones sobre si continuar, modificar o suspender el tratamiento podrían basarse en los resultados de estas pruebas.
Algunas de las pruebas se seguirán realizando periódicamente después de que finalice el tratamiento. Los resultados de estas pruebas pueden mostrar si la afección de su hijo o hija ha cambiado o si el cáncer ha recidivado (regresado).
For childhood extracranial germ cell tumors, follow-up may include regular physical exams, tumor marker tests, and imaging tests such as CT scan, MRI or chest x-ray.
Treatment of Childhood Mature and Immature Teratomas
Para más información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
Treatment of newly diagnosed mature teratomas includes the following:
- Surgery to remove the tumor followed by observation.
Treatment of newly diagnosed immature teratomas includes the following:
- Surgery to remove the tumor followed by observation for stage I tumors.
- Surgery to remove the tumor for stage I–IV tumors. In young children, surgery is followed by observation; the use of chemotherapy after surgery is controversial. In adolescents and young adults, chemotherapy is given after surgery.
Sometimes a mature or immature teratoma also has malignant cells. A teratoma with malignant cells may need to be treated differently.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Treatment of Malignant Testicular Germ Cell Tumors
Para más información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
Treatment of newly diagnosed malignant testicular germ cell tumors may include the following:
For boys younger than 11 years:
- Surgery (radical inguinal orchiectomy) followed by observation for stage I tumors.
- Surgery (radical inguinal orchiectomy) followed by chemotherapy for stage II–IV tumors and repeat surgery to remove any remaining tumor.
- A clinical trial of a new regimen of surgery followed by observation for stage I tumors or chemotherapy for stage II–IV tumors.
For boys 11 years and older:
Malignant testicular germ cell tumors in boys 11 years and older are treated differently than they are in young boys. For more information, see Testicular Cancer Treatment.
- Surgery to remove the tumor. Sometimes lymph nodes in the abdomen are also removed.
- A clinical trial of a new regimen of surgery followed by observation for stage I tumors or chemotherapy for stage II–IV tumors.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Treatment of Malignant Ovarian Germ Cell Tumors
Dysgerminomas
Para más información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
Treatment of newly diagnosed stage I dysgerminomas of the ovary may include the following:
- Surgery (unilateral salpingo-oophorectomy) followed by observation. Chemotherapy may be given if tumor marker levels do not decrease after surgery or the tumor comes back.
- A clinical trial of a new regimen of surgery followed by observation.
Treatment of newly diagnosed stages II–IV dysgerminomas of the ovary may include the following:
- Surgery (unilateral salpingo-oophorectomy) followed by chemotherapy.
- Chemotherapy to shrink the tumor, followed by surgery (unilateral salpingo-oophorectomy).
Nongerminomas
Para más información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
Treatment of newly diagnosed nongerminomas of the ovary, such as yolk sac tumors, mixed germ cell tumors, choriocarcinoma, and embryonal carcinomas, in young girls may include the following:
- Surgery followed by observation for stage I tumors.
- Surgery followed by chemotherapy for stage I–IV tumors.
- A clinical trial of a new regimen of surgery followed by observation for stage I tumors or chemotherapy for stage II–IV.
Treatment of newly diagnosed nongerminomas of the ovary in adolescents and young women may include the following:
- Surgery and chemotherapy for stage I–IV tumors.
- A clinical trial of a new regimen of surgery followed by observation for stage I or chemotherapy for stage II–IV.
Treatment of newly diagnosed nongerminomas of the ovary that cannot be removed by primary surgery without risk to nearby tissue may include the following:
- Biopsy followed by chemotherapy and surgery.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Treatment of Malignant Extragonadal Extracranial Germ Cell Tumors
Para más información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
Treatment of newly diagnosed childhood malignant extragonadal extracranial germ cell tumors in young children may include the following:
- Surgery and chemotherapy for stage I–IV tumors.
- Biopsy followed by chemotherapy with or without surgery for stage III and IV tumors.
In addition to stage of the disease, treatment of malignant extragonadal extracranial germ cell tumors also depends on where the tumor formed in the body:
- For tumors in the sacrum or coccyx, chemotherapy to shrink the tumor followed by surgery to remove the tumor and coccyx.
- For tumors in the mediastinum, chemotherapy before or after surgery to remove the tumor in the mediastinum.
- For tumors in the abdomen, biopsy followed by chemotherapy to shrink the tumor and surgery to remove the tumor in the abdomen.
- For tumors in the head and neck, surgery to remove the tumor in the head or neck, which may be followed by chemotherapy if the tumor is cancer.
Treatment of newly diagnosed childhood malignant extragonadal extracranial germ cell tumors in adolescents and young adults may include the following:
- Cirugía
- Quimioterapia
- Chemotherapy followed by surgery to remove the tumor.
- Un ensayo clínico de un nuevo régimen de cirugía seguida de observación para tumores en estadio I o quimioterapia para tumores en estadio II a IV.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento de tumores malignos de células germinales extracraneales recurrentes en la niñez
Para más información sobre los tratamientos que se enumeran a continuación, consulte la sección Aspectos generales de las opciones de tratamiento.
El tratamiento de los tumores de células germinales extracraneales infantiles recidivantes puede consistir en:
- Cirugía.
- Quimioterapia administrada antes o después de la cirugía para la mayoría de los tumores malignos de células germinales extracraneales, incluidos los teratomas inmaduros, los tumores malignos de células germinales testiculares y los tumores malignos de células germinales ováricas.
- Quimioterapia para tumores malignos recidivantes de células germinales testiculares y no germinomas recidivantes del ovario que estaban en estadio I al momento del diagnóstico.
- Quimioterapia de dosis alta y trasplante de células madre
- Radioterapia seguida de cirugía para extirpar el cáncer que se ha propagado al cerebro.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
To Learn More About Childhood Cancer
Para obtener más información del National Cancer Institute sobre los tumores de células germinales extracraneales infantiles, consulte las siguientes páginas web:
- Página de inicio de Tumor de células germinales extracraneal (infancia)
- Tomografía computarizada para el cáncer
- Terapia dirigida para tratar el cáncer
Para obtener más información sobre el cáncer infantil y otros recursos generales sobre el cáncer, consulte los siguientes sitios web:
- El cáncer
- Cánceres infantiles
- CureSearch para el cáncer infantil
- Efectos tardíos del tratamiento del cáncer infantil
- Adolescentes y adultos jóvenes con cáncer
- Niños con cáncer: una guía para padres
- El cáncer en los niños y los adolescentes
- Estadificación del cáncer
- Cómo hacer frente al cáncer
- Preguntas para el médico sobre el cáncer
- Para supervivientes, cuidadores e intercesores
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen del PDQ sobre el cáncer contiene información actualizada del tratamiento de los tumores extracraneales de células germinativas en la niñez. El propósito es informar y ayudar a los pacientes, sus familiares y cuidadores. No da pautas ni recomendaciones formales para tomar decisiones relacionadas con la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
La información de este resumen para pacientes procede de la versión para profesionales de la salud, la cual es revisada y actualizada periódicamente por el comité editorial del PDQ sobre el tratamiento pediátrico según sea necesario.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre el tratamiento pediátrico. Tratamiento de tumores extracraneales de células germinales infantiles (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Actualizado:
URL de origen: https://www.cancer.gov/node/2599/syndication
Agencia de origen: National Cancer Institute (NCI)
Fecha de captura: 14/09/2013 09:01:05.0