








Neuroblastoma
En el Montefiore Einstein Comprehensive Cancer Center, nuestros oncólogos especializados están a su disposición para diagnosticar y tratar el neuroblastoma con la mayor experiencia y dedicación. Le ofrecemos tratamientos de última generación y un acompañamiento integral para usted y sus seres queridos en cada etapa del proceso.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Tratamiento del neuroblastoma (PDQ®): versión para pacientes
Información general sobre el neuroblastoma
Puntos clave
- El neuroblastoma es un tipo de cáncer que se forma en los neuroblastos (tejido nervioso inmaduro) de las glándulas suprarrenales, el cuello, el pecho o la médula espinal.
- Ciertas afecciones genéticas aumentan el riesgo de tener neuroblastoma.
- Las pruebas genéticas pueden determinar si un niño tiene una forma hereditaria de neuroblastoma.
- En ocasiones, es necesario examinar a los niños con determinadas mutaciones genéticas para detectar signos de neuroblastoma.
- Los signos y síntomas del neuroblastoma pueden ser dolor de huesos o un bulto en el abdomen, el cuello o el pecho.
- Para diagnosticar el neuroblastoma se utilizan pruebas que examinan muchos tejidos y fluidos corporales diferentes.
- Los pacientes pueden obtener una segunda opinión.
- Certain factors affect prognosis (chance of recovery) and treatment options.
El neuroblastoma es un tipo de cáncer que se forma en los neuroblastos (tejido nervioso inmaduro) de las glándulas suprarrenales, el cuello, el pecho o la médula espinal.
El neuroblastoma a menudo comienza en el tejido nervioso de las glándulas suprarrenales. Hay dos glándulas suprarrenales, una encima de cada riñón en la parte posterior de la parte superior del abdomen. Las glándulas suprarrenales producen hormonas importantes que ayudan a controlar la frecuencia cardiaca, la presión arterial, el azúcar en sangre y la forma en que el cuerpo reacciona al estrés.
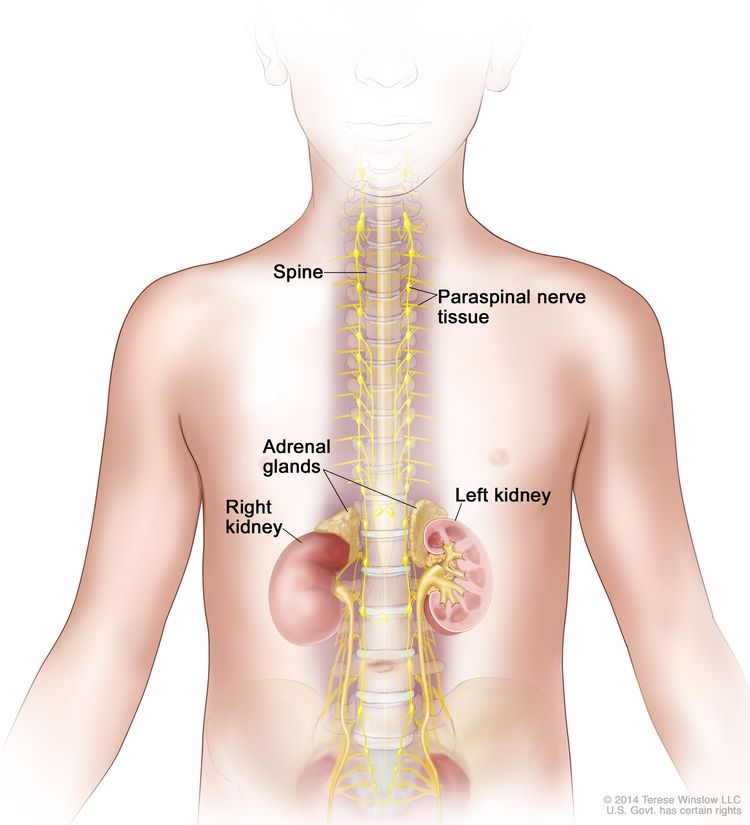
El neuroblastoma se puede encontrar en las glándulas suprarrenales y en el tejido nervioso paraespinal, que va desde el cuello hasta la pelvis.
El neuroblastoma suele comenzar en la infancia. Suele diagnosticarse entre el primer mes de vida y los 5 años. El tumor se encuentra cuando comienza a crecer y causar signos o síntomas. A veces se forma antes del nacimiento y se detecta durante una ecografía del bebé.
Para cuando se diagnostica el cáncer, por lo general ya se ha metastatizado (extendido). El neuroblastoma suele extenderse a los ganglios linfáticos, los huesos, la médula ósea, el hígado y la piel en bebés y niños. Los adolescentes también pueden presentar metástasis en los pulmones y el cerebro.
Ciertas afecciones genéticas aumentan el riesgo de tener neuroblastoma.
El neuroblastoma se produce por ciertos cambios en el funcionamiento de los neuroblastos, especialmente en su crecimiento y división en nuevas células. Hay muchos factores de riesgo de neuroblastoma, pero muchos no causan cáncer directamente. En cambio, aumentan la probabilidad de que se produzcan daños en el ADN de las células que pueden dar lugar a un neuroblastoma. Obtenga más información sobre cómo se desarrolla el cáncer en ¿Qué es el cáncer?
Un factor de riesgo es cualquier factor que aumenta la probabilidad de contraer una enfermedad. Algunos factores de riesgo se pueden modificar. También incluyen factores que no se pueden modificar, como el historial familiar. Es importante conocer los factores de riesgo del neuroblastoma, ya que pueden ayudar a tomar decisiones sobre los exámenes de detección del cáncer.
Los posibles factores de riesgo del neuroblastoma pueden ser:
- Tener ciertos cambios en los genes (ALK o PHOX2B)
- having certain afecciones genéticas conditions, such as:
- Síndrome de Costello
- Síndrome de Noonan
- Neurofibromatosis tipo 1
- Síndrome de Li-Fraumeni
- Síndrome de Beckwith-Wiedemann
- Síndromes de feocromocitoma/paraganglioma
- Síndromes de ROHHAD (obesidad de aparición rápida, disfunción hipotalámica, hipoventilación y disfunción autonómica)
- Tener un historial familiar importante de neuroblastoma
Las pruebas genéticas pueden determinar si un niño tiene una forma hereditaria de neuroblastoma.
Las mutaciones genéticas que aumentan el riesgo de neuroblastoma a veces se heredan (se transmiten de padres a hijos). En los niños con una mutación genética, el neuroblastoma suele aparecer a una edad más temprana y se puede formar más de un tumor en las glándulas suprarrenales o en el tejido nervioso del cuello, el pecho, el abdomen o la pelvis.
El historial médico familiar no siempre permite determinar con claridad si una afección es hereditaria. Algunas familias pueden beneficiarse del asesoramiento y las pruebas genéticas. Los asesores genéticos y otros profesionales sanitarios especialmente formados para ello pueden analizar el diagnóstico del niño y el historial de salud familiar para entender los siguientes aspectos:
- Las opciones para las pruebas de los genes ALK o PHOX2B
- El riesgo de neuroblastoma para su hijo o hija y los hermanos de su hijo o hija
- Los riesgos y beneficios de conocer la información genética
Los asesores genéticos también pueden ayudar a los padres a afrontar los resultados de las pruebas genéticas de sus hijos, incluyendo cómo hablar de los resultados con el resto de la familia.
Una vez se determina que el niño tiene una forma hereditaria de neuroblastoma, otros miembros de la familia se pueden realizar exámenes de detección para la mutación en los genes ALK o PHOX2B.
Obtenga más información sobre las pruebas genéticas en Pruebas genéticas para el riesgo de cáncer hereditario .
En ocasiones, es necesario examinar a los niños con determinadas mutaciones genéticas para detectar signos de neuroblastoma.
Los niños con determinadas mutaciones genéticas o síndromes hereditarios (heredados) deben realizarse revisiones para detectar signos de neuroblastoma hasta los 10 años de edad. Se pueden utilizar las siguientes pruebas:
- Ecografía abdominal: prueba en la que se hacen rebotar ondas sonoras de alta energía (ultrasonido) en el abdomen y se generan ecos. Estos ecos forman una imagen del abdomen llamada ecografía.
- Estudios de catecolaminas en orina: prueba en la que se analiza una muestra de orina para medir las cantidades de ciertas sustancias, ácido vanililmandélico (VMA) y ácido homovanílico (HVA), que se producen cuando las catecolaminas se descomponen y se liberan en la orina. Una cantidad de VMA o HVA superior a lo normal puede ser un signo de neuroblastoma.
- Radiografía de tórax: radiografía de los órganos y huesos del interior del tórax. Un rayo X es un tipo de haz de energía que puede atravesar el cuerpo y plasmarse en una película, generando una imagen de áreas internas del cuerpo.
Hable con el médico de su hijo o hija sobre la frecuencia con la que deben realizarse estas pruebas.
Los signos y síntomas del neuroblastoma pueden ser dolor de huesos o un bulto en el abdomen, el cuello o el pecho.
Los signos y síntomas más frecuentes del neuroblastoma se deben a que el tumor presiona los tejidos cercanos a medida que crece o a que el cáncer se extiende al hueso.
Consulte con el médico si su hijo o hija presenta alguno de estos signos y síntomas:
- Un bulto en el abdomen, el cuello o el pecho
- Dolor de huesos
- Estómago hinchado y dificultad para respirar (en bebés)
- Ojos saltones
- Círculos oscuros alrededor de los ojos (ojeras)
- Bultos azulados e indoloros debajo de la piel (en bebés)
- Debilidad o parálisis (pérdida de la capacidad de mover una parte del cuerpo)
Los signos y síntomas menos comunes del neuroblastoma son:
- fever
- Dificultad para respirar
- Cansancio
- Hematomas o sangrados que aparecen con facilidad
- Petequias (manchas planas y puntiformes debajo de la piel causadas por sangrado)
- Hipertensión
- Diarrea acuosa severa
- Síndrome de Horner (párpado caído, pupila más pequeña y menos sudoración en un lado de la cara)
- Movimientos musculares espasmódicos
- Movimientos oculares incontrolados
Estos y otros signos y síntomas pueden ser causados por un neuroblastoma u otras afecciones. La única forma de saberlo es consultando al médico de su hijo o hija.
Para diagnosticar el neuroblastoma se utilizan pruebas que examinan muchos tejidos y fluidos corporales diferentes.
Si su hijo o hija presenta síntomas que sugieren un neuroblastoma, el médico deberá determinar si se deben al cáncer o a otra afección. El médico le preguntará cuándo comenzaron los síntomas y con qué frecuencia los ha tenido el niño. También le preguntará sobre el historial médico personal y familiar de su hijo o hija y le realizará un reconocimiento físico.
Según los síntomas, el historial médico y los resultados del reconocimiento físico y neurológico, el médico puede recomendar más pruebas para determinar si su hijo o hija tiene neuroblastoma y, de ser así, determinar su alcance (estadio). Si se diagnostica neuroblastoma, los resultados de estas pruebas y procedimientos le ayudarán a usted y al médico a tomar decisiones sobre el tratamiento.
Se pueden utilizar las siguientes pruebas y procedimientos:
- Estudios de catecolaminas en orina: prueba en la que se analiza una muestra de orina para medir las cantidades de ciertas sustancias, ácido vanililmandélico (VMA) y ácido homovanílico (HVA), que se producen cuando las catecolaminas se descomponen y se liberan en la orina. Una cantidad de VMA o HVA superior a lo normal puede ser un signo de neuroblastoma.
- Estudios de química sanguínea: prueba en la que se analiza una muestra de sangre para medir las cantidades de ciertas sustancias liberadas en la sangre por los órganos y tejidos del cuerpo. Una cantidad de lactato deshidrogenasa (LDH) superior a la normal puede ser un signo de enfermedad.
- Nivel de ferritina: prueba en la que se analiza una muestra de sangre para medir la cantidad de ferritina (una proteína que almacena hierro en las células). Una cantidad superior a la normal puede ser un signo de enfermedad.
- Gammagrafía con MIBG: procedimiento que se utiliza para detectar tumores neuroendocrinos, como el neuroblastoma. Se inyecta en una vena una cantidad muy pequeña de una sustancia llamada MIBG radiactiva y esta viaja a través del torrente sanguíneo. Las células de los tumores neuroendocrinos absorben la MIBG radiactiva y se detectan mediante un escáner. Las gammagrafías se pueden realizar en el transcurso de uno a tres días. Se puede administrar una solución de yodo antes o durante la prueba para evitar que la glándula tiroides absorba demasiada MIBG. Esta prueba también se utiliza para averiguar cómo está respondiendo el tumor al tratamiento. El MIBG también se utiliza en dosis altas para tratar el neuroblastoma.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye puede inyectarse en una vena o ingerirse para que los órganos o tejidos se visualicen con mayor claridad. Este procedimiento también se denomina tomografía axial computarizada. Obtenga más información sobre ello en Tomografía computarizada para el cáncer.
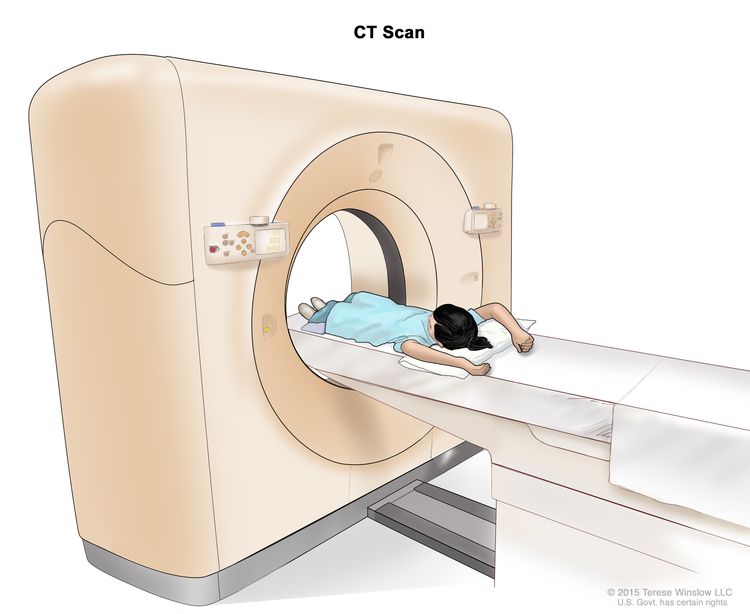
Tomografía computarizada (TC): el niño se recuesta sobre una camilla que se desliza a través del escáner, el cual toma una serie de radiografías detalladas de zonas internas del cuerpo.
- Resonancia magnética (RM) con gadolinio: procedimiento que utiliza un imán, ondas de radioy una computadora para crear una serie de imágenes detalladas de zonas internas del cuerpo. Se inyecta una sustancia llamada gadolinio en una vena. El gadolinio se acumula alrededor de las células cancerosas, haciéndolas más brillantes en la imagen. Este procedimiento también se llama imagen por resonancia magnética nuclear (IRMN).
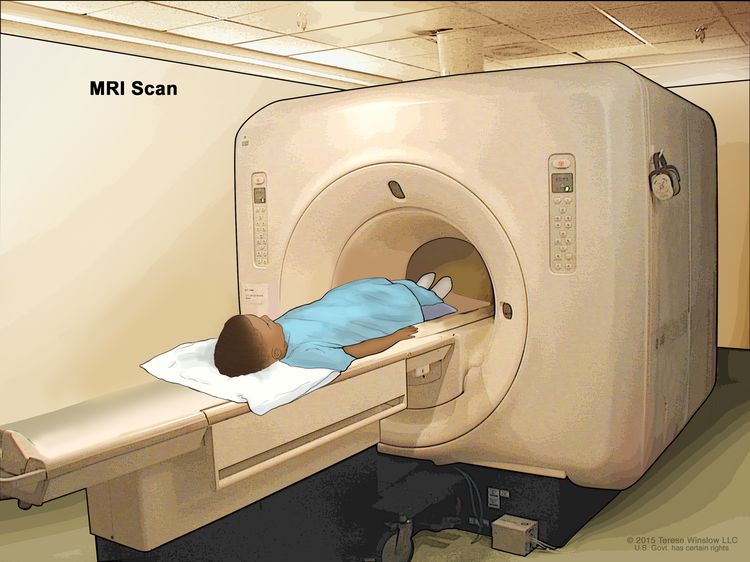
Resonancia magnética (RM): el niño se recuesta en una camilla que se desliza a través del equipo de resonancia magnética, que toma una serie de imágenes detalladas del interior del cuerpo. La posición del niño en la camilla depende de la parte del cuerpo que se va a examinar.
- Tomografía por emisión de positrones (PET): procedimiento para encontrar células tumorales malignas en el cuerpo. Se inyecta una pequeña cantidad de glucosa radiactiva (azúcar) en una vena. El escáner de la PET gira alrededor del cuerpo y genera una imagen de dónde se utiliza la glucosa en el cuerpo. Las células tumorales malignas aparecen más brillantes en la imagen porque están más activas y absorben más glucosa que las células normales. Por lo general, esta prueba solo se realizará si el tumor no absorbe MIBG.
- Radiografía de tórax o de huesos: un rayo X es un tipo de haz de energía que puede atravesar el cuerpo y plasmarse en una película, creando una imagen de zonas internas del cuerpo.
- Ecografía: procedimiento en el que ondas sonoras de alta energía (ultrasonido) rebotan en los tejidos u órganos internos y producen ecos. Estos ecos forman una imagen de los tejidos corporales llamada ecografía. No se realiza una ecografía si se ha realizado una tomografía computarizada o una resonancia magnética.
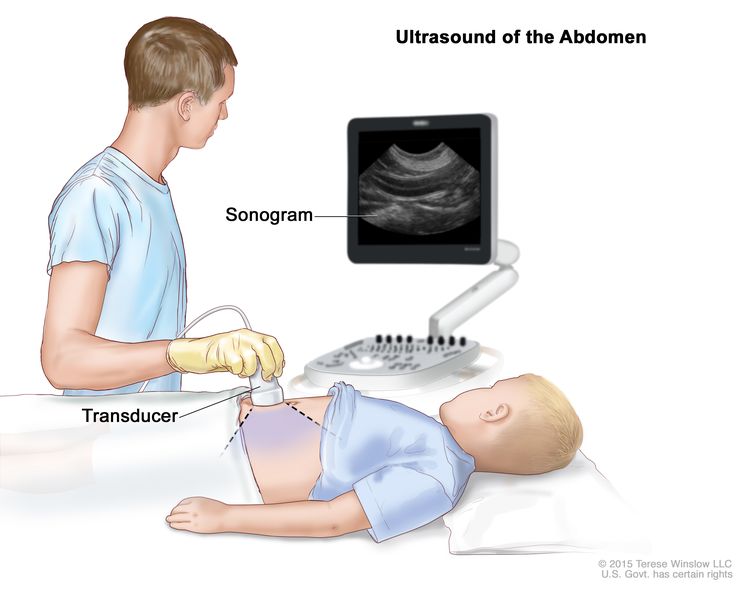
Ultrasonido abdominal: se presiona un transductor de ultrasonido conectado a una computadora contra la piel del abdomen. El transductor hace rebotar ondas de sonido en los órganos y tejidos internos para producir ecos que forman un ecograma (imagen de computadora).
- Biopsia del tumor: se toman células y tejidos durante una biopsia para que puedan ser analizados con un microscope por un pathologist y detectar así signos de cáncer. La forma en que se realiza la biopsia depende de la ubicación del tumor en el cuerpo. En ocasiones, se extirpa todo el tumor al mismo tiempo que se realiza la biopsia. El médico que revisa la biopsia del tumor determinará si este presenta características favorables o desfavorables. Estas características pueden afectar el tratamiento y la supervivencia.
Es posible que los niños de hasta 6 meses no necesiten una biopsia o cirugía para extirpar el tumor porque éste puede desaparecer sin tratamiento.
- Biopsia y aspiración de la médula ósea: consiste en la extracción de médula ósea, sangre y un pequeño fragmento de hueso mediante la inserción de una aguja hueca en el hueso de la cadera o el esternón. Un patólogo examina la médula ósea, la sangre y el hueso con un microscopio para buscar signos de cáncer. Esta prueba también se utiliza para determinar el estadio del tumor.
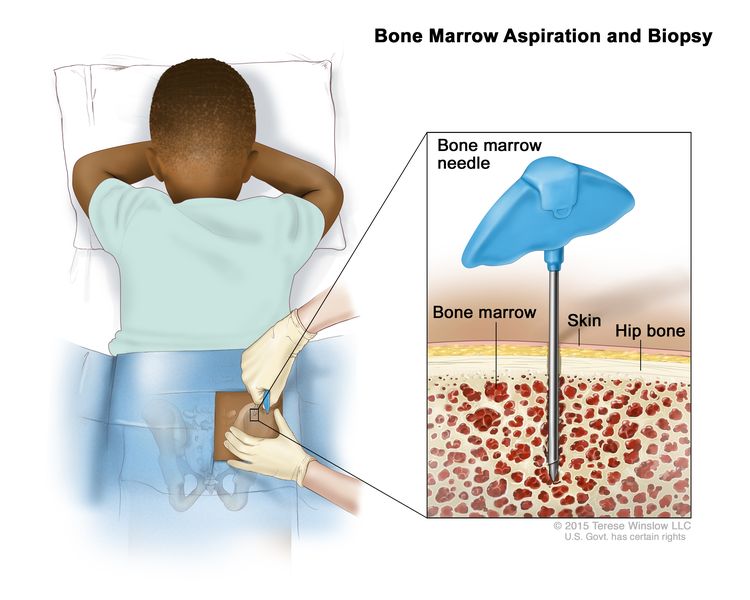
Aspiración y biopsia de médula ósea: tras anestesiar una pequeña zona de la piel, se introduce una aguja para médula ósea en el hueso de la cadera del niño. Se extraen muestras de sangre, hueso y médula ósea para examinarlas con un microscopio.
- Biopsia de ganglio linfático: extirpación total o parcial de un ganglio linfático. Un patólogo examina el tejido del ganglio linfático con el microscopio para detectar células cancerosas. Esta prueba se utiliza para diagnosticar y estadificar el tumor. Se puede realizar uno de los siguientes tipos de biopsias:
- Biopsia por escisión: extirpación de un ganglio linfático completo
- Biopsia incisional: extirpación de parte de un ganglio linfático
- Biopsia central: extracción de tejido de un ganglio linfático con una aguja ancha
- Biopsia por aspiración con aguja fina (AAF): extracción de tejido o líquido de un ganglio linfático mediante una aguja fina
- Microscopía óptica: prueba de laboratorio en la que se observan células de una muestra de tejido con microscopios normales y de alta potencia para buscar ciertos cambios en las células.
- Inmunohistoquímica: prueba de laboratorio que utiliza anticuerpos para detectar ciertos antígenos (marcadores) en una muestra de tejido de un paciente. Los anticuerpos suelen estar unidos a una enzima o un colorante fluorescente. Tras unirse a un antígeno específico en la muestra de tejido, la enzima o el colorante se activan y el antígeno puede observarse con ayuda del microscopio. Este tipo de prueba se utiliza para ayudar a diagnosticar el cáncer y a distinguir un tipo de cáncer de otro.
- Las pruebas moleculares: una prueba molecular busca ciertos genes, proteínas u otras moléculas en una muestra de tejido, sangre o médula ósea. Las pruebas moleculares también detectan ciertos cambios en un gen o cromosoma que pueden causar o afectar la probabilidad de desarrollar neuroblastoma. Se puede utilizar una prueba molecular para ayudar a planificar el tratamiento, determinar en qué medida está funcionando bien el tratamiento o hacer un pronóstico.
Los niños con neuroblastoma de riesgo alto recién diagnosticado podrían ser candidatos para realizarse pruebas moleculares a través de la Iniciativa de Caracterización Molecular.
La Iniciativa de Caracterización Molecular ofrece pruebas moleculares gratuitas a niños, adolescentes y adultos jóvenes con ciertos tipos de cáncer recién diagnosticados. El programa se imparte a través de la Iniciativa de Datos sobre Cáncer Infantil del NCI. Para más información, visite el sitio Acerca de la Iniciativa de Caracterización Molecular.
- Pruebas de biomarcadores: la prueba de biomarcadores es una forma de buscar genes, proteínas y otras sustancias (llamadas biomarcadores o marcadores tumorales) que pueden brindar información sobre el cáncer. Algunos biomarcadores afectan al comportamiento de ciertos tipos de cáncer y al funcionamiento de ciertos tratamientos. Las pruebas de biomarcadores pueden ayudar a su médico a elegir un tratamiento contra el cáncer.
Para verificar estos biomarcadores, se extraen muestras de tejido que contienen células de neuroblastoma durante una biopsia o cirugía y se analizan en un laboratorio.
Las pruebas de biomarcadores de neuroblastoma son:
- Estudio de amplificación de MYCN: estudio de laboratorio en el que se analizan las células de una muestra tumoral o de médula ósea para determinar cuántas copias del gen MYCN hay en el ADN tumoral. El MYCN es importante para el crecimiento celular. Tener más de diez copias del gen se denomina amplificación de MYCN. El neuroblastoma con amplificación de MYCN tiene mayor probabilidad de extenderse por el organismo y de crecer rápidamente.
- ALK: las células tumorales pueden analizarse en el laboratorio para detectar mutaciones o amplificación (verificación del número) del gen ALK. Estos cambios pueden aumentar el crecimiento de células cancerosas. Encontrar cambios en el gen ALK en el tejido tumoral puede llevar a cambios en el plan de tratamiento del cáncer.
- Análisis citogenético: prueba de laboratorio en la que se cuenta el número y la estructura de los cromosomas de las células de una muestra de tejido y se analizan para detectar cualquier cambio, como cromosomas rotos, faltantes, reorganizados o adicionales. Los cambios en ciertos cromosomas pueden ser un signo de cáncer. El análisis citogenético se utiliza para diagnosticar el cáncer, planificar el tratamiento o determinar su eficacia.
- Pruebas genéticas para los genes ALK o PHOX2B: prueba de laboratorio en la que se analiza una muestra de sangre o tejido para detectar un cambio en el gen ALK o en el gen PHOX2B en células normales.
Los pacientes pueden obtener una segunda opinión.
Puede que desee obtener una segunda opinión para confirmar el diagnóstico de neuroblastoma y el plan de tratamiento de su hijo o hija. Si busca una segunda opinión, deberá obtener los resultados de las pruebas médicas y los informes del primer médico para compartirlos con el segundo médico. El segundo médico revisará los resultados de las pruebas genéticas, el informe patológico, las diapositivas y las exploraciones. Este médico puede estar de acuerdo con el primer médico, sugerir cambios en el plan de tratamiento o proporcionar más información sobre el cáncer del niño.
Para obtener más información sobre cómo elegir un médico y obtener una segunda opinión, consulte Búsqueda de tratamiento para el cáncer. Puede comunicarse con el Servicio de Información de Cáncer del NCI por chat, correo electrónico o teléfono (tanto en inglés como en español) para obtener ayuda para encontrar un médico, un hospital o una segunda opinión. Si tiene alguna pregunta que desee hacer en las citas de su hijo o hija, consulte Preguntas para el médico sobre el cáncer.
Certain factors affect prognosis (chance of recovery) and treatment options.
Si a su hijo o hija le han diagnosticado neuroblastoma, es posible que tenga preguntas sobre la gravedad del cáncer y sus posibilidades de supervivencia. El pronóstico es el resultado o la evolución probable de una enfermedad.
El pronóstico y las opciones de tratamiento dependen de:
- La edad en el momento del diagnóstico
- El grupo de riesgo del niño
- Posibles cambios en los genes MYCN o ALK
- Si el tumor es diploide o hiperdiploide
- Posibles cambios en los cromosomas del tumor
- El tipo de receptor de neurotrofina tumoral
- En qué parte del cuerpo se originó el tumor (abdomen, pecho, cuello o columna)
- the stage of the cancer
- Los niveles de LDH y ferritina
- Cómo responde el tumor al tratamiento
- Cuánto tiempo pasó entre el diagnóstico y el momento en que el cáncer reapareció (en el caso de cáncer recidivante)
El pronóstico y las opciones de tratamiento del neuroblastoma también se ven afectados por la histología del tumor, lo cual comprende:
- Los patrones de las células tumorales
- En qué medida son diferentes las células tumorales de las células normales
- La rapidez con la que crecen las células tumorales
La histología tumoral se considera favorable o desfavorable según estos factores. Un niño con histología tumoral favorable tiene mayores probabilidades de recuperación.
En algunos niños de hasta 6 meses, el neuroblastoma puede desaparecer sin tratamiento. Esto se denomina regresión espontánea. Se vigila de cerca al niño para detectar signos o síntomas de neuroblastoma. Si se presentan signos o síntomas, podría ser necesario un tratamiento.
Estadios del neuroblastoma
Puntos clave
- Después de diagnosticar un neuroblastoma, se realizan pruebas para determinar si el cáncer se ha extendido desde el lugar donde se originó a otras partes del cuerpo.
- Para determinar el estadio del neuroblastoma se utiliza el Sistema Internacional de Estadificación del Grupo de Riesgo de Neuroblastoma (INRGSS).
- Estadio L1
- Estadio L2
- Estadio M
- Estadio MS
- El tratamiento del neuroblastoma se basa en los grupos de riesgo.
- A veces, el neuroblastoma no responde al tratamiento o reaparece después del tratamiento.
Después de diagnosticar un neuroblastoma, se realizan pruebas para determinar si el cáncer se ha extendido desde el lugar donde se originó a otras partes del cuerpo.
El proceso que se utiliza para determinar la extensión o propagación del cáncer se llama estadificación. La información obtenida del proceso de estadificación ayuda a determinar el estadio de la enfermedad. En el caso del neuroblastoma, el estadio de la enfermedad determina si el cáncer es de riesgo bajo, riesgo intermedio o riesgo alto. También afecta al plan de tratamiento. Los resultados de algunas pruebas y procedimientos utilizados para diagnosticar el neuroblastoma se pueden utilizar para la estadificación. Consulte la sección Información general para obtener una descripción de estas pruebas y procedimientos.
Para determinar el estadio del neuroblastoma se utiliza el Sistema Internacional de Estadificación del Grupo de Riesgo de Neuroblastoma (INRGSS).
Estadio L1
En el estadio L1, el cáncer se encuentra en una sola zona y no existen factores de riesgo definidos por imágenes (IDRF, por sus siglas en inglés). Los IDRF se encuentran en resonancias magnéticas o tomografías computarizadas realizadas durante el diagnóstico. Los IDRF se utilizan para determinar el riesgo de la cirugía y la posibilidad de extirpar completamente el tumor.
Estadio L2
En el estadio L2, el cáncer está en una zona, no se ha extendido más allá del tejido cercano y hay uno o más IDRF.
Estadio M
En el estadio M, el neuroblastoma se ha extendido a zonas alejadas del tumor. Esto no incluye el estadio MS.
Estadio MS
En el estadio MS, los niños menores de 18 meses tienen cáncer que se ha extendido a la piel, el hígado o la médula ósea.
El tratamiento del neuroblastoma se basa en los grupos de riesgo.
Para muchos tipos de cáncer, se utilizan estadios a fin de planificar el tratamiento. En el caso del neuroblastoma, el tratamiento depende del grupo de riesgo del paciente. El grupo de riesgo se determina en función de los siguientes factores:
- El estadio del cáncer
- La edad del niño en el momento del diagnóstico
- La Clasificación Patológica Internacional del Neuroblastoma (INPC) (histología tumoral)
- Si los tumores son diploides o hiperdiploides (índice de ADN).
- Si el gen del cáncer MYCN se encuentra en las células tumorales.
- Cuánto cáncer se podría eliminar mediante cirugía.
Hay tres grupos de riesgo: riesgo bajo, riesgo intermedio y riesgo alto.
- El neuroblastoma de riesgo bajo e intermedio tiene buenas posibilidades de curación.
- El neuroblastoma de riesgo alto puede ser difícil de curar.
Para obtener más información sobre la clasificación de los grupos de riesgo, consulte la sección Criterios internacionales revisados de respuesta al neuroblastoma (INRC) en Tratamiento del neuroblastoma (versión para profesionales de la salud).
A veces, el neuroblastoma no responde al tratamiento o reaparece después del tratamiento.
El neuroblastoma refractario es un tumor que no responde al tratamiento.
El neuroblastoma recurrente es un cáncer que ha reaparecido después de haber sido tratado. El tumor puede reaparecer en el lugar donde se originó o en el sistema nervioso central .
Treatment Option Overview
Puntos clave
- Existen diferentes tipos de tratamiento para niños con neuroblastoma.
- El tratamiento de los niños con neuroblastoma debe ser planificado por un equipo de médicos expertos en el tratamiento del cáncer infantil, especialmente del neuroblastoma.
- Pueden emplearse los siguientes tipos de tratamiento:
- Observation
- Cirugía
- Quimioterapia
- Radioterapia
- Quimioterapia de dosis alta y radioterapia con rescate de células madre
- Terapia con yodo 131-MIBG
- Terapia dirigida
- Otras terapias farmacológicas
- Inmunoterapia
- New types of treatment are being tested in clinical trials.
- El tratamiento del neuroblastoma provoca efectos secundarios y efectos tardíos.
- Es posible que se necesiten cuidados de seguimiento.
Existen diferentes tipos de tratamiento para niños con neuroblastoma.
Existen diferentes tipos de tratamiento para niños y adolescentes con neuroblastoma. Usted y el equipo de cáncer de su hijo o hija trabajarán juntos para decidir el tratamiento. Se considerarán muchos factores, como la salud general del niño y si el cáncer se ha diagnosticado recientemente o ha regresado.
El tratamiento de los niños con neuroblastoma debe ser planificado por un equipo de médicos expertos en el tratamiento del cáncer infantil, especialmente del neuroblastoma.
Un oncólogo pediátrico, un médico especializado en el tratamiento de niños con cáncer, supervisará el tratamiento. El oncólogo pediátrico trabaja con otros profesionales de la salud pediátrica que son expertos en el tratamiento de niños con cáncer y especializados en determinados campos de la medicina. Entre ellos pueden figurar los siguientes especialistas:
- Cirujano pediatra
- Oncólogo radioterapeuta pediátrico
- Endocrinólogo
- Neurólogo
- Neuropatólogo pediátrico
- Neurorradiólogo
- Pediatra
- Especialista en enfermería pediátrica
- Trabajador social
- Profesional de desarrollo infantil
- Psicólogo
El plan de tratamiento de su hijo o hija incluirá información sobre el cáncer, los objetivos del tratamiento, las opciones de tratamiento y los posibles efectos secundarios. Antes de comenzar el tratamiento, le resultará útil hablar con el equipo de atención médica del cáncer del niño sobre lo que puede esperar. Para obtener ayuda en cada paso del camino, consulte nuestro folleto descargable Niños con cáncer: una guía para padres.
Pueden emplearse los siguientes tipos de tratamiento:
Observation
La observación consiste en monitorear de cerca la condición de un paciente sin administrar ningún tratamiento hasta que aparezcan o cambien los signos o síntomas.
Cirugía
La cirugía se utiliza para tratar el neuroblastoma que no se ha extendido a otras partes del cuerpo. Se extirpa la mayor cantidad de tumor posible de forma segura. También se extirpan los ganglios linfáticos y se examinan para detectar signos de cáncer.
Si no se puede extirpar el tumor, se puede realizar una biopsia.
Learn more about Surgery to Treat Cancer.
Quimioterapia
La quimioterapia (también llamada quimio) utiliza medicamentos para detener el crecimiento de las células cancerosas, ya sea matándolas o impidiendo que se dividan. Cuando la quimioterapia se toma por vía oral o se inyecta en una vena o músculo, los medicamentos ingresan al torrente sanguíneo y pueden llegar a las células cancerosas de todo el cuerpo (quimioterapia sistémica).
El uso de dos o más medicamentos contra el cáncer se denomina quimioterapia combinada.
Consulte Medicamentos aprobados para el neuroblastoma para obtener más información.
Más información sobre la quimioterapia para tratar el cáncer.
Radioterapia
La radioterapia es un tratamiento contra el cáncer que utiliza rayos X de alta energía u otros tipos de radiación para matar las células cancerosas o evitar que crezcan. Existen diferentes tipos de radioterapia:
- La radioterapia externa utiliza una máquina externa al cuerpo para enviar radiación hacia la zona cancerosa. Este tratamiento se utiliza en pacientes con neuroblastoma de riesgo alto o en pacientes cuyo tumor creció durante el tratamiento con quimioterapia.
- La radioterapia interna utiliza una sustancia radiactiva sellada en agujas, semillas, cables o catéteres que se colocan directamente en el cáncer o cerca de él.
- La radioinmunoterapia es un tipo de radioterapia en la que se vincula una sustancia radiactiva a un anticuerpo monoclonal y se inyecta en el cuerpo. El anticuerpo monoclonal puede unirse a sustancias del cuerpo, incluidas las células cancerosas. La sustancia radiactiva emite una radiación que puede ayudar a matar las células cancerosas.
Más información sobre la radioterapia para tratar el cáncer.
Quimioterapia de dosis alta y radioterapia con rescate de células madre
La quimioterapia y la radioterapia en altas dosis se administran para eliminar las células cancerosas que puedan regenerarse y provocar la reaparición del cáncer. El tratamiento también destruye las células sanas, incluidas las hematopoyéticas . El rescate con células madre es un tratamiento para reemplazar las células hematopoyéticas. Las células madre (células sanguíneas inmaduras) se extraen de la sangre o la médula ósea del paciente, se congelan y se almacenan. Tras completar la quimioterapia y la radioterapia, las células madre almacenadas se descongelan y se reinfunden al paciente. Estas células madre reinfundidas se desarrollan y regeneran las células sanguíneas del cuerpo.
Terapia con yodo 131-MIBG
La terapia con yodo 131-MIBG es un tratamiento con yodo radiactivo. El yodo radiactivo se administra a través de una vía intravenosa (IV) e ingresa al torrente sanguíneo, que transporta la radiación directamente a las células tumorales. El yodo radiactivo se acumula en las células del neuroblastoma y las mata con la radiación que se desprende. La terapia con yodo 131-MIBG a veces se usa para tratar el neuroblastoma de riesgo alto que reaparece después del tratamiento inicial.
Terapia dirigida
La terapia dirigida utiliza medicamentos u otras sustancias para bloquear la acción de enzimas, proteínas u otras moléculas específicas involucradas en el crecimiento y la propagación de las células cancerosas.
- Terapia con anticuerpos monoclonales: Los anticuerpos monoclonales son sistema inmunitario fabricadas en el laboratorio para tratar numerosas enfermedades, incluido el cáncer. Como tratamiento contra el cáncer, estos anticuerpos pueden unirse a un objetivo específico en las células cancerosas u otras células que pueden ayudar a las células cancerosas a crecer. Los anticuerpos pueden entonces destruir las células cancerosas, bloquear su crecimiento o impedir su propagación. Los anticuerpos monoclonales se administran por infusión. Pueden usarse solos o para transportar fármacos, toxinaso radioactivo material directamente a las células cancerosas.
- El dinutuximab se utiliza para tratar a pacientes con neuroblastoma de riesgo alto y neuroblastoma que ha reaparecido después del tratamiento o no ha respondido al tratamiento.
- La terapia con inhibidores de la ornitina descarboxilasa retarda el crecimiento y la división de las células cancerosas.
- La eflornitina se puede administrar durante dos años después de la terapia de mantenimiento para el neuroblastoma de riesgo alto.
Obtenga más información en Terapia dirigida para tratar el cáncer.
Otras terapias farmacológicas
Otro medicamento que se usa en combinación para tratar el neuroblastoma es:
- Isotretinoína: un medicamento similar a una vitamina que reduce la capacidad del cáncer para producir más células cancerosas y modifica su apariencia y comportamiento. Este medicamento se administra por vía oral.
Inmunoterapia
La inmunoterapia ayuda al sistema inmunológico de un niño a combatir el cáncer.
- Factor estimulante de colonias de granulocitos y macrófagos (GM-CSF): una citoquina que ayuda al cuerpo a producir más glóbulos blancos, especialmente granulocitos y macrófagos, que pueden atacar y matar las células cancerosas. El GM-CSF también puede mejorar la respuesta del sistema inmunológico contra el cáncer al aumentar la cantidad de células T que combaten el cáncer.
- Terapia con células CAR-T: las células T del paciente (un tipo de célula del sistema inmunitario) se modifican para que ataquen a ciertas proteínas en la superficie de las células cancerosas. Se extraen células T del paciente y se añaden receptores especiales a su superficie en el laboratorio. Las células cambiadas se llaman (receptor de antígeno quimérico) células CAR-T. Estas células se cultivan en el laboratorio y se administran al paciente mediante infusión. Se multiplican en la sangre del paciente y atacan las células cancerosas.
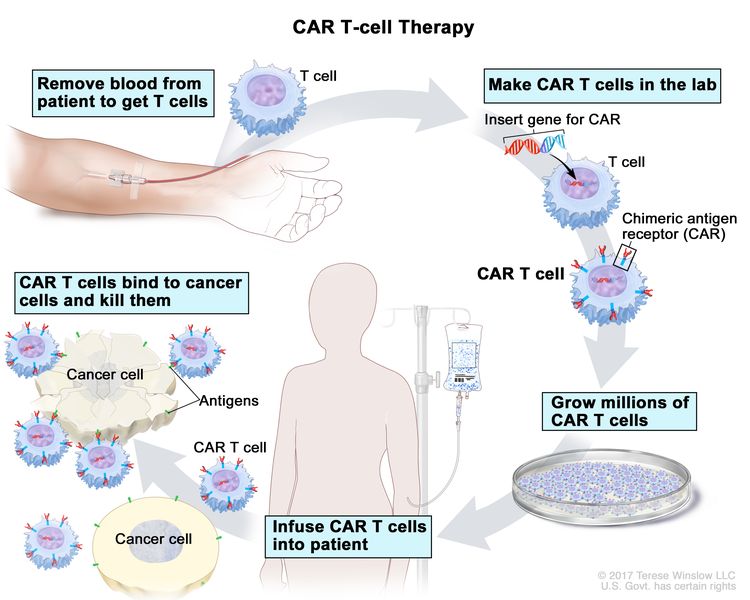
Terapia con células CAR-T: es un tratamiento en el que las células T del paciente (un tipo de célula inmunitaria) se modifican en el laboratorio para que se unan a las células cancerosas y las destruyan. La sangre del paciente fluye desde una vena del brazo a través de un tubo hacia una máquina de aféresis (no mostrada en el dibujo), que extrae los glóbulos blancos, incluidas las células T, y devuelve el resto de la sangre al paciente. En el laboratorio, se inserta un gen especial llamado receptor de antígeno quimérico (CAR) en las células T. Millones de estas células CAR-T se cultivan y se administran al paciente mediante una infusión. Una vez en el cuerpo, las células CAR-T se unen a un antígeno en las células cancerosas y las destruyen.
Se está estudiando la terapia con células CAR-T para tratar el neuroblastoma que ha reaparecido después del tratamiento o no ha respondido al tratamiento.
Más información sobre la terapia de transferencia de células T.
New types of treatment are being tested in clinical trials.
Un ensayo clínico de tratamiento es un estudio de investigación cuyo objetivo es ayudar a mejorar los tratamientos actuales u obtener información sobre nuevos tratamientos para personas con cáncer. Para algunos pacientes, participar en un ensayo clínico puede ser una opción. Debido a que el cáncer en los niños es poco frecuente, se debe considerar la posibilidad de participar en un ensayo clínico.
Utilice nuestra búsqueda de ensayos clínicos para encontrar ensayos clínicos sobre el cáncer respaldados por el NCI que estén aceptando pacientes. Puede buscar ensayos según el tipo de cáncer, la edad del paciente y dónde se realizan los ensayos. Algunos ensayos clínicos están abiertos sólo a pacientes que no han iniciado el tratamiento. Los ensayos clínicos respaldados por otras organizaciones se pueden encontrar en el sitio web ClinicalTrials.gov.
Para obtener más información, consulte la sección Información sobre ensayos clínicos para pacientes y cuidadores .
El tratamiento del neuroblastoma provoca efectos secundarios y efectos tardíos.
Para obtener más información sobre los efectos secundarios que aparecen durante el tratamiento del cáncer, consulte la sección Efectos secundarios.
Los efectos secundarios del tratamiento del cáncer que comienzan después del tratamiento y continúan durante meses o años se denominan efectos tardíos. A continuación, se mencionan algunos efectos tardíos del tratamiento del cáncer:
- Problemas físicos, como los siguientes:
- Desarrollo dental
- Obstrucción intestinal
- Crecimiento de huesos y cartílagos
- Función auditiva
- Síndrome metabólico (presión arterial elevada, triglicéridos elevados, colesterol elevado, aumento del porcentaje de grasa corporal)
- Cambios en el estado de ánimo, los sentimientos, los pensamientos, el aprendizaje o la memoria
- Segundos cánceres (nuevos tipos de cáncer), como el síndrome mielodisplásico, la leucemia mieloide aguda, el cáncer de tiroides o el cáncer de riñón
Algunos efectos tardíos pueden tratarse o controlarse. Es importante hablar con los pediatras sobre los efectos que el tratamiento del cáncer puede tener en su hijo o hija. Para obtener más información, consulte Efectos tardíos del tratamiento anticanceroso en la niñez.
Es posible que se necesiten cuidados de seguimiento.
Durante el tratamiento, su hijo/a se someterá a pruebas o revisiones de seguimiento. Algunas pruebas realizadas para diagnosticar o estadificar el cáncer podrían repetirse para evaluar la eficacia del tratamiento. Las decisiones sobre si continuar, modificar o suspender el tratamiento podrían basarse en los resultados de estas pruebas.
Algunas de las pruebas se seguirán realizando periódicamente después de que finalice el tratamiento. Los resultados de estas pruebas pueden mostrar si la afección de su hijo o hija ha cambiado o si el cáncer ha recidivado (regresado).
Los cuidados de seguimiento para niños con neuroblastoma pueden incluir:
- Estudios de catecolaminas en orina
- Exploración con MIBG
Tratamiento del neuroblastoma de riesgo bajo
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento del neuroblastoma de riesgo bajo recién diagnosticado puede incluir:
- Cirugía seguida de observación
- Observación sola para bebés menores de 6 meses que tienen tumores suprarrenales pequeños o para bebés que no presentan signos ni síntomas de neuroblastoma.
- Observación con biopsia para bebés menores de 1 año que tienen histología favorable y cumplen otros criterios de riesgo bajo.
- Quimioterapia con o sin cirugía, para niños con síntomas o niños cuyo tumor ha seguido creciendo y no se puede extirpar mediante cirugía.
- Quimioterapia en el caso de ciertos pacientes
- Radioterapia para tratar tumores que causan problemas graves y no responden rápidamente a la quimioterapia o la cirugía.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del neuroblastoma de riesgo intermedio
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento del neuroblastoma de riesgo intermedio recién diagnosticado puede incluir:
- Quimioterapia para niños con síntomas o para reducir un tumor que no se puede extirpar mediante cirugía. La cirugía se puede realizar después de la quimioterapia.
- Cirugía sola en el caso de los bebés
- Observación sola en el caso de los lactantes
- Radioterapia para tratar tumores que han seguido creciendo durante el tratamiento con quimioterapia o tumores que no se pueden extirpar mediante cirugía y han continuado creciendo después del tratamiento con quimioterapia
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del neuroblastoma de riesgo alto
For information about the treatments listed below, see the Treatment Option Overview section.
Los niños con neuroblastoma de riesgo alto recién diagnosticado generalmente reciben tratamiento en tres fases: inducción, consolidación y mantenimiento.
El tratamiento durante la inducción puede incluir:
- Quimioterapia combinada
- Cirugía
El tratamiento durante la consolidación puede incluir:
- Dos ciclos de quimioterapia combinada en dosis altas seguidos de rescate de células madre
- Radioterapia
El tratamiento durante el mantenimiento puede incluir terapia con anticuerpos monoclonales (dinutuximab), factor estimulante de colonias de granulocitos y macrófagos (GM-CSF) e isotretinoína.
El tratamiento después del mantenimiento puede incluir eflornitina.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del neuroblastoma en estadio MS
For information about the treatments listed below, see the Treatment Option Overview section.
No existe un tratamiento estándar para el neuroblastoma recién diagnosticado en estadio MS, pero el tratamiento incluye las siguientes opciones:
- Observación y cuidados médicos de apoyo para niños que tienen una biología tumoral favorable y no presentan signos ni síntomas.
- Quimioterapia para niños que presentan signos o síntomas, para bebés muy pequeños o para niños con una biología tumoral desfavorable.
- Radioterapia para niños con neuroblastoma que se ha extendido al hígado.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del neuroblastoma recidivante
For information about the treatments listed below, see the Treatment Option Overview section.
Pacientes que recibieron tratamiento anterior por neuroblastoma de riesgo bajo
El tratamiento del neuroblastoma recidivante que reaparece en la zona donde se formó por primera vez puede consistir en:
- Cirugía seguida de observación o quimioterapia
- Quimioterapia que puede ir seguida de cirugía.
El tratamiento para el neuroblastoma recidivante que reaparece en otras partes del cuerpo o que no ha respondido al tratamiento puede consistir en:
- Observación
- Quimioterapia
- Cirugía seguida de quimioterapia
- Tratamiento similar al del neuroblastoma de riesgo alto recién diagnosticado, en el caso de niños mayores de 18 meses
Pacientes que recibieron tratamiento anterior por neuroblastoma de riesgo intermedio
El tratamiento del neuroblastoma recidivante que reaparece en la zona donde se formó por primera vez puede consistir en:
- Cirugía que puede ir seguida de quimioterapia.
- Radioterapia para niños cuya enfermedad ha empeorado después de la quimioterapia y la cirugía de revisión.
El tratamiento para el neuroblastoma recidivante que reaparece en otras partes del cuerpo puede incluir:
- Tratamiento similar al del neuroblastoma de riesgo alto recién diagnosticado
Pacientes que recibieron un tratamiento anterior por neuroblastoma de riesgo alto
No existe un tratamiento estándar para el neuroblastoma recidivante en pacientes que recibieron tratamiento anterior para un neuroblastoma de riesgo alto. El tratamiento puede consistir en:
- Quimioterapia combinada con terapia con anticuerpo monoclonal (dinutuximab)
- Terapia con yodo 131-MIBG para aliviar los síntomas y mejorar la calidad de vida. Puede administrarse sola o en combinación con quimioterapia, o seguida de un rescate de células madre.
- Quimioterapia.
- Un ensayo clínico de terapia con células CAR T
Dado que no existe un tratamiento estándar, los pacientes que reciben tratamiento inicial para un neuroblastoma de riesgo alto podrían valorar la posibilidad de participar en un ensayo clínico. Más información sobre ensayos clínicos en Información sobre ensayos clínicos para pacientes y cuidadores.
Pacientes con neuroblastoma recidivante en el sistema nervioso central
El tratamiento para el neuroblastoma que recidiva (regresa) en el sistema nervioso central (SNC; encéfalo y médula espinal) puede consistir en:
- Cirugía para extirpar el tumor en el SNC seguida de radioterapia
- Quimioterapia, cirugía y radioterapia
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Más información sobre el neuroblastoma
Para obtener más información del National Cancer Institute sobre el neuroblastoma, consulte los siguientes enlaces:
- Página de inicio del neuroblastoma
- Exámenes de detección del neuroblastoma
- Tomografía computarizada para el cáncer
- Medicamentos aprobados para el neuroblastoma
- Terapia dirigida para tratar el cáncer
- Immunotherapy to Treat Cancer
- Nuevos enfoques para la terapia del neuroblastoma (NANT)
Para obtener más información sobre el cáncer infantil y otros recursos generales sobre el cáncer, consulte los siguientes sitios web:
- El cáncer
- Cánceres infantiles
- CureSearch para el cáncer infantil
- Efectos tardíos del tratamiento del cáncer infantil
- Adolescentes y adultos jóvenes con cáncer
- Niños con cáncer: una guía para padres
- El cáncer en los niños y los adolescentes
- Estadificación del cáncer
- Cómo hacer frente al cáncer
- Preguntas para el médico sobre el cáncer
- Para supervivientes, cuidadores e intercesores
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen del PDQ sobre el cáncer contiene información actualizada del tratamiento del neuroblastoma. El propósito es informar y ayudar a los pacientes, sus familiares y cuidadores. No da pautas ni recomendaciones formales para tomar decisiones relacionadas con la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
La información de este resumen para pacientes procede de la versión para profesionales de la salud, la cual es revisada y actualizada periódicamente por el comité editorial del PDQ sobre el tratamiento pediátrico según sea necesario.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre el tratamiento pediátrico. Tratamiento del neuroblastoma (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Actualizado:
URL de origen: https://www.cancer.gov/node/5031/syndication
Agencia de origen: National Cancer Institute (NCI)
Fecha de captura: 2013-09-14 09:02:35.0