








Neuroblastoma
Look to the skilled oncologists at Montefiore Einstein Comprehensive Cancer Center to expertly diagnose and treat Neuroblastoma. Benefit from the most advanced treatments and well-rounded support services for you and your loved ones.

Video could not be played
Cancer Clinical Trials
- Blood & Bone Marrow Cancers
- Brain, Spine & Central Nervous System Cancers
- Breast Cancer
- Childhood Cancers
- Endocrine System Cancers
- Gastrointestinal (GI) Cancers
- Genitourinary (GU) & Urologic Cancers
- Gynecologic Cancers
- Head & Neck Cancers
- Kaposi Sarcoma & AIDS-Related Cancers
- Lung & Chest Cancers
- Prostate Cancer
- Sarcomas
- Skin Cancer
As an NCI-designated comprehensive cancer center, Montefiore Einstein Comprehensive Cancer Center supports the mission and guidelines of the National Cancer Institute (NCI). The following information about types of cancer, prevention and treatments is provided by the NCI.
Neuroblastoma Treatment (PDQ®)–Patient Version
General Information About Neuroblastoma
Key Points
- Neuroblastoma is a type of cancer that forms in neuroblasts (immature nerve tissue) in the adrenal glands, neck, chest, or spinal cord.
- Certain genetic conditions affect the risk of having neuroblastoma.
- Genetic testing can determine whether a child has an inherited form of neuroblastoma.
- Sometimes children with certain gene mutations should be checked for signs of neuroblastoma.
- Signs and symptoms of neuroblastoma include bone pain or a lump in the abdomen, neck, or chest.
- Tests that examine many different body tissues and fluids are used to diagnose neuroblastoma.
- Getting a second opinion.
- Certain factors affect prognosis (chance of recovery) and treatment options.
Neuroblastoma is a type of cancer that forms in neuroblasts (immature nerve tissue) in the adrenal glands, neck, chest, or spinal cord.
Neuroblastoma often begins in the nerve tissue of the adrenal glands. There are two adrenal glands, one on top of each kidney in the back of the upper abdomen. The adrenal glands make important hormones that help control heart rate, blood pressure, blood sugar, and the way the body reacts to stress.
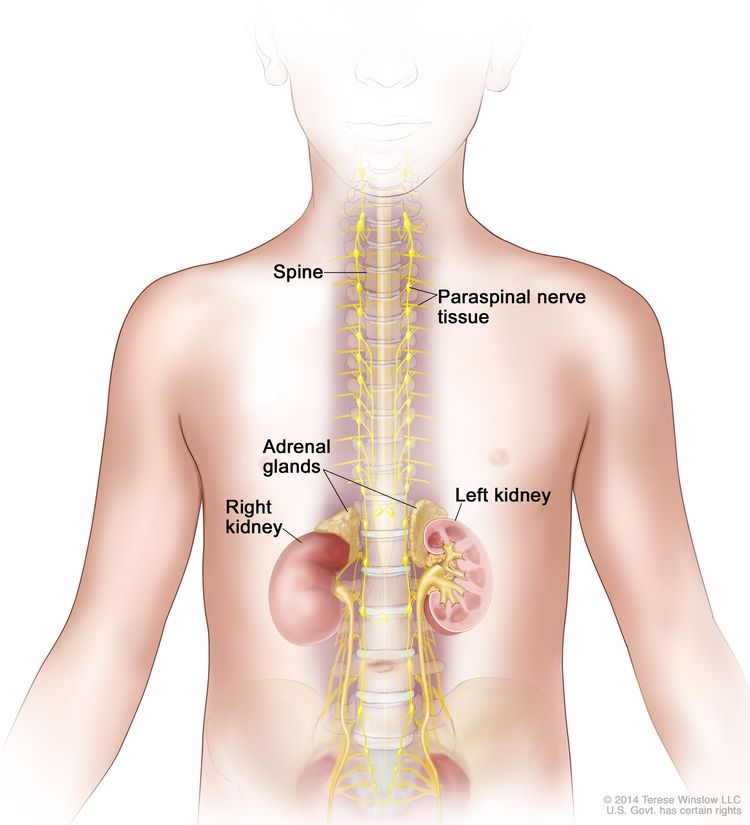
Neuroblastoma may be found in the adrenal glands and paraspinal nerve tissue from the neck to the pelvis.
Neuroblastoma most often begins in infancy. It is usually diagnosed between the first month of life and age 5 years. The tumor is found when it begins to grow and cause signs or symptoms. Sometimes it forms before birth and is found during an ultrasound of the baby.
By the time cancer is diagnosed, it has usually metastasized (spread). Neuroblastoma spreads most often to the lymph nodes, bones, bone marrow, liver, and skin in infants and children. Adolescents may also have metastasis to the lungs and brain.
Certain genetic conditions affect the risk of having neuroblastoma.
Neuroblastoma is caused by certain changes to the way neuroblast cells function, especially how they grow and divide into new cells. There are many risk factors for neuroblastoma, but many do not directly cause cancer. Instead, they increase the chance of DNA damage in cells that may lead to neuroblastoma. Learn more about how cancer develops at What Is Cancer?
A risk factor is anything that increases the chance of getting a disease. Some risk factors can be changed. Risk factors also include things people cannot change, like family history. It's important to learn about risk factors for neuroblastoma because it can help you make choices about screening for cancer.
Possible risk factors for neuroblastoma include:
- having certain changes in genes (ALK or PHOX2B)
- having certain genetic conditions, such as:
- Costello syndrome
- Noonan syndrome
- neurofibromatosis type 1
- Li-Fraumeni syndrome
- Beckwith-Wiedemann syndrome
- pheochromocytoma/paraganglioma syndromes
- ROHHAD syndromes (rapid-onset obesity, hypothalamic dysfunction, hypoventilation, and autonomic dysfunction)
- having a strong family history of neuroblastoma
Genetic testing can determine whether a child has an inherited form of neuroblastoma.
Gene mutations that increase the risk of neuroblastoma are sometimes inherited (passed from the parent to the child). In children with a gene mutation, neuroblastoma usually occurs at a younger age, and more than one tumor may form in the adrenal glands or in the nerve tissue in the neck, chest, abdomen, or pelvis.
It is not always clear from the family medical history whether a condition is inherited. Certain families may benefit from genetic counseling and genetic testing. Genetic counselors and other specially trained health professionals can discuss a child's diagnosis and the family's medical history to understand:
- the options for ALK or PHOX2B gene testing
- the risk of neuroblastoma for your child and your child's siblings
- the risks and benefits of learning genetic information
Genetic counselors can also help parents cope with their child's genetic testing results, including how to discuss the results with family members.
Once it is known that your child has an inherited form of neuroblastoma, other family members can be screened for the ALK or PHOX2B mutation.
Learn more about genetic testing at Genetic Testing for Inherited Cancer Risk.
Sometimes children with certain gene mutations should be checked for signs of neuroblastoma.
Children with certain gene mutations or hereditary (inherited) syndromes should be checked for signs of neuroblastoma until they are 10 years old. The following tests may be used:
- Abdominal ultrasound: A test in which high-energy sound waves (ultrasound) are bounced off the abdomen and make echoes. The echoes form a picture of the abdomen called a sonogram.
- Urine catecholamine studies: A test in which a urine sample is checked to measure the amounts of certain substances, vanillylmandelic acid (VMA) and homovanillic acid (HVA), that are made when catecholamines break down and are released into the urine. A higher-than-normal amount of VMA or HVA can be a sign of neuroblastoma.
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
Talk to your child's doctor about how often these tests need to be done.
Signs and symptoms of neuroblastoma include bone pain or a lump in the abdomen, neck, or chest.
The most common signs and symptoms of neuroblastoma are caused by the tumor pressing on nearby tissues as it grows or by cancer spreading to the bone.
Check with your child's doctor if your child has:
- a lump in the abdomen, neck, or chest
- bone pain
- a swollen stomach and trouble breathing (in infants)
- bulging eyes
- dark circles around the eyes ("black eyes")
- painless, bluish lumps under the skin (in infants)
- weakness or paralysis (loss of ability to move a body part)
Less common signs and symptoms of neuroblastoma include:
- fever
- shortness of breath
- feeling tired
- easy bruising or bleeding
- petechiae (flat, pinpoint spots under the skin caused by bleeding)
- high blood pressure
- severe watery diarrhea
- Horner syndrome (droopy eyelid, smaller pupil, and less sweating on one side of the face)
- jerky muscle movements
- uncontrolled eye movements
These and other signs and symptoms may be caused by neuroblastoma or by other conditions. The only way to know is to see your child's doctor.
Tests that examine many different body tissues and fluids are used to diagnose neuroblastoma.
If your child has symptoms that suggest neuroblastoma, the doctor will need to find out if these are due to cancer or another condition. The doctor will ask when the symptoms started and how often your child has been having them. They will also ask about your child's personal and family medical history and do a physical exam.
Depending on your child's symptoms and medical history and the results of their physical and neurological exam, the doctor may recommend more tests to find out if your child has neuroblastoma, and if so, its extent (stage). If neuroblastoma is diagnosed, the results of these tests and procedures will help you and your child's doctor make decisions about treatment.
The following tests and procedures may be used:
- Urine catecholamine studies: A test in which a urine sample is checked to measure the amounts of certain substances, vanillylmandelic acid (VMA) and homovanillic acid (HVA), that are made when catecholamines break down and are released into the urine. A higher-than-normal amount of VMA or HVA can be a sign of neuroblastoma.
- Blood chemistry studies: A test in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. A higher-than-normal amount of lactate dehydrogenase (LDH) can be a sign of disease.
- Ferritin level: A test in which a blood sample is checked to measure the amount of ferritin (a protein that stores iron in cells). A higher-than-normal amount may be a sign of disease.
- MIBG scan: A procedure used to find neuroendocrine tumors, such as neuroblastoma. A very small amount of a substance called radioactive MIBG is injected into a vein and travels through the bloodstream. Neuroendocrine tumor cells take up the radioactive MIBG and are detected by a scanner. Scans may be taken over 1–3 days. An iodine solution may be given before or during the test to keep the thyroid gland from absorbing too much of the MIBG. This test is also used to find out how well the tumor is responding to treatment. MIBG is also used in high doses to treat neuroblastoma.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography. Learn more about Computed Tomography (CT) Scans and Cancer.
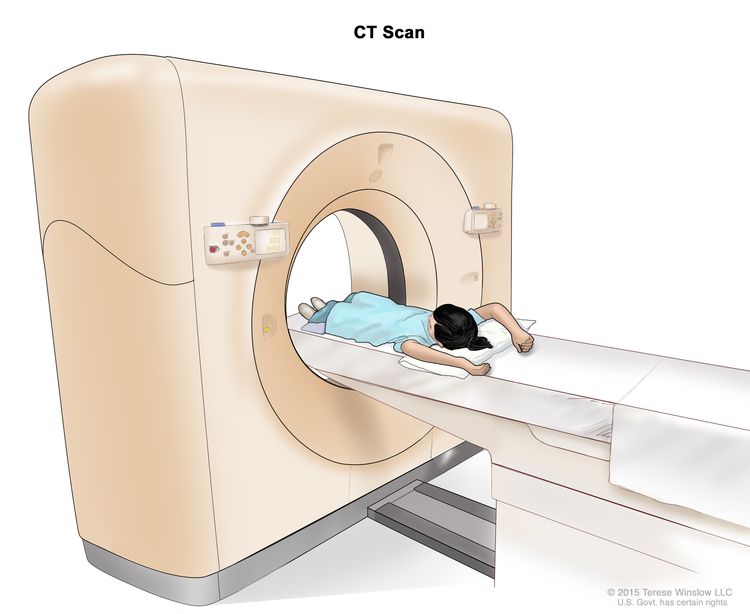
Computed tomography (CT) scan. The child lies on a table that slides through the CT scanner, which takes a series of detailed x-ray pictures of areas inside the body.
- MRI (magnetic resonance imaging) with gadolinium: A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. A substance called gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
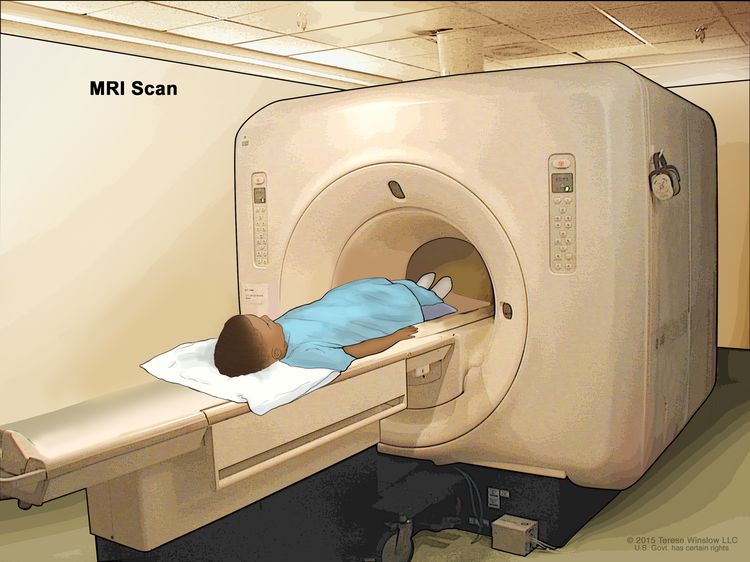
Magnetic resonance imaging (MRI) scan. The child lies on a table that slides into the MRI machine, which takes a series of detailed pictures of areas inside the body. The positioning of the child on the table depends on the part of the body being imaged.
- PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do. This test will usually only be done if the tumor does not take up MIBG.
- X-ray of the chest or bone: An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram. An ultrasound exam is not done if a CT/MRI has been done.
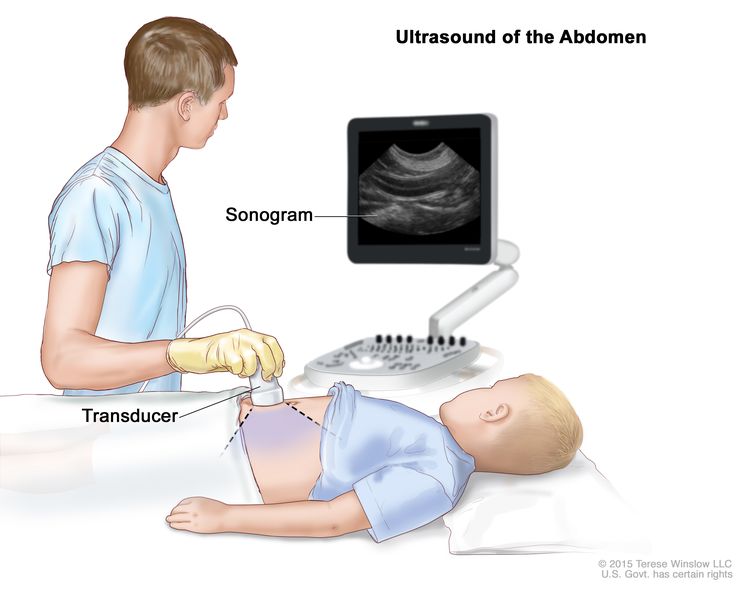
Abdominal ultrasound. An ultrasound transducer connected to a computer is pressed against the skin of the abdomen. The transducer bounces sound waves off internal organs and tissues to make echoes that form a sonogram (computer picture).
- Tumor biopsy: Cells and tissues are removed during a biopsy so they can be viewed under a microscope by a pathologist to check for signs of cancer. The way the biopsy is done depends on where the tumor is in the body. Sometimes the whole tumor is removed at the same time the biopsy is done. The doctor who reviews the tumor biopsy will determine if the tumor appears to have more favorable or unfavorable features. These features may affect treatment and survival.
Children up to age 6 months may not need a biopsy or surgery to remove the tumor because the tumor may disappear without treatment.
- Bone marrow aspiration and biopsy: The removal of bone marrow, blood, and a small piece of bone by inserting a hollow needle into the hipbone or breastbone. A pathologist views the bone marrow, blood, and bone under a microscope to look for signs of cancer. This test is also used to stage the tumor.
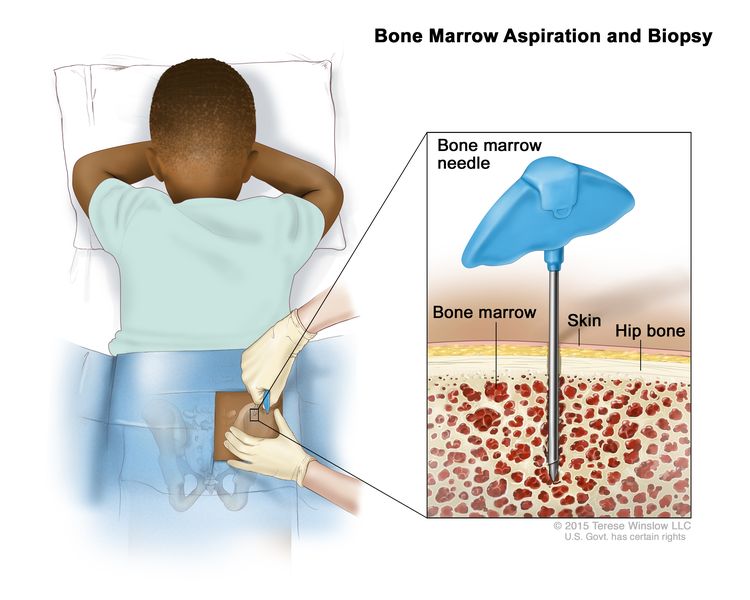
Bone marrow aspiration and biopsy. After a small area of skin is numbed, a bone marrow needle is inserted into the child’s hip bone. Samples of blood, bone, and bone marrow are removed for examination under a microscope.
- Lymph node biopsy: The removal of all or part of a lymph node. A pathologist views the lymph node tissue under a microscope to check for cancer cells. This test is used to diagnose and stage the tumor. One of the following types of biopsies may be done:
- Excisional biopsy: The removal of an entire lymph node.
- Incisional biopsy: The removal of part of a lymph node.
- Core biopsy: The removal of tissue from a lymph node using a wide needle.
- Fine-needle aspiration (FNA) biopsy: The removal of tissue or fluid from a lymph node using a thin needle.
- Light microscopy: A laboratory test in which cells in a sample of tissue are viewed under regular and high-powered microscopes to look for certain changes in the cells.
- Immunohistochemistry: A laboratory test that uses antibodies to check for certain antigens (markers) in a sample of a patient’s tissue. The antibodies are usually linked to an enzyme or a fluorescent dye. After the antibodies bind to a specific antigen in the tissue sample, the enzyme or dye is activated, and the antigen can then be seen under a microscope. This type of test is used to help diagnose cancer and to help tell one type of cancer from another type of cancer.
- Molecular testing: A molecular test checks for certain genes, proteins, or other molecules in a sample of tissue, blood, or bone marrow. Molecular tests also check for certain changes in a gene or chromosome that may cause or affect the chance of developing neuroblastoma. A molecular test may be used to help plan treatment, find out how well treatment is working, or make a prognosis.
Children with newly diagnosed high-risk neuroblastoma may be eligible for molecular testing through the Molecular Characterization Initiative.
The Molecular Characterization Initiative offers free molecular testing to children, adolescents, and young adults with certain types of newly diagnosed cancer. The program is offered through NCI's Childhood Cancer Data Initiative. To learn more, visit About the Molecular Characterization Initiative.
- Biomarker testing: Biomarker testing is a way to look for genes, proteins, and other substances (called biomarkers or tumor markers) that can provide information about cancer. Some biomarkers affect how certain cancers behave and how certain treatments work. Biomarker testing may help your doctor choose a cancer treatment.
To check for these biomarkers, samples of tissue containing neuroblastoma cells are removed during a biopsy or surgery and tested in a laboratory.
Neuroblastoma biomarker testing includes:
- MYCN amplification study: A laboratory study in which cells in a sample of tumor or bone marrow are checked to see how many copies of the MYCN gene are in the tumor DNA. MYCN is important for cell growth. Having more than 10 copies of the gene is called MYCN amplification. Neuroblastoma with MYCN amplification is more likely to spread in the body and more likely to show rapid growth.
- ALK: The tumor cells may be checked in the laboratory for mutations or amplification (checking the number) of the ALK gene. These changes may increase the growth of cancer cells. Finding changes in the ALK gene in tumor tissue may lead to changes in the cancer treatment plan.
- Cytogenetic analysis: A laboratory test in which the number and structure of chromosomes of cells in a sample of tissue are counted and checked for any changes, such as broken, missing, rearranged, or extra chromosomes. Changes in certain chromosomes may be a sign of cancer. Cytogenetic analysis is used to help diagnose cancer, plan treatment, or find out how well treatment is working.
- ALK or PHOX2B genetic tests: A laboratory test in which a sample of blood or tissue is tested for a change in the ALK gene or PHOX2B gene in normal cells.
Getting a second opinion.
You may want to get a second opinion to confirm their child's neuroblastoma diagnosis and treatment plan. If you seek a second opinion, you will need to get medical test results and reports from the first doctor to share with the second doctor. The second doctor will review the genetic test results, pathology report, slides, and scans. This doctor may agree with the first doctor, suggest changes to the treatment plan, or provide more information about your child's cancer.
To learn more about choosing a doctor and getting a second opinion, see Finding Cancer Care. You can contact NCI's Cancer Information Service via chat, email, or phone (both in English and Spanish) for help finding a doctor or hospital that can provide a second opinion. For questions you might want to ask at your child's appointments, see Questions to Ask Your Doctor About Cancer.
Certain factors affect prognosis (chance of recovery) and treatment options.
If your child has been diagnosed with neuroblastoma, you may have questions about how serious the cancer is and your child's chances of survival. The likely outcome or course of a disease is called prognosis.
The prognosis and treatment options depend on:
- age at the time of diagnosis
- the child's risk group
- whether there are certain changes in the MYCN or ALK genes
- whether the tumor is diploid or hyperdiploid
- whether there are changes to the tumor chromosomes
- the type of tumor neurotrophin receptor
- where in the body the tumor started (abdomen, chest, neck, or spine)
- the stage of the cancer
- levels of LDH and ferritin
- how the tumor responds to treatment
- how much time passed between diagnosis and when the cancer recurred (for recurrent cancer)
Prognosis and treatment options for neuroblastoma are also affected by tumor histology, which includes:
- the patterns of the tumor cells
- how different the tumor cells are from normal cells
- how fast the tumor cells are growing
The tumor histology is said to be favorable or unfavorable, depending on these factors. A child with favorable tumor histology has a better chance of recovery.
In some children up to age 6 months, neuroblastoma may disappear without treatment. This is called spontaneous regression. The child is closely watched for signs or symptoms of neuroblastoma. If signs or symptoms occur, treatment may be needed.
Stages of Neuroblastoma
Key Points
- After neuroblastoma has been diagnosed, tests are done to find out if cancer has spread from where it started to other parts of the body.
- The International Neuroblastoma Risk Group Staging System (INRGSS) is used to determine the stage of neuroblastoma.
- Stage L1
- Stage L2
- Stage M
- Stage MS
- Treatment of neuroblastoma is based on risk groups.
- Sometimes neuroblastoma does not respond to treatment or comes back after treatment.
After neuroblastoma has been diagnosed, tests are done to find out if cancer has spread from where it started to other parts of the body.
The process used to find out the extent or spread of cancer is called staging. The information gathered from the staging process helps determine the stage of the disease. For neuroblastoma, the stage of disease affects whether the cancer is low risk, intermediate risk, or high risk. It also affects the treatment plan. The results of some tests and procedures used to diagnose neuroblastoma may be used for staging. See the General Information section for a description of these tests and procedures.
The International Neuroblastoma Risk Group Staging System (INRGSS) is used to determine the stage of neuroblastoma.
Stage L1
In stage L1, the cancer is in only one area, and there are no image-defined risk factors (IDRFs). IDRFs are found on MRI or CT scans done during diagnosis. IDRFs are used to determine the risk of surgery and the chance of completely removing the tumor.
Stage L2
In stage L2, the cancer is in one area, has not spread beyond nearby tissue, and there are one or more IDRFs.
Stage M
In stage M, neuroblastoma has spread to areas far from the tumor. This does not include stage MS.
Stage MS
In stage MS, children younger than 18 months have cancer that has spread to the skin, liver, or bone marrow.
Treatment of neuroblastoma is based on risk groups.
For many types of cancer, stages are used to plan treatment. For neuroblastoma, treatment depends on the patient's risk group. The risk group is determined by the following factors:
- the stage of the cancer
- the child's age at diagnosis
- the International Neuroblastoma Pathologic Classification (INPC) (tumor histology)
- whether the tumors are diploid or hyperdiploid (DNA index)
- whether the cancer gene MYCN is found in the tumor cells
- how much of the cancer could be removed by surgery
There are three risk groups: low risk, intermediate risk, and high risk.
- Low-risk and intermediate-risk neuroblastoma have a good chance of being cured.
- High-risk neuroblastoma may be hard to cure.
For more information on the risk group classification, see the Revised International Neuroblastoma Response Criteria (INRC) section in Neuroblastoma Treatment (Health Professional Version).
Sometimes neuroblastoma does not respond to treatment or comes back after treatment.
Refractory neuroblastoma is a tumor that does not respond to treatment.
Recurrent neuroblastoma is cancer that has recurred (come back) after it has been treated. The tumor may come back in the site where it began or in the central nervous system.
Treatment Option Overview
Key Points
- There are different types of treatment for children with neuroblastoma.
- Children with neuroblastoma should have their treatment planned by a team of doctors who are experts in treating childhood cancer, especially neuroblastoma.
- The following types of treatment may be used:
- Observation
- Surgery
- Chemotherapy
- Radiation therapy
- High-dose chemotherapy and radiation therapy with stem cell rescue
- Iodine 131-MIBG therapy
- Targeted therapy
- Other drug therapy
- Immunotherapy
- New types of treatment are being tested in clinical trials.
- Treatment for neuroblastoma causes side effects and late effects.
- Follow-up care may be needed.
There are different types of treatment for children with neuroblastoma.
There are different types of treatment for children and adolescents with neuroblastoma. You and your child's cancer team will work together to decide treatment. Many factors will be considered, such as your child's overall health and whether the cancer is newly diagnosed or has come back.
Children with neuroblastoma should have their treatment planned by a team of doctors who are experts in treating childhood cancer, especially neuroblastoma.
A pediatric oncologist, a doctor who specializes in treating children with cancer, will oversee treatment. The pediatric oncologist works with other pediatric health care professionals who are experts in treating children with cancer and who specialize in certain areas of medicine. These may include the following specialists and others:
- pediatric surgeon
- pediatric radiation oncologist
- endocrinologist
- neurologist
- pediatric neuropathologist
- neuroradiologist
- pediatrician
- pediatric nurse specialist
- social worker
- child life professional
- psychologist
Your child's treatment plan will include information about the cancer, the goals of treatment, treatment options, and the possible side effects. It will be helpful to talk with your child's cancer care team before treatment begins about what to expect. For help every step of the way, see our downloadable booklet, Children with Cancer: A Guide for Parents.
The following types of treatment may be used:
Observation
Observation is closely monitoring a patient's condition without giving any treatment until signs or symptoms appear or change.
Surgery
Surgery is used to treat neuroblastoma that has not spread to other parts of the body. As much of the tumor as is safely possible is removed. Lymph nodes are also removed and checked for signs of cancer.
If the tumor cannot be removed, a biopsy may be done instead.
Learn more about Surgery to Treat Cancer.
Chemotherapy
Chemotherapy (also called chemo) uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy).
The use of two or more anticancer drugs is called combination chemotherapy.
See Drugs Approved for Neuroblastoma for more information.
Learn more about Chemotherapy to Treat Cancer.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are different types of radiation therapy:
- External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer. This treatment is used for patients with high-risk neuroblastoma or for patients whose tumor grew while being treated with chemotherapy.
- Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer.
- Radioimmunotherapy is a type of radiation therapy in which a radioactive substance is linked to a monoclonal antibody and injected into the body. The monoclonal antibody can bind to substances in the body, including cancer cells. The radioactive substance gives off radiation, which may help kill cancer cells.
Learn more about Radiation Therapy to Treat Cancer.
High-dose chemotherapy and radiation therapy with stem cell rescue
High-dose chemotherapy and radiation therapy are given to kill any cancer cells that may regrow and cause the cancer to come back. Healthy cells, including blood-forming cells, are also destroyed by the cancer treatment. Stem cell rescue is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient and are frozen and stored. After the completion of chemotherapy and radiation therapy, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
Iodine 131-MIBG therapy
Iodine 131-MIBG therapy is a treatment with radioactive iodine. The radioactive iodine is given through an intravenous (IV) line and enters the bloodstream, which carries radiation directly to tumor cells. Radioactive iodine collects in neuroblastoma cells and kills them with the radiation that is given off. Iodine 131-MIBG therapy is sometimes used to treat high-risk neuroblastoma that comes back after initial treatment.
Targeted therapy
Targeted therapy uses drugs or other substances to block the action of specific enzymes, proteins, or other molecules involved in the growth and spread of cancer cells.
- Monoclonal antibody therapy: Monoclonal antibodies are immune system proteins made in the laboratory to treat many diseases, including cancer. As a cancer treatment, these antibodies can attach to a specific target on cancer cells or other cells that may help cancer cells grow. The antibodies are able to then kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells.
- Dinutuximab is used to treat patients with high-risk neuroblastoma and neuroblastoma that has come back after treatment or has not responded to treatment.
- Ornithine decarboxylase inhibitor therapy slows the growth and division of cancer cells.
- Eflornithine may be given for two years after maintenance therapy for high-risk neuroblastoma.
Learn more about Targeted Therapy to Treat Cancer.
Other drug therapy
Other drugs used in combination to treat neuroblastoma include:
- Isotretinoin: A vitamin-like drug that slows the cancer's ability to make more cancer cells and changes how these cells look and act. This drug is taken by mouth.
Immunotherapy
Immunotherapy helps a child's immune system fight cancer.
- Granulocyte-macrophage colony-stimulating factor (GM-CSF): a cytokine that helps the body make more white blood cells, especially granulocytes and macrophages, which can attack and kill cancer cells. GM-CSF can also enhance the immune system response against cancer by increasing the number of cancer-fighting T cells.
- CAR T-cell therapy: The patient's T cells (a type of immune system cell) are changed so that they will attack certain proteins on the surface of cancer cells. T cells are taken from the patient, and special receptors are added to their surface in the laboratory. The changed cells are called chimeric antigen receptor (CAR) T cells. The CAR T cells are grown in the laboratory and given to the patient by infusion. The CAR T cells multiply in the patient's blood and attack cancer cells.
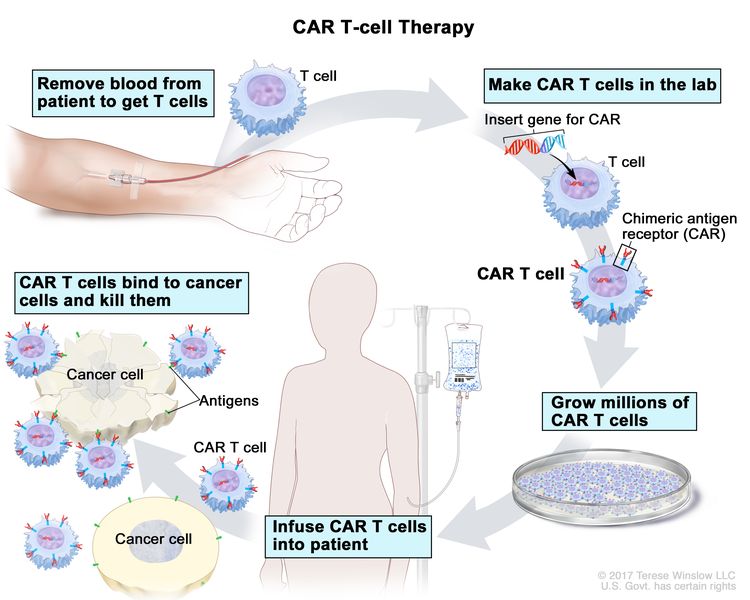
CAR T-cell therapy. A type of treatment in which a patient’s T cells (a type of immune cell) are changed in the laboratory so they will bind to cancer cells and kill them. Blood from a vein in the patient’s arm flows through a tube to an apheresis machine (not shown), which removes the white blood cells, including the T cells, and sends the rest of the blood back to the patient. Then, the gene for a special receptor called a chimeric antigen receptor (CAR) is inserted into the T cells in the laboratory. Millions of the CAR T cells are grown in the laboratory and then given to the patient by infusion. The CAR T cells are able to bind to an antigen on the cancer cells and kill them.
CAR T-cell therapy is being studied to treat neuroblastoma that has come back after treatment or has not responded to treatment.
Learn more about T-Cell Transfer Therapy.
New types of treatment are being tested in clinical trials.
A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for people with cancer. For some patients, taking part in a clinical trial may be an option. Because cancer in children is rare, taking part in a clinical trial should be considered.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. Some clinical trials are open only to patients who have not started treatment. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Learn more at Clinical Trials Information for Patients and Caregivers.
Treatment for neuroblastoma causes side effects and late effects.
To learn more about side effects that begin during treatment for cancer, visit Side Effects.
Side effects from cancer treatment that begin after treatment and continue for months or years are called late effects. Late effects of cancer treatment may include:
- physical problems, such as:
- tooth development
- intestinal blockage (obstruction)
- bone and cartilage growth
- hearing function
- metabolic syndrome (elevated blood pressure, elevated triglycerides, elevated cholesterol, increased body fat percentage)
- changes in mood, feelings, thinking, learning, or memory
- second cancers (new types of cancer), such as myelodysplastic syndrome, acute myeloid leukemia, thyroid cancer, or kidney cancer
Some late effects may be treated or controlled. It is important to talk with your child's doctors about the effects cancer treatment can have on your child. Learn more about Late Effects of Treatment for Childhood Cancer.
Follow-up care may be needed.
As your child goes through treatment, they will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your child's condition has changed or if the cancer has recurred (come back).
Follow-up care for children with neuroblastoma may include:
- urine catecholamine studies
- MIBG scan
Treatment of Low-Risk Neuroblastoma
For information about the treatments listed below, see the Treatment Option Overview section.
Treatment of newly diagnosed low-risk neuroblastoma may include:
- surgery followed by observation
- observation alone for infants younger than 6 months who have small adrenal tumors or for infants who do not have signs or symptoms of neuroblastoma
- observation with biopsy for infants younger than age 1 year who have favorable histology and meet other low-risk criteria
- chemotherapy with or without surgery, for children with symptoms or children whose tumor has continued to grow and cannot be removed by surgery
- chemotherapy, for certain patients
- radiation therapy to treat tumors that are causing serious problems and do not respond quickly to chemotherapy or surgery
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of Intermediate-Risk Neuroblastoma
For information about the treatments listed below, see the Treatment Option Overview section.
Treatment of newly diagnosed intermediate-risk neuroblastoma may include:
- Chemotherapy for children with symptoms or to shrink a tumor that cannot be removed by surgery. Surgery may be done after chemotherapy.
- Surgery alone for infants.
- Observation alone for infants.
- Radiation therapy to treat tumors that have continued to grow during treatment with chemotherapy or tumors that cannot be removed by surgery and have continued to grow after treatment with chemotherapy.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of High-Risk Neuroblastoma
For information about the treatments listed below, see the Treatment Option Overview section.
Children with newly diagnosed high-risk neuroblastoma usually receive treatment in three phases: induction, consolidation, and maintenance.
Treatment during induction may include:
- combination chemotherapy
- surgery
Treatment during consolidation may include:
- two courses of high-dose combination chemotherapy followed by stem cell rescue
- radiation therapy
Treatment during maintenance may include monoclonal antibody therapy (dinutuximab), granulocyte-macrophage colony-stimulating factor (GM-CSF), and isotretinoin.
Treatment after maintenance may include eflornithine.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of Stage MS Neuroblastoma
For information about the treatments listed below, see the Treatment Option Overview section.
There is no standard treatment for newly diagnosed stage MS, but treatment options include:
- observation and supportive care for children who have favorable tumor biology and do not have signs or symptoms
- chemotherapy, for children who have signs or symptoms, for very young infants, or for children with unfavorable tumor biology
- radiation therapy for children with neuroblastoma that has spread to the liver
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Treatment of Recurrent Neuroblastoma
For information about the treatments listed below, see the Treatment Option Overview section.
Patients First Treated for Low-Risk Neuroblastoma
Treatment for recurrent neuroblastoma that comes back in the area where the cancer first formed may include:
- surgery followed by observation or chemotherapy
- chemotherapy that may be followed by surgery
Treatment for recurrent neuroblastoma that comes back in other parts of the body or that has not responded to treatment may include:
- observation
- chemotherapy
- surgery followed by chemotherapy
- treatment as for newly diagnosed high-risk neuroblastoma, for children older than 18 months
Patients First Treated for Intermediate-Risk Neuroblastoma
Treatment for recurrent neuroblastoma that comes back in the area where the cancer first formed may include:
- surgery that may be followed by chemotherapy
- radiation therapy for children whose disease has gotten worse after chemotherapy and second-look surgery
Treatment for recurrent neuroblastoma that comes back in other parts of the body may include:
- treatment as for newly diagnosed high-risk neuroblastoma
Patients First Treated for High-Risk Neuroblastoma
There is no standard treatment for recurrent neuroblastoma in patients first treated for high-risk neuroblastoma. Treatment may include:
- Combination chemotherapy with monoclonal antibody therapy (dinutuximab).
- Iodine 131-MIBG therapy to relieve symptoms and improve quality of life. It may be given alone or in combination with chemotherapy, or followed by stem cell rescue.
- Chemotherapy.
- A clinical trial of CAR T-cell therapy.
Because there is no standard treatment, patients first treated for high-risk neuroblastoma may want to consider a clinical trial. Learn more about clinical trials at Clinical Trials Information for Patients and Caregivers.
Patients with Recurrent CNS Neuroblastoma
Treatment for neuroblastoma that recurs (comes back) in the central nervous system (CNS; brain and spinal cord) may include:
- surgery to remove the tumor in the CNS followed by radiation therapy
- chemotherapy, surgery, and radiation therapy
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
To Learn More About Neuroblastoma
For more information from the National Cancer Institute about neuroblastoma, see:
- Neuroblastoma Home Page
- Neuroblastoma Screening
- Computed Tomography (CT) Scans and Cancer
- Drugs Approved for Neuroblastoma
- Targeted Therapy to Treat Cancer
- Immunotherapy to Treat Cancer
- New Approaches to Neuroblastoma Therapy (NANT)
For more childhood cancer information and other general cancer resources, visit:
- About Cancer
- Childhood Cancers
- CureSearch for Children's Cancer
- Late Effects of Treatment for Childhood Cancer
- Adolescents and Young Adults with Cancer
- Children with Cancer: A Guide for Parents
- Cancer in Children and Adolescents
- Cancer Staging
- Coping with Cancer
- Questions to Ask Your Doctor about Cancer
- For Survivors, Caregivers, and Advocates
About This PDQ Summary
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute's (NCI's) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government’s center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of neuroblastoma. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary ("Updated") is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Pediatric Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become "standard." Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI's website. For more information, call the Cancer Information Service (CIS), NCI's contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as “NCI’s PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary].”
The best way to cite this PDQ summary is:
PDQ® Pediatric Treatment Editorial Board. PDQ Neuroblastoma Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/neuroblastoma/patient/neuroblastoma-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389278]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website’s E-mail Us.
Updated:
Source URL: https://www.cancer.gov/node/5031/syndication
Source Agency: National Cancer Institute (NCI)
Captured Date: 2013-09-14 09:02:35.0