








Tratamiento del cáncer de testículo
En Montefiore Einstein Comprehensive Cancer Center, puede acceder a una atención integral y compasiva para el cáncer testicular. Creemos que cada persona es única y que no hay dos tipos de cáncer iguales. Por eso, nuestro equipo desarrolla un plan de tratamiento personalizado para cada paciente al que atendemos, diseñado para lograr el mejor resultado posible.
Somos uno de los primeros centros de cáncer designados por el NCI, y como tal, durante más de 50 años, hemos sido líderes en la investigación, el diagnóstico y el tratamiento de más de 200 tipos de cáncer.
Nuestro equipo de cáncer testicular está a la vanguardia de los métodos de tratamiento más nuevos e innovadores. Puede esperar una atención compasiva y personalizada que cumpla con los más altos estándares de calidad y seguridad. Nuestro objetivo es lo que llamamos la trilogía: eliminar el cáncer, normalizar la función urinaria y restaurar la función sexual. Nuestro programa de recuperación de pacientes respalda estos objetivos, al mismo tiempo que brinda acceso a grupos de apoyo dirigidos por personal de enfermería.
También se beneficia de nuestra investigación continua sobre tratamientos nuevos e innovadores, algunos de los cuales pueden incorporarse a su atención antes de su disponibilidad generalizada si decide participar en uno de nuestros ensayos clínicos oncológicos de vanguardia. Nuestro equipo está comprometido con la atención integral de la persona y ofrece a los pacientes una amplia gama de servicios de apoyo y programas de cuidados paliativos para satisfacer las complejas necesidades médicas, emocionales y espirituales de los pacientes y sus familias.
Cuando necesite atención médica para el cáncer testicular, recurra a nuestros proveedores, quienes se dedican con pasión a combatir el cáncer y a atender todas sus necesidades de salud.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Tratamiento del cáncer de testículo (PDQ®): versión para pacientes
Información general sobre el cáncer testicular
Puntos clave
- El cáncer testicular es una enfermedad en la que se forman células malignas (cancerosas) en los tejidos de uno o ambos testículos.
- El historial de salud puede afectar el riesgo de padecer cáncer testicular.
- Los signos y síntomas del cáncer testicular incluyen hinchazón o malestar en el escroto.
- Para diagnosticar el cáncer testicular se utilizan pruebas que examinan los testículos y la sangre.
- Certain factors affect prognosis (chance of recovery) and treatment options.
- El tratamiento para el cáncer testicular puede causar infertilidad.
El cáncer testicular es una enfermedad en la que se forman células malignas (cancerosas) en los tejidos de uno o ambos testículos.
Los testículos son dos glándulas con forma de huevo ubicadas dentro del escroto (un saco de piel suelta que se encuentra directamente debajo del pene). Los testículos se mantienen dentro del escroto mediante el cordón espermático, que también contiene los conductos deferentes y los vasos y nervios de los testículos.
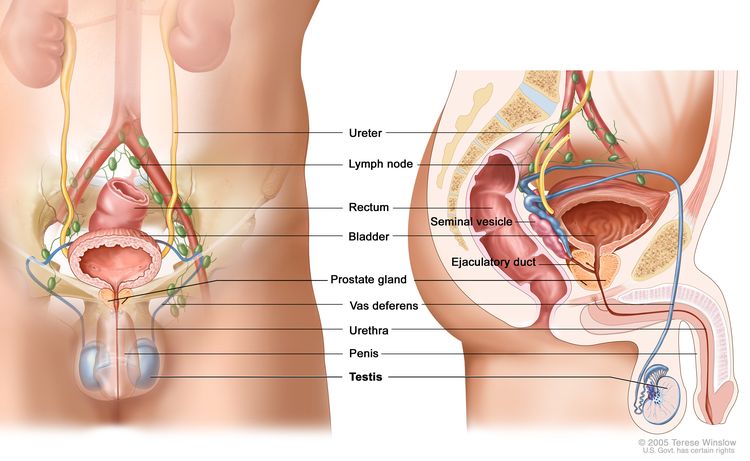
Anatomía de los sistemas reproductor y urinario masculinos; se muestran los testículos, la próstata, la vejiga y otros órganos.
Los testículos son las glándulas sexuales masculinas y producen testosterona y esperma. Las células germinales dentro de los testículos producen espermatozoides inmaduros que viajan a través de una red de túbulos (tubos diminutos) y tubos más grandes hasta el epidídimo (un tubo largo y enrollado al lado de los testículos), donde los espermatozoides maduran y se almacenan.
Casi todos los cánceres testiculares comienzan en las células germinales. Los dos tipos principales de tumores de células germinales testiculares son los seminomas y los no seminomas. Estos dos tipos crecen y se propagan de manera diferente y se tratan de manera diferente. Los no seminomas tienden a crecer y propagarse más rápidamente que los seminomas. Los seminomas son más sensibles a la radiación. Un tumor testicular que contiene células tanto seminomatosas como no seminomatosas se trata como un tumor no seminomatoso.
El cáncer testicular es el cáncer más común en hombres de 20 a 35 años.
El historial de salud puede afectar el riesgo de padecer cáncer testicular.
Todo lo que aumenta las posibilidades de que una persona contraiga una enfermedad se llama factor de riesgo. No todas las personas con uno o más de estos factores de riesgo desarrollarán cáncer testicular, y la enfermedad se desarrollará en personas que no tienen ningún factor de riesgo conocido. Hable con su médico si cree que puede estar en riesgo. Los factores de riesgo del cáncer testicular incluyen:
- Haber tenido un testículo no descendido
- Haber tenido un desarrollo anormal de los testículos
- Tener un historial de salud personal de cáncer testicular
- Tener un historial de salud familiar de cáncer testicular (especialmente en un padre o hermano)
- Ser blanco
Los signos y síntomas del cáncer testicular incluyen hinchazón o malestar en el escroto.
Estos y otros signos y síntomas pueden estar causados por cáncer testicular u otras afecciones. Consulte con su médico si presenta alguno de los siguientes síntomas:
Para diagnosticar el cáncer testicular se utilizan pruebas que examinan los testículos y la sangre.
In addition to asking about your personal and family health history and doing a physical exam, your doctor may perform the following tests and procedures:
- Examen físico de los testículos: examen en el que el médico busca bultos, hinchazón o dolor en los testículos.
- Ecografía de los testículos: procedimiento en el que ondas sonoras de alta energía (ultrasonido) rebotan en tejidos u órganos internos y producen ecos. Los ecos forman una imagen de los tejidos del cuerpo llamada ecograma.
- Pruebas séricas de marcadores tumorales: procedimiento en el que se toma una muestra de sangre y se examina para medir las cantidades de ciertas sustancias liberadas en la sangre por órganos, tejidos o células tumorales en el cuerpo. Ciertas sustancias están relacionadas con tipos específicos de cáncer cuando se encuentran en niveles elevados en la sangre. Estos se llaman marcadores tumorales. Los siguientes marcadores tumorales se utilizan para detectar el cáncer testicular:
- Alfafetoproteína (AFP)
- Gonadotropina coriónica humana beta (beta-hCG)
- Orquiectomía inguinal: procedimiento para extirpar todo el testículo a través de una incisión en la ingle. Luego se observa una muestra de tejido del testículo bajo un microscopio para detectar células cancerosas. (El cirujano no corta el escroto hasta el testículo para extraer la muestra de tejido para realizar la biopsia, porque si hay cáncer, este procedimiento podría hacer que se propagase al escroto y los ganglios linfáticos. Es importante elegir un cirujano que tenga experiencia con este tipo de cirugías). Si se encuentra cáncer, entonces se determina el tipo de célula (seminoma o no seminoma) para poder planificar el tratamiento.
Certain factors affect prognosis (chance of recovery) and treatment options.
El pronóstico y las opciones de tratamiento dependen de los siguientes aspectos:
- Estadio del cáncer (si está en el testículo o cerca de él, o si se ha extendido a otras partes del cuerpo, y niveles sanguíneos de AFP, beta-hCG y LDH)
- Tipo de cáncer
- Tamaño del tumor
- Número y tamaño de los ganglios linfáticos retroperitoneales
El cáncer testicular generalmente se puede curar en pacientes que reciben quimioterapia o radioterapia adyuvante después del tratamiento primario.
El tratamiento para el cáncer testicular puede causar infertilidad.
Ciertos tratamientos para el cáncer testicular pueden causar infertilidad, la cual puede ser permanente. Los pacientes que deseen tener hijos deben considerar la crioconservación de espermatozoides antes de recibir tratamiento. La crioconservación de espermatozoides es el proceso de congelar esperma y almacenarlo para su uso posterior.
Estadios del cáncer de testículo
Puntos clave
- Una vez que se diagnostica el cáncer testicular, se realizan pruebas para determinar si las células cancerosas se han extendido dentro de los testículos o hacia otras partes del cuerpo.
- There are three ways that cancer spreads in the body.
- El cáncer puede extenderse desde donde comenzó a otras partes del cuerpo.
- Se utilizan los siguientes estadios para el cáncer de testículo:
- Estadio 0
- Estadio I
- Estadio II
- Estadio III
- El cáncer de testículo puede recidivar (regresar) después de haber sido tratado.
Una vez que se diagnostica el cáncer testicular, se realizan pruebas para determinar si las células cancerosas se han extendido dentro de los testículos o hacia otras partes del cuerpo.
El proceso utilizado para determinar si el cáncer se ha propagado dentro de los testículos o a otras partes del cuerpo se denomina estadificación. La información obtenida mediante el proceso de estadificación determina el estadio de la enfermedad. Es importante conocer el estadio para planificar el tratamiento.
En el proceso de estadificación pueden utilizarse las siguientes pruebas y procedimientos:
- Radiografía del tórax: radiografía de los órganos y huesos del interior del tórax. Los rayos X son un tipo de haz de energía que puede atravesar el cuerpo, plasmarse en una película y generar una imagen de áreas del interior del cuerpo.
- Exploración por tomografía computarizada (TAC): procedimiento que genera una serie de imágenes detalladas de áreas internas del cuerpo, como el abdomen, tomadas desde diferentes ángulos. Las imágenes son tomadas por una computadora conectada a una máquina de rayos X. Se puede inyectar un tinte en una vena o ingerirlo para ayudar a que los órganos o tejidos se vean más claramente. Este procedimiento también se llama tomografía axial computarizada.
- Imágenes por resonancia magnética (IRM): procedimiento que utiliza un imán, ondas de radio y una computadora para generar una serie de imágenes detalladas de áreas internas del cuerpo, como el abdomen. Este procedimiento también se llama resonancia magnética nuclear (IRMN).
- Disección de ganglios linfáticos abdominales: procedimiento quirúrgico en el que se extirpan los ganglios linfáticos del abdomen y se examina una muestra de tejido bajo un microscopio para detectar signos de cáncer. Este procedimiento también se llama linfadenectomía. En el caso de los pacientes con tumores no seminomatosos, la extirpación de los ganglios linfáticos puede ayudar a detener la propagación de la enfermedad. Las células cancerosas en los ganglios linfáticos de pacientes con seminoma se pueden tratar con radioterapia.
- Pruebas séricas de marcadores tumorales: procedimiento en el que se toma una muestra de sangre y se examina para medir las cantidades de ciertas sustancias liberadas en la sangre por órganos, tejidos o tumor células en el cuerpo. Ciertas sustancias están relacionadas con tipos específicos de cáncer cuando se encuentran en niveles elevados en la sangre. Estos se llaman marcadores tumorales. Los siguientes tres marcadores tumorales se utilizan en la estadificación del cáncer de testículo:
- Alfafetoproteína (AFP)
- Gonadotropina coriónica humana beta (beta-hCG)
- Lactato deshidrogenasa (LDH)
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
El cáncer puede extenderse desde donde comenzó a otras partes del cuerpo.
Cuando el cáncer se extiende a otra parte del cuerpo se denomina metástasis. Las células cancerosas se desprenden de donde comenzaron (tumor primario) y viajan a través del sistema linfático o la sangre.
- Sistema linfático: el cáncer entra en el sistema linfático, viaja a través de los vasos linfáticos y forma un tumor (tumor metastásico) en otra parte del cuerpo.
- Sangre: el cáncer llega a la sangre, viaja a través de los vasos sanguíneos y forma un tumor (tumor metastásico) en otra parte del cuerpo.
El tumor metastásico es el mismo tipo de cáncer que el tumor primario. Por ejemplo, si el cáncer testicular se propaga al pulmón, las células cancerosas del pulmón son en realidad células cancerosas testiculares. La enfermedad es cáncer testicular metastásico, no cáncer de pulmón.
Se utilizan los siguientes estadios para el cáncer de testículo:
Estadio 0
En el estadio 0, se encuentran células anormales en los pequeños túbulos donde los espermatozoides comienzan a desarrollarse. Estas células anormales pueden convertirse en cáncer y extenderse al tejido normal cercano. Todos los niveles de marcadores tumorales son normales. El estadio 0 también se llama neoplasia de células germinales in situ.
Estadio I
En el estadio I, se ha formado cáncer. El estadio I se divide en los estadios IA, IB e IS.
- En el estadio IA, el El cáncer se encuentra en la testículo, incluido el rete testis, pero no se ha extendido a los vasos sanguíneos o Vasos linfaticos en el testículo.
Todos los niveles de marcadores tumorales son normales.
- En el estadio IB, el El cáncer:
- Se encuentra en el testículo, incluida la rete testis, y se ha extendido a los vasos sanguíneos o linfáticos del testículo; o
- Se ha extendido al tejido blando hiliar (tejido formado por fibras y grasa con vasos sanguíneos y vasos linfáticos), el epidídimo o las membranas externas que rodean el testículo; o
- Se ha extendido al cordón espermático; o
- Se ha extendido al escroto.
Todos los niveles de marcadores tumorales son normales.
- En la etapa IS, el El cáncer se encuentra en cualquier parte del testículo y puede haberse extendido al cordón espermático o escroto.
Los niveles de marcadores tumorales varían entre cifras ligeramente superiores al rango normal y niveles significativamente altos.
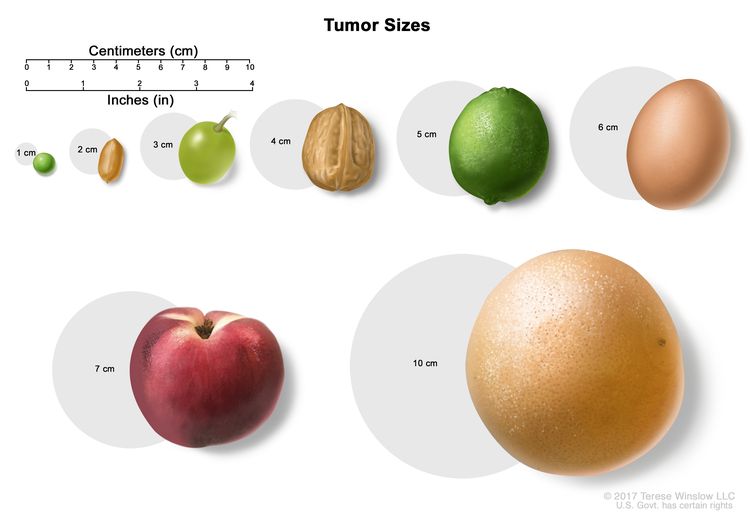
El tamaño de los tumores a menudo se mide en centímetros (cm) o pulgadas (in). A veces se usan alimentos comunes para mostrar el tamaño de un tumor en centímetros: una arveja o guisante (1 cm), un maní o cacahuate (2 cm), una uva (3 cm), una nuez (4 cm), una lima o limón verde (5 cm o 2 in), un huevo (6 cm), un durazno (7 cm) y un pomelo (10 cm o 4 in).
Estadio II
El estadio II se divide en los estadios IIA, IIB y IIC.
- En el estadio IIA, el El cáncer se encuentra en cualquier parte del testículo y puede haberse extendido al cordón espermático o escroto. El cáncer se ha propagado a entre uno y cinco ganglios linfáticos cercanos y los ganglios linfáticos miden 2 centímetros o menos.
Todos los niveles de marcadores tumorales son normales o ligeramente superiores a lo normal.
- En el estadio IIB, el El cáncer se encuentra en cualquier parte del testículo y puede haberse extendido al cordón espermático o escroto. El cáncer se ha propagado a:
- Un ganglio linfático cercano y el ganglio linfático mide más de 2 centímetros pero no más de 5 centímetros; o
- Más de cinco ganglios linfáticos cercanos y los ganglios linfáticos no miden más de 5 centímetros; o
- Un ganglio linfático cercano y el cáncer se ha extendido fuera del ganglio linfático.
Todos los niveles de marcadores tumorales son normales o ligeramente superiores a lo normal.
- En el estadio IIC, el El cáncer se encuentra en cualquier parte del testículo y puede haberse extendido al cordón espermático o escroto. El cáncer se ha propagado a los ganglios linfáticos cercanos y el ganglio linfático mide más de 5 centímetros.
Todos los niveles de marcadores tumorales son normales o ligeramente superiores a lo normal.
Estadio III
El estadio III se divide en los estadios IIIA, IIIB y IIIC.
- En el estadio IIIA, el El cáncer se encuentra en cualquier parte del testículo y puede haberse extendido al cordón espermático o escroto. Es posible que el cáncer se haya propagado a uno o más ganglios linfáticos. El cáncer se ha extendido a los ganglios linfáticos distantes o a los pulmones.
Todos los niveles de marcadores tumorales son normales o ligeramente superiores a lo normal.
- En el estadio IIIB, el El cáncer se encuentra en cualquier parte del testículo y puede haberse extendido al cordón espermático o escroto. El cáncer se ha propagado:
- A uno o más ganglios linfáticos cercanos y no se ha extendido a otras partes del cuerpo; o
- A uno o más ganglios linfáticos cercanos. El cáncer se ha extendido a los ganglios linfáticos distantes o a los pulmones.
El nivel de uno o más marcadores tumorales está moderadamente por encima de lo normal.
- En el estadio IIIC, el El cáncer se encuentra en cualquier parte del testículo y puede haberse extendido al cordón espermático o escroto. El cáncer se ha propagado:
- A uno o más ganglios linfáticos cercanos y no se ha extendido a otras partes del cuerpo; o
- A uno o más ganglios linfáticos cercanos. El cáncer se ha extendido a los ganglios linfáticos distantes o a los pulmones.
El nivel de uno o más marcadores tumorales es alto.
o
El cáncer se encuentra en cualquier parte del testículo y puede haberse extendido al cordón espermático o al escroto. El cáncer no se ha extendido a los ganglios linfáticos distantes ni al pulmón, sino que se ha extendido a otras partes del cuerpo, como el hígado o los huesos.
Los niveles de marcadores tumorales oscilan entre normales y altos.
El cáncer de testículo puede recidivar (regresar) después de haber sido tratado.
El cáncer puede reaparecer muchos años después del cáncer inicial, en el otro testículo o en otras partes del cuerpo.
Treatment Option Overview
Puntos clave
- Existen diferentes tipos de tratamiento para los pacientes con cáncer de testículo.
- Los tumores testiculares se dividen en tres grupos, según cómo se espera que respondan al tratamiento.
- Buen pronóstico
- Pronóstico intermedio
- Pronóstico desfavorable
- The following types of treatment are used:
- Cirugía
- Radioterapia
- Quimioterapia
- Vigilancia
- Quimioterapia de dosis alta con trasplante de células madre
- New types of treatment are being tested in clinical trials.
- El tratamiento para el cáncer testicular puede causar efectos secundarios.
- Patients may want to think about taking part in a clinical trial.
- Patients can enter clinical trials before, during, or after starting their cancer treatment.
- Pueden ser necesarias pruebas de seguimiento.
Existen diferentes tipos de tratamiento para los pacientes con cáncer de testículo.
Existen distintos tipos de tratamientos disponibles para los pacientes con cáncer testicular. Algunos tratamientos son estándar (el tratamiento que se utiliza actualmente) y otros se están probando en ensayos clínicos. Un ensayo clínico de tratamiento es un estudio de investigación cuyo objetivo es ayudar a mejorar los tratamientos actuales u obtener información sobre nuevos tratamientos para pacientes con cáncer. Cuando los ensayos clínicos muestran que un nuevo tratamiento es mejor que el tratamiento estándar, el nuevo tratamiento puede convertirse en el tratamiento estándar. Es posible que los pacientes quieran pensar en participar en un ensayo clínico. Algunos ensayos clínicos están abiertos solo a pacientes que no han comenzado el tratamiento.
Los tumores testiculares se dividen en tres grupos, según cómo se espera que respondan al tratamiento.
Buen pronóstico
Para casos no seminomatosos, deben cumplirse todas las siguientes condiciones:
- El tumor se encuentra únicamente en el testículo o en el retroperitoneo (área fuera o detrás de la pared abdominal).
- El tumor no se ha diseminado a otros órganos además de los pulmones.
- Los niveles de todos los marcadores tumorales están ligeramente por encima de lo normal.
En el caso del seminoma, deben cumplirse todas las siguientes condiciones:
- El tumor no se ha extendido a otros órganos aparte de los pulmones.
- El nivel de alfafetoproteína (AFP) es normal. La gonadotropina coriónica humana beta (beta-hCG) y la lactato deshidrogenasa (LDH) pueden estar en cualquier nivel.
Pronóstico intermedio
Para el no seminoma, deben cumplirse todas las siguientes condiciones:
- El tumor se encuentra en un solo testículo o en el retroperitoneo (área fuera o detrás de la pared abdominal).
- El tumor no se ha extendido a otros órganos aparte de los pulmones.
- El nivel de cualquiera de los marcadores tumorales se encuentra marcadamente por encima de lo normal.
Para el seminoma, debe darse todo lo siguiente:
- El tumor se ha extendido a otros órganos además de los pulmones.
- El nivel de AFP es normal. Beta-hCG y LDH pueden estar en cualquier nivel.
Pronóstico desfavorable
Para el no seminoma, debe presentarse por lo menos una de las condiciones siguientes:
- El tumor está en el centro del tórax entre los pulmones.
- El tumor se ha extendido a otros órganos además de los pulmones.
- El nivel de cualquiera de los marcadores tumorales es alto.
Los seminomas de testículo no tienen un grupo de mal pronóstico.
The following types of treatment are used:
Cirugía
La cirugía para extirpar el testículo (orquiectomía inguinal) y algunos de los ganglios linfáticos se puede realizar en el momento del diagnóstico y la estadificación. (Consulte las secciones Información general y Estadios de este resumen). Los tumores que se han extendido a otras partes del cuerpo se pueden extirpar parcial o totalmente mediante cirugía.
Después de que el médico extirpe todo el cáncer que se puede observar en el momento de la cirugía, algunos pacientes podrían recibir quimioterapia o radioterapia para eliminar cualquier célula cancerosa restante. El tratamiento que se administra después de la cirugía para reducir el riesgo de reaparición del cáncer se denomina terapia adyuvante.
Radioterapia
La radioterapia es un tratamiento contra el cáncer que utiliza rayos X de alta energía u otros tipos de radiación para matar las células cancerosas o evitar que crezcan. Para la radioterapia externa se usa una máquina que envía la radiación hacia la zona con cáncer desde el exterior del cuerpo.
Quimioterapia
La quimioterapia es un tratamiento contra el cáncer que utiliza medicamentos para detener el crecimiento de las células cancerosas, ya sea matándolas o impidiendo que se dividan. Cuando la quimioterapia se toma por vía oral o se inyecta en una vena o músculo, los medicamentos ingresan al torrente sanguíneo y pueden llegar a las células cancerosas de todo el cuerpo (quimioterapia sistémica).
Consulte Medicamentos aprobados para el cáncer de testículo para obtener más información.
Vigilancia
La vigilancia consiste en seguir de cerca la afección del paciente sin administrarle ningún tratamiento a menos que haya cambios en los resultados de las pruebas. Se utiliza para detectar signos tempranos de que el cáncer ha reaparecido (regresado). Durante la vigilancia, a los pacientes se les realizan determinados exámenes y pruebas de forma periódica.
Quimioterapia de dosis alta con trasplante de células madre
Se administran dosis altas de quimioterapia para matar las células cancerosas. El tratamiento contra el cáncer también destruye las células sanas, incluidas las células productoras de sangre. El trasplante de células madre es un tratamiento para reemplazar las células productoras de sangre. Las células madre (células sanguíneas inmaduras) se extraen de la sangre o de la médula ósea del paciente o de un donante y se congelan y almacenan. Una vez que el paciente completa la quimioterapia, las células madre almacenadas se descongelan y se devuelven al paciente mediante una infusión. Estas células madre reinfundidas se convierten en células sanguíneas del cuerpo que restauran las células destruidas.
Consulte Medicamentos aprobados para el cáncer de testículo para obtener más información.
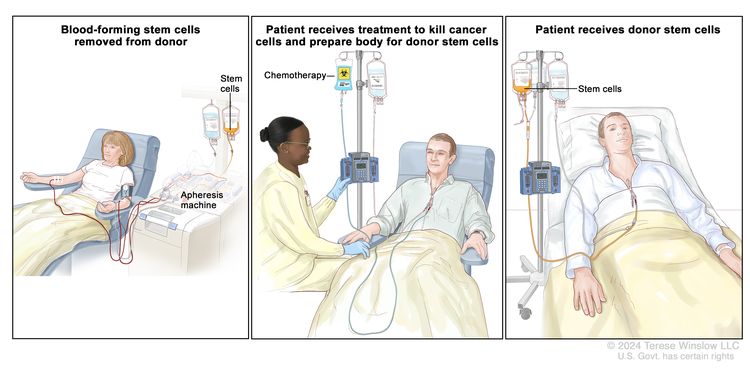
Trasplante de células madre de un donante. (Paso 1): Cuatro o cinco días antes de la recolección de células madre del donante, este recibe un medicamento para aumentar la cantidad de células madre que circulan por su torrente sanguíneo (no se muestra en la imagen). Las células madre hematopoyéticas se extraen del donante a través de una vena grande del brazo. La sangre fluye a través de una máquina de aféresis que extrae las células madre. El resto de la sangre se devuelve al donante a través de una vena del otro brazo. (Paso 2): El paciente recibe quimioterapia para destruir las células cancerosas y preparar su cuerpo para las células madre del donante. El paciente también puede recibir radioterapia (no se muestra en la imagen). (Paso 3): El paciente recibe una infusión de las células madre del donante.
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the NCI website.
El tratamiento para el cáncer testicular puede causar efectos secundarios.
For information about side effects caused by treatment for cancer, visit our Side Effects page.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Pueden ser necesarias pruebas de seguimiento.
A medida que avanza el tratamiento, se le realizarán pruebas o controles de seguimiento. Es posible que se repitan algunas pruebas para diagnosticar o estadificar el cáncer con el fin de evaluar cómo está funcionando el tratamiento. Las decisiones sobre si continuar, modificar o suspender el tratamiento pueden basarse en los resultados de estas pruebas.
Algunas pruebas seguirán realizándose de manera periódica después de terminar el tratamiento. Los resultados pueden indicar si su afección ha cambiado o si el cáncer ha redicivado (regresado).
Los hombres que han tenido cáncer testicular tienen un mayor riesgo de desarrollar cáncer en el otro testículo. Se recomienda al paciente que revise regularmente el otro testículo e informe inmediatamente a un médico sobre cualquier síntoma inusual.
Los exámenes clínicos a largo plazo son muy importantes. El paciente probablemente tendrá controles frecuentes durante el primer año después de la cirugía y con menor frecuencia después.
Tratamiento del estadio 0 (neoplasia intraepitelial de testículo)
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento del estadio 0 puede incluir las siguientes opciones:
- Radioterapia.
- Vigilancia.
- Cirugía para extirpar el testículo
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del cáncer de testículo en estadio I
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento del cáncer testicular en estadio I depende de si el cáncer es un seminoma o no seminoma.
El tratamiento del seminoma puede incluir las siguientes opciones:
- Cirugía para extirpar el testículo, seguida de vigilancia
- Para los pacientes que desean un tratamiento activo en lugar de vigilancia, se utiliza la siguiente opción:
- Cirugía para extirpar el testículo, seguida de quimioterapia
El tratamiento del no seminoma puede incluir las siguientes opciones:
- Cirugía para extirpar el testículo, con seguimiento a largo plazo
- Cirugía para extirpar el testículo y los ganglios linfáticos del abdomen, con seguimiento a largo plazo
- Cirugía seguida de quimioterapia para pacientes con alto riesgo de recurrencia, con seguimiento a largo plazo
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del cáncer de testículo en estadio II
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento del cáncer testicular en estadio II depende de si el cáncer es un seminoma o no seminoma.
El tratamiento del seminoma puede incluir las siguientes opciones:
- Cuando el tumor mide 5 centímetros o menos:
- Cirugía para extirpar el testículo, seguida de radioterapia en los ganglios linfáticos del abdomen y la pelvis
- Quimioterapia combinada.
- Cirugía para extirpar el testículo y los ganglios linfáticos del abdomen
- Cuando el tumor mide más de 5 centímetros:
- Cirugía para extirpar el testículo, seguida de quimioterapia combinada o radioterapia en los ganglios linfáticos del abdomen y la pelvis, con seguimiento a largo plazo
El tratamiento del no seminoma puede incluir las siguientes opciones:
- Cirugía para extirpar el testículo y los ganglios linfáticos, con seguimiento a largo plazo
- Cirugía para extirpar el testículo y los ganglios linfáticos, seguida de quimioterapia combinada y seguimiento a largo plazo
- Cirugía para extirpar el testículo, seguida de quimioterapia combinada y una segunda cirugía si el cáncer persiste, con seguimiento a largo plazo.
- Para el cáncer que se ha propagado y se cree que pone en peligro la vida, quimioterapia combinada antes de la cirugía para extirpar el testículo
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del cáncer de testículo en estadio III
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento del cáncer testicular en estadio III depende de si el cáncer es un seminoma o no seminoma.
El tratamiento del seminoma puede incluir las siguientes opciones:
- Cirugía Para eliminar el testículo, seguida por Quimioterapia combinada. Si hay tumores restante después de la Quimioterapia, el tratamiento puede ser uno de los siguientes:
- Vigilancia sin tratamiento a menos que los tumores crezcan.
- Vigilancia de tumores que midan menos de 3 centímetros y cirugía para extirpar tumores que midan más de 3 centímetros.
- Una exploración PET dos meses después de la quimioterapia y cirugía para extirpar los tumores que aparecen con cáncer en la exploración.
- Participación en un ensayo clínico de quimioterapia
El tratamiento del no seminoma puede incluir las siguientes opciones:
- Cirugía para extirpar el testículo, seguida de quimioterapia combinada
- Quimioterapia combinada seguida de cirugía para extirpar el testículo y todos los tumores restantes. Se puede administrar quimioterapia adicional si el tejido tumoral extirpado contiene células cancerosas en crecimiento o si las pruebas de seguimiento muestran que el cáncer está progresando.
- Para el cáncer que se ha propagado y se cree que pone en peligro la vida, quimioterapia combinada antes de la cirugía para extirpar el testículo
- Participación en un ensayo clínico de quimioterapia
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del cáncer de testículo recidivante
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento del cáncer testicular recurrente puede incluir las siguientes opciones:
- Quimioterapia combinada.
- Quimioterapia de dosis alta y trasplante de células madre
- Cirugía para eliminar el El cáncer que presenta una de estas características:
- Ha vuelto más de dos años después de la remisión completa.
- Ha vuelto en un solo lugar y no responde a la quimioterapia.
- Participación en un ensayo clínico de una terapia nueva
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Más información sobre el cáncer testicular
Para obtener más información del National Cancer Institute sobre el cáncer de testículo, consulte las siguientes páginas web:
- Página principal sobre el cáncer de testículo
- Detección del cáncer de testículo
- Medicamentos aprobados para el cáncer de testículo
For general cancer information and other resources from the National Cancer Institute, visit:
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen de información sobre el cáncer del PDQ contiene información actualizada sobre el tratamiento del cáncer de testículo. Su objetivo es informar y ayudar a los pacientes, las familias y los cuidadores. No proporciona directrices ni recomendaciones formales para tomar decisiones sobre la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre el tratamiento para adultos. Tratamiento del cáncer testicular (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Actualizado:
URL de origen: https://www.cancer.gov/node/4590/syndication
Agencia de origen: National Cancer Institute (NCI)
Fecha de captura: 2013-09-14 09:02:19.0