








Tratamiento del cáncer de recto
Acceda a una atención excepcional para el cáncer de recto y otros cánceres gastrointestinales en el Montefiore Einstein Comprehensive Cancer Center. Nuestro equipo multidisciplinario cuenta con una amplia experiencia en el tratamiento de este tipo de cáncer. Como uno de los primeros centros del cáncer designados por el NCI, llevamos más de 50 años liderando la investigación, el diagnóstico y el tratamiento de más de 200 tipos de cáncer.
Estamos a la vanguardia en el tratamiento y la investigación del cáncer de recto y otros cánceres gastrointestinales. El Programa de Cáncer Colorrectal del Montefiore Einstein Comprehensive Cancer Center permite a los pacientes acceder a médicos y cirujanos reconocidos a nivel nacional, quienes ofrecen un tratamiento excelente para todas los estadios de la enfermedad y cuentan con una amplia experiencia en casos recurrentes y avanzados de cáncer colorrectal. Nuestro programa, uno de los pocos de este tipo en el mundo, se distingue por su enfoque multidisciplinario en la prevención y el tratamiento del cáncer colorrectal, garantizando una atención integral y personalizada para cada paciente.
Cuando necesite atención médica para el cáncer colorrectal, confíe en nuestros proveedores, muy comprometidos con erradicar el cáncer y atender todas sus necesidades de salud.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Tratamiento del cáncer de recto (PDQ®): versión para pacientes
Información general sobre el cáncer de recto
Puntos clave
- El cáncer de recto es un tipo de cáncer que se forma en los tejidos del recto.
- El historial de salud influye en el riesgo de padecer esta enfermedad.
- Entre los síntomas del cáncer de recto se incluyen la presencia de sangre en las heces o un cambio en los hábitos intestinales.
- Para diagnosticar el cáncer de recto se utilizan pruebas que examinan el recto y el colon.
- Una vez que se ha confirmado el diagnóstico de cáncer de recto, se realizan pruebas de imágenes para determinar si las células cancerosas se han diseminado dentro del recto o a otras partes del cuerpo.
- Some people decide to get a second opinion.
- Certain factors affect prognosis (chance of recovery) and treatment options.
El cáncer de recto es un tipo de cáncer que se forma en los tejidos del recto.
El recto forma parte del sistema digestivo. Este sistema absorbe los nutrientes ( vitaminas, minerales, carbohidratos, grasas, proteínas y agua) de los alimentos y ayuda a eliminar los desechos del cuerpo. El sistema digestivo está compuesto por el esófago, el estómago y los intestinos delgado y grueso. El colon ( intestino grueso) es la parte principal del intestino grueso y mide aproximadamente 1,5 metros de largo. El recto y el canal anal, en conjunto, forman la última parte del intestino grueso y miden entre 15 y 20 centímetros de largo. El canal anal termina en el ano (la abertura del intestino grueso hacia el exterior del cuerpo).
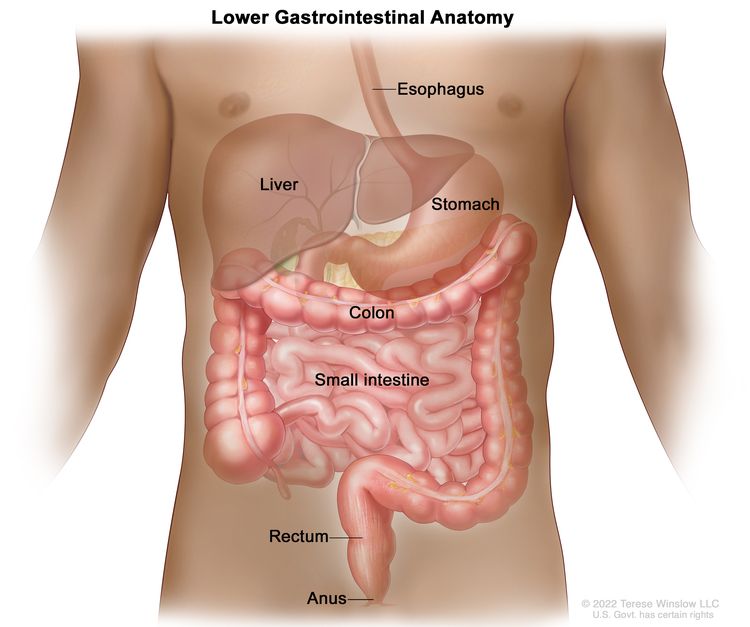
Anatomy of the lower gastrointestinal (digestive) system showing the colon, rectum, and anus. Other organs that make up the digestive system are also shown.
El historial de salud influye en el riesgo de padecer esta enfermedad.
El cáncer colorrectal se produce por ciertas alteraciones en el funcionamiento de las células colorrectales, especialmente en su crecimiento y división celular. Existen muchos factores de riesgo para el cáncer colorrectal, pero muchos no lo causan directamente. En cambio, aumentan la probabilidad de daño en el ADN celular, lo que puede derivar en cáncer colorrectal. Para obtener más información sobre el desarrollo del cáncer, consulte ¿Qué es el cáncer?
Un factor de riesgo es cualquier elemento que aumenta la probabilidad de desarrollar una enfermedad. Algunos factores de riesgo del cáncer colorrectal, como el tabaquismo, se pueden modificar. Sin embargo, otros factores de riesgo incluyen aspectos que no se pueden cambiar, como el historial de salud familiar. Conocer los factores de riesgo del cáncer colorrectal puede ayudarle a tomar medidas para reducir su riesgo.
Los factores de riesgo del cáncer colorrectal incluyen:
- tener un familiar de primer grado (padre, madre, hermano/a o hijo/a) con antecedentes de cáncer de colon o recto
- tener antecedentes personales de cáncer de colon, recto u ovario
- Tener un historial de salud personal de adenomas de riesgo alto (pólipos colorrectales de 1 centímetro o más o con células de apariencia anómala con microscopio)
- Haber heredado cambios en ciertos genes que aumentan el riesgo de poliposis adenomatosa familiar (PAF) o síndrome de Lynch (cáncer colorrectal hereditario sin poliposis)
- tener antecedentes personales de colitis ulcerosa crónica o enfermedad de Crohn durante 8 años o más
- Consumir tres o más bebidas alcohólicas al día
- Fumar cigarrillos
- Ser negro
- Tener obesidad
La edad avanzada es un factor de riesgo importante para la mayoría de los cánceres, ya que la probabilidad de desarrollar la enfermedad aumenta con el envejecimiento.
Tener uno o más de estos factores de riesgo no significa que vaya a desarrollar cáncer colorrectal. Muchas personas con factores de riesgo nunca desarrollan cáncer colorrectal, mientras que otras sin factores de riesgo conocidos sí lo hacen. Hable con su médico si cree que podría tener un mayor riesgo.
Entre los síntomas del cáncer de recto se incluyen la presencia de sangre en las heces o un cambio en los hábitos intestinales.
Estos y otros signos y síntomas pueden ser causados por cáncer de recto u otras afecciones. Consulte a su médico si presenta:
- Sangre en las heces (de color rojo brillante o muy oscura)
- Un cambio en los hábitos intestinales:
- Diarrea
- Constipación
- Sensación de evacuación incompleta del intestino
- Heces más estrechas o con una forma diferente a la habitual
- Malestar abdominal general (dolores frecuentes por gases, hinchazón, sensación de plenitud o calambres ).
- Cambios en el apetito
- weight loss for no known reason
- fatigue
Para diagnosticar el cáncer de recto se utilizan pruebas que examinan el recto y el colon.
In addition to asking about your personal and family health history and doing a physical exam, your doctor may perform the following tests and procedures:
- El tacto rectal digital (TRD) es un examen del recto. El médico o la enfermera introduce un dedo enguantado y lubricado en la parte inferior del recto para palpar si hay bultos o cualquier otra anomalía. En las mujeres, también se puede examinar la vagina .
- Colonoscopia Es un procedimiento que utiliza un colonoscopio para examinar el interior del recto y el colon en busca de pólipos (pequeñas protuberancias de tejido), áreas anormales o cáncer. Un colonoscopio es un instrumento delgado, con forma de tubo, que cuenta con una luz y una lente para la visualización. También puede incluir un instrumento para extraer pólipos o muestras de tejido, que se examinan al microscopio para detectar signos de cáncer.
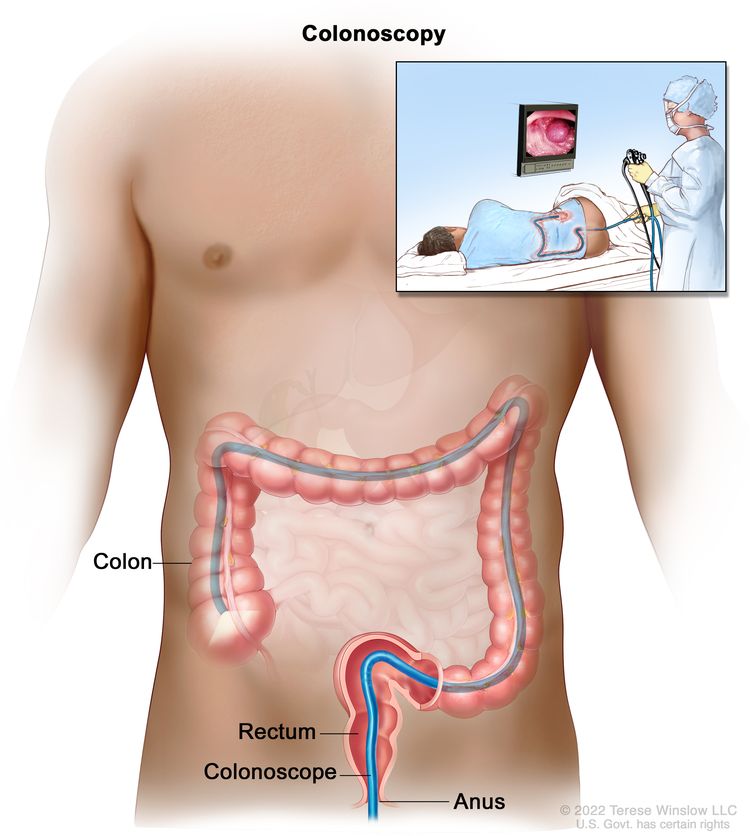
Colonoscopia. Se inserta un tubo delgado y con luz a través del ano y el recto hasta el colon para buscar áreas anómalas.
- La biopsia consiste en la extracción de células o tejidos para su observación al microscopio y la detección de signos de cáncer. El tejido tumoral extraído durante la biopsia puede analizarse para determinar si el paciente presenta la mutación genética causante del síndrome de Lynch (también conocido como cáncer colorrectal hereditario no polipósico). Esto puede ayudar a planificar el tratamiento. Para obtener más información sobre el tipo de datos que puede incluir el informe del patólogo acerca de las células o el tejido extraído durante una biopsia, visite Informes de Patología .
- La inmunohistoquímica es una prueba de laboratorio que utiliza anticuerpos para detectar ciertos antígenos ( marcadores ) en una muestra de tejido del paciente. Los anticuerpos suelen estar unidos a una enzima o a un colorante fluorescente. Tras la unión de los anticuerpos a un antígeno específico en la muestra de tejido, la enzima o el colorante se activan, permitiendo visualizar el antígeno al microscopio. Este tipo de prueba se utiliza para ayudar a diagnosticar el cáncer y diferenciar un tipo de cáncer de otro.
- La inestabilidad de microsatélites (MSI) es una prueba de laboratorio que analiza el tejido tumoral en busca de células que puedan presentar defectos en los genes implicados en la reparación del ADN . Los resultados pueden indicar si el paciente padece un tipo de cáncer asociado a un síndrome de cáncer hereditario, como el síndrome de Lynch.
Una vez que se ha confirmado el diagnóstico de cáncer de recto, se realizan pruebas de imágenes para determinar si las células cancerosas se han diseminado dentro del recto o a otras partes del cuerpo.
El proceso que se utiliza para determinar si el cáncer se ha diseminado dentro del recto o a otras partes del cuerpo se denomina estadificación . La información obtenida durante la estadificación determina la etapa de la enfermedad. Es importante conocer la etapa para planificar el tratamiento.
En el proceso de estadificación pueden utilizarse las siguientes pruebas y procedimientos:
- Chest x-ray is a type of radiation that can go through the body and make pictures of the organs and bones inside the chest.
- La tomografía computarizada (TC) utiliza una computadora conectada a un equipo de rayos X para generar imágenes detalladas de áreas internas del cuerpo, como el abdomen, la pelvis o el tórax. Las imágenes se toman desde diferentes ángulos y se utilizan para crear vistas tridimensionales de los tejidos y órganos. Se puede inyectar un contraste en una vena o ingerirlo para que los órganos o tejidos se visualicen con mayor claridad. Este procedimiento también se conoce como tomografía computarizada o tomografía axial computarizada.
- La resonancia magnética ( RM ) utiliza un imán, ondas de radio y una computadora para generar imágenes detalladas del interior del recto. Se inyecta gadolinio al paciente por vía intravenosa. El gadolinio se acumula alrededor de las células cancerosas, lo que hace que se vean más brillantes en la imagen. Este procedimiento también se conoce como resonancia magnética nuclear (RMN).
- La tomografía por emisión de positrones ( PET ) utiliza una pequeña cantidad de glucosa (un tipo de azúcar radiactiva) que se inyecta en una vena. Un escáner gira alrededor del cuerpo para crear imágenes computarizadas detalladas de las áreas internas donde se absorbe la glucosa. Dado que las células cancerosas suelen absorber más glucosa que las células normales, estas imágenes pueden utilizarse para detectar células cancerosas en el organismo.
- La ecografía endorrectal se utiliza para examinar el recto y los órganos cercanos. Se introduce un transductor de ultrasonido (sonda) en el recto, que emite ondas sonoras de alta energía ( ultrasonido ) que rebotan en los tejidos u órganos internos y producen ecos. Estos ecos forman una imagen de los tejidos corporales llamada ecografía . El médico puede identificar tumores observando la ecografía. Este procedimiento también se conoce como ecografía transrectal.
- El análisis del antígeno carcinoembrionario (ACE) es una prueba que mide el nivel de ACE en la sangre. Esta sustancia es liberada por células cancerosas y normales, pero cuando sus niveles están por encima de lo habitual, puede ser un indicador de cáncer de recto u otras afecciones.
Some people decide to get a second opinion.
Es posible que desee obtener una segunda opinión para confirmar su diagnóstico de cáncer de recto y su plan de tratamiento. Si busca una segunda opinión, deberá obtener los resultados de las pruebas médicas y los informes del primer médico para compartirlos con el segundo especialista. El segundo médico revisará el informe patológico, las diapositivas y las exploraciones. Es posible que esté de acuerdo con el primer médico, sugiera cambios en el plan de tratamiento, proponga otro enfoque terapéutico o le ofrezca más información sobre su cáncer.
Para obtener más información sobre cómo elegir un médico y obtener una segunda opinión, visite la sección «Cómo encontrar atención oncológica» . Puede comunicarse con el Servicio de Información Oncológica del NCI por chat, correo electrónico o teléfono (en inglés y español) para obtener ayuda para encontrar un médico, un hospital o una segunda opinión. Para preguntas que pueda hacer durante sus citas, visite la sección «Preguntas para hacerle a su médico sobre el cáncer» .
Certain factors affect prognosis (chance of recovery) and treatment options.
El pronóstico y las opciones de tratamiento dependen de:
- la etapa del cáncer (si afecta solo al revestimiento interno del recto, si afecta a todo el recto o si se ha extendido a los ganglios linfáticos, órganos cercanos u otras partes del cuerpo)
- Si el cáncer está relacionado con defectos en los genes encargados de la reparación del ADN
- Si el tumor se ha diseminado, ya sea dentro de la pared intestinal o más allá de ella
- La ubicación del cáncer dentro del recto
- Si hay obstrucción o perforación del intestino
- Si se puede extirpar todo el tumor mediante cirugía
- el estado de salud general del paciente
- Si el cáncer se ha diagnosticado recientemente o si ha reaparecido (regresado)
Estadios del cáncer de recto
Puntos clave
- Para clasificar el cáncer de recto se utilizan los siguientes estadios:
- Estadio 0 (carcinoma in situ)
- Cáncer de recto en estadio I (también llamado estadio 1)
- Cáncer de recto en estadio II (también llamado estadio 2)
- Cáncer de recto en estadio III (también llamado estadio 3)
- Cáncer de recto en estadio IV (también llamado estadio 4)
- El cáncer de recto puede reaparecer (regresar) después de haber sido tratado.
La etapa del cáncer describe la extensión del cáncer en el cuerpo, como el tamaño del tumor, si se ha diseminado y hasta dónde se ha extendido desde donde se formó inicialmente.
Existen varios sistemas de estadificación para el cáncer que describen su extensión. La estadificación del cáncer rectal generalmente utiliza el sistema TNM . Este sistema puede describirse en su informe de patología. Según los resultados del TNM, se asigna una etapa (I, II, III o IV, también escritas como 1, 2, 3 o 4) a su cáncer. Al hablar con usted sobre su diagnóstico, su médico podría describir el cáncer como una de estas etapas.
Infórmese sobre las pruebas para la estadificación del cáncer de recto . Obtenga más información sobre la estadificación del cáncer .
Para clasificar el cáncer de recto se utilizan los siguientes estadios:
Estadio 0 (carcinoma in situ)
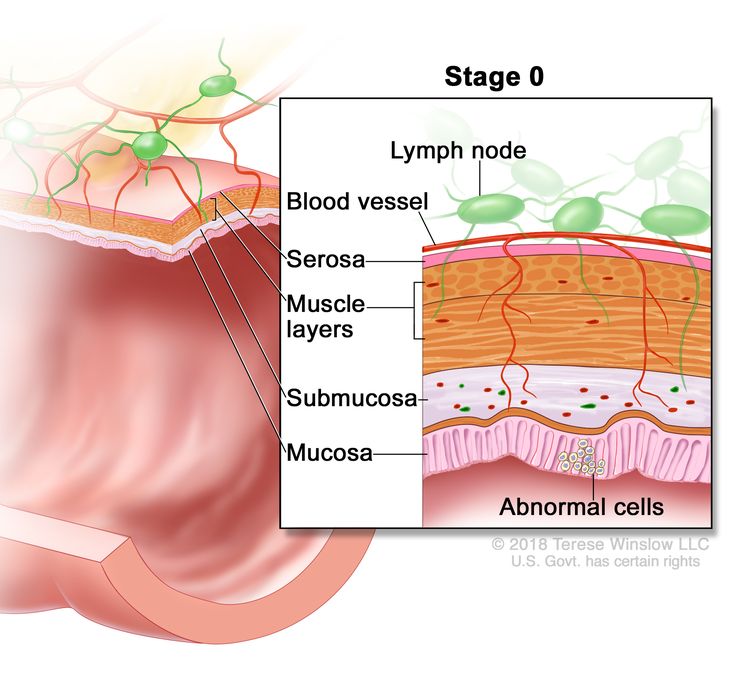
Estadio 0 (carcinoma rectal in situ). Se muestran células anómalas en la mucosa de la pared del recto.
En el cáncer de recto en estadio 0, se encuentran células anormales en la mucosa (capa más interna) de la pared rectal. Estas células anormales pueden convertirse en cáncer y extenderse al tejido normal circundante. El estadio 0 también se conoce como carcinoma in situ.
Cáncer de recto en estadio I (también llamado estadio 1)
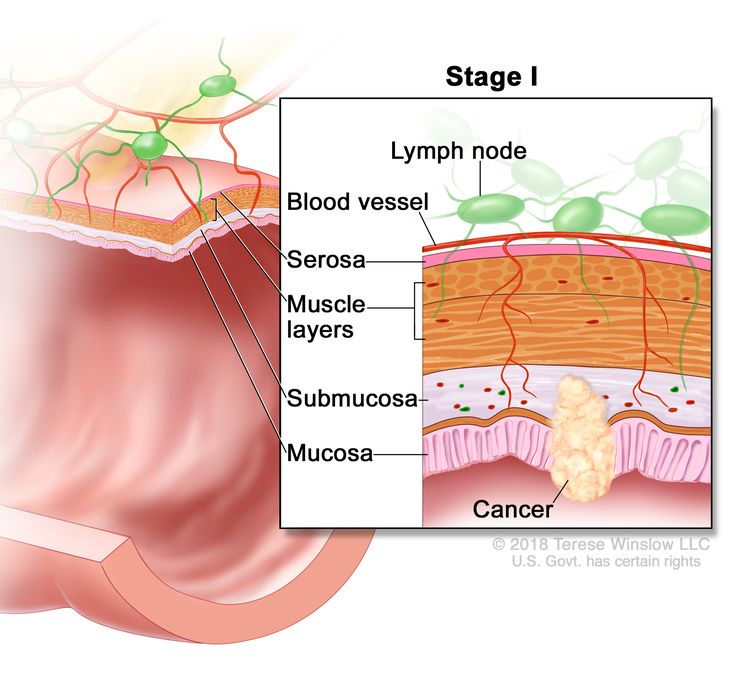
Cáncer de recto en estadio I. El cáncer se ha extendido desde la mucosa de la pared del recto hasta la submucosa o la capa muscular.
En el cáncer de recto en estadio I, el cáncer se formó en la mucosa, la capa más interna de la pared del recto, y se ha extendido a la submucosa, la capa de tejido adyacente a la mucosa) o a la capa muscular de la pared del recto.
Cáncer de recto en estadio II (también llamado estadio 2)
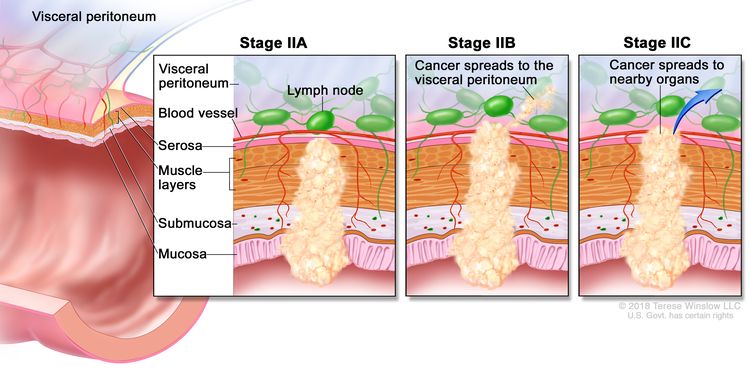
Cáncer de recto en estadio II. En el estadio IIA, el cáncer se ha extendido a través de la capa muscular de la pared del recto hasta la serosa. En el estadio IIB, el cáncer se ha extendido a través de la serosa, pero no a los órganos cercanos. En el estadio IIC, el cáncer se ha extendido a través de la serosa a los órganos cercanos.
El cáncer de recto en estadio II se divide en los estadios IIA, IIB y IIC.
- Estadio IIA: el cáncer se ha extendido a través de la capa muscular de la pared del recto hasta la serosa, la capa más externa de la pared del recto.
- Estadio IIB: el cáncer se ha extendido a través de la serosa, la capa más externa de la pared del recto, hasta el tejido que recubre los órganos del abdomen (peritoneo visceral).
- Estadio IIC: el cáncer se ha extendido a través de la serosa, la capa más externa de la pared del recto, hasta los órganos cercanos.
Cáncer de recto en estadio III (también llamado estadio 3)
El cáncer de recto en estadio III se divide en los estadios IIIA, IIIB y IIIC.
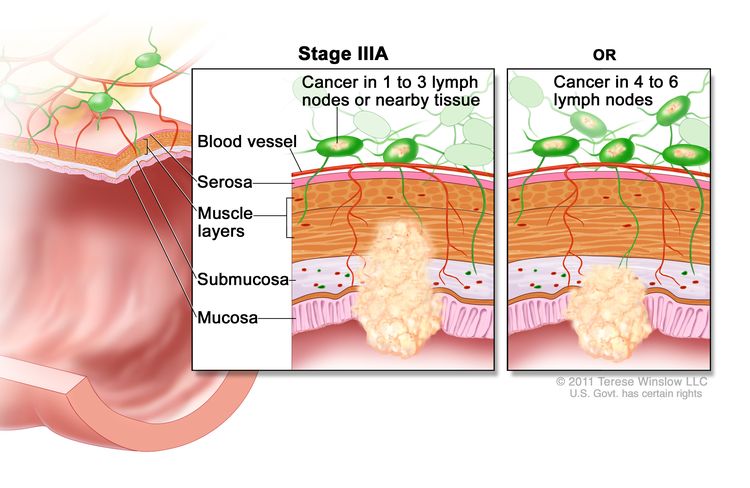
Cáncer de recto en estadio IIIA. El cáncer se ha extendido a través de la mucosa de la pared del recto hasta la submucosa y, posiblemente, a la capa muscular. También puede haberse extendido a uno o tres ganglios linfáticos cercanos o a los tejidos adyacentes a los ganglios linfáticos. En otro caso, el cáncer se ha extendido a través de la mucosa hasta la submucosa y ha alcanzado cuatro a seis ganglios linfáticos cercanos.
En el estadio IIIA, el cáncer se ha extendido de una de las siguientes maneras:
- a través de la mucosa (capa más interna) de la pared rectal hasta la submucosa (capa de tejido adyacente a la mucosa) o hasta la capa muscular de la pared rectal. El cáncer se ha diseminado a uno o tres ganglios linfáticos cercanos, o se han formado células cancerosas en el tejido cercano a los ganglios linfáticos; o
- A través de la mucosa, la capa más interna de la pared del recto, hasta la submucosa, la capa de tejido próxima a la mucosa. El cáncer se ha extendido de cuatro a seis ganglios linfáticos cercanos.
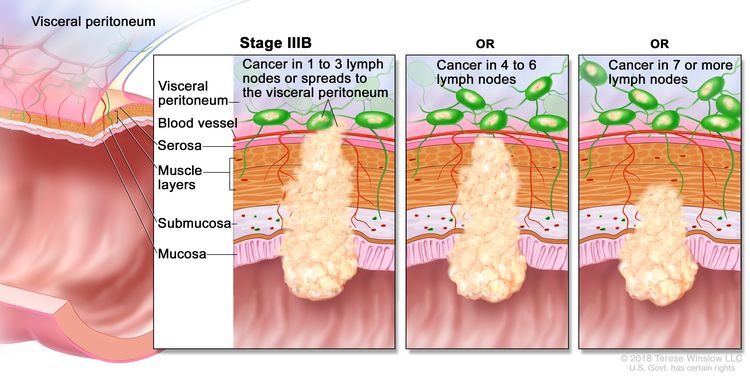
Cáncer de recto en estadio IIIB. El cáncer se ha extendido a través de la capa muscular de la pared del recto hasta la serosa, o se ha extendido a través de la serosa sin llegar a los órganos cercanos. También se ha extendido a uno a tres ganglios linfáticos cercanos o a los tejidos adyacentes a los ganglios linfáticos. Otra posibilidad es que el cáncer se haya extendido a la capa muscular o la serosa, afectando a entre cuatro y seis ganglios linfáticos cercanos. En un tercer escenario, el cáncer ha avanzado desde la mucosa hasta la submucosa, y posiblemente hasta la capa muscular, diseminándose a siete o más ganglios linfáticos cercanos.
En el estadio IIIB, el cáncer se ha extendido de una de las siguientes maneras:
- a través de la capa muscular de la pared rectal hasta la serosa (capa más externa) de la pared rectal o se ha extendido a través de la serosa hasta el tejido que recubre los órganos del abdomen (peritoneo visceral). El cáncer se ha extendido a uno o tres ganglios linfáticos cercanos, o se han formado células cancerosas en el tejido cercano a los ganglios linfáticos; o
- A la capa muscular o a la serosa, la capa más externa de la pared del recto. El cáncer se ha extendido a entre cuatro y seis ganglios linfáticos cercanos.
- A través de la mucosa, la capa más interna de la pared del recto hasta la submucosa, la capa de tejido próxima a la mucosa, o hasta la capa muscular de la pared del recto. El cáncer se ha extendido a siete o más ganglios linfáticos cercanos.
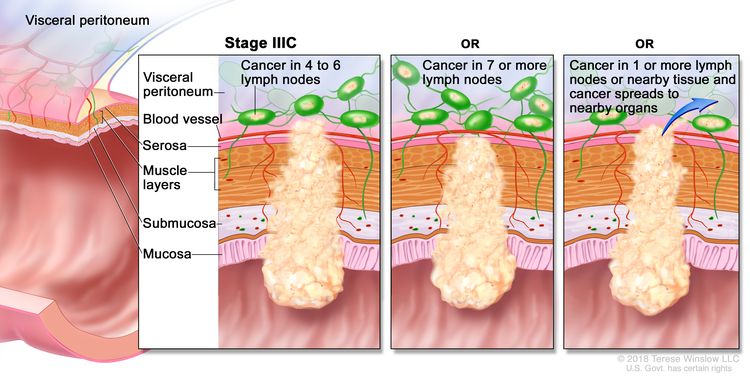
Cáncer de recto en estadio IIIC. El cáncer se ha extendido a través de la serosa de la pared del recto, pero no ha alcanzado los órganos cercanos; además, se ha extendido a entre cuatro y seis ganglios linfáticos cercanos. Otra posibilidad es que el cáncer se haya extendido desde la capa muscular hasta la serosa, o haya atravesado la serosa sin afectar los órganos cercanos, diseminándose a siete o más ganglios linfáticos cercanos. O bien, el cáncer se ha extendido a través de la serosa y ha alcanzado órganos cercanos, además de alcanzar a uno o más ganglios linfáticos cercanos o a los tejidos próximos a los ganglios linfáticos.
En el estadio IIIC, el cáncer se ha extendido de una de las siguientes maneras:
- a través de la serosa (capa más externa) de la pared del recto hasta el tejido que recubre los órganos del abdomen (peritoneo visceral). El cáncer se ha diseminado a cuatro o seis ganglios linfáticos cercanos; o
- A través de la capa muscular de la pared del recto hasta la serosa, la capa más externa de la pared del recto o se ha extendido a través de la serosa hasta el tejido que recubre los órganos del abdomen (peritoneo visceral). El cáncer se ha extendido a siete o más ganglios linfáticos cercanos.
- A través de la serosa, la capa más externa de la pared del recto hasta los órganos cercanos. El cáncer se ha extendido a uno o más ganglios linfáticos cercanos, o se han formado células cancerosas en el tejido cerca de los ganglios linfáticos.
Cáncer de recto en estadio IV (también llamado estadio 4)
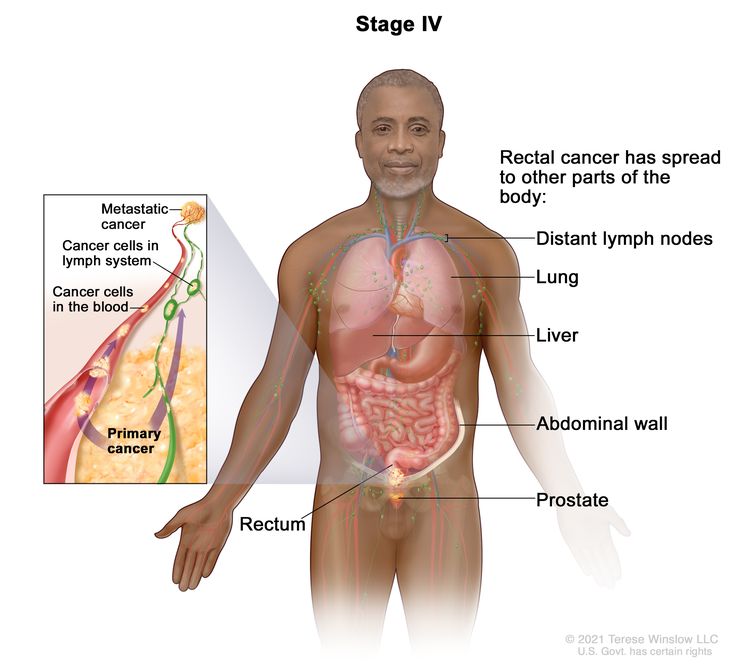
Cáncer de recto en estadio IV. El cáncer se ha extendido a través de la sangre y los ganglios linfáticos a otras partes del cuerpo, como los pulmones, el hígado, la pared abdominal o la próstata.
El cáncer de recto en estadio IV se divide en los estadios IVA, IVB y IVC.
- Estadio IVA: El cáncer se ha extendido a una zona u órgano que no está cerca del recto, como el hígado, el pulmón, la próstata o un ganglio linfático distante.
- Estadio IVB: el cáncer se ha extendido a más de un área u órgano alejado del recto, como el hígado, el pulmón, la próstata o un ganglio linfático distante.
- Estadio IVC: el cáncer se ha extendido al tejido que recubre la pared del abdomen y puede haberse extendido a otras áreas u órganos.
El cáncer de recto en estadio IV también se conoce como cáncer de recto metastásico. Este tipo de cáncer se da cuando las células cancerosas viajan a través del sistema linfático o el torrente sanguíneo, formando tumores en otras partes del cuerpo. El tumor metastásico es el mismo tipo de cáncer que el tumor primario. Por ejemplo, si el cáncer de recto se propaga al hígado, las células cancerosas del hígado siguen siendo células cancerosas de recto, por lo que la enfermedad se denomina cáncer de recto metastásico y no cáncer de hígado. Obtenga más información en Cáncer metastásico: cuando el cáncer se disemina.
El cáncer de recto puede reaparecer (regresar) después de haber sido tratado.
El cáncer rectal recurrente es aquel que reaparece después de haber sido tratado. Si el cáncer rectal reaparece, puede hacerlo en el recto o en otras partes del cuerpo, como el colon, la pelvis, el hígado o los pulmones. Se realizarán pruebas para determinar la ubicación de la recidiva. El tipo de tratamiento para el cáncer rectal recurrente dependerá de la localización de la recidiva.
Learn more in Recurrent Cancer: When Cancer Comes Back.
Treatment Option Overview
Puntos clave
- Existen diferentes tipos de tratamiento para las personas con cáncer de recto.
- The following types of treatment are used:
- Cirugía
- Radioterapia
- Quimioterapia
- Chemoradiation therapy
- Vigilancia activa
- Terapia dirigida
- Inmunoterapia
- New types of treatment are being tested in clinical trials.
- El tratamiento para el cáncer de recto puede causar efectos secundarios.
- Es posible que se necesiten cuidados de seguimiento.
Existen diferentes tipos de tratamiento para las personas con cáncer de recto.
Existen diferentes tipos de tratamientos para el cáncer de recto. Usted y su equipo de atención oncológica trabajarán juntos para definir su plan de tratamiento, que puede incluir más de un tipo de tratamiento. Se tendrán en cuenta muchos factores, como el estadio del cáncer, su estado de salud general y sus preferencias. Su plan incluirá información sobre su cáncer, los objetivos del tratamiento, las opciones de tratamiento disponibles, los posibles efectos secundarios y la duración prevista del tratamiento.
Hablar con tu equipo de atención oncológica antes de que comience el tratamiento sobre qué esperar te será de gran ayuda. Es importante que sepas qué debes hacer antes de que empiece el tratamiento, cómo te sentirás durante el mismo y qué tipo de ayuda necesitarás. Para obtener más información, visita la sección Preguntas para hacerle a tu médico sobre el tratamiento .
The following types of treatment are used:
Cirugía
La cirugía es el tratamiento más común para todos los estadios del cáncer de recto. El cáncer se extirpa mediante uno de los siguientes tipos de cirugía:
- Polipectomía: Si el cáncer se encuentra en un pólipo (un pequeño trozo de tejido abultado), a menudo se extirpa el pólipo durante una colonoscopia .
- Escisión local: si el cáncer está en la superficie interna del recto y no se ha extendido a la pared del recto, se extirpa junto con una pequeña cantidad de tejido sano circundante.
- Resección: Si el cáncer se ha extendido a la pared del recto, se extirpa la sección afectada y el tejido sano circundante. En ocasiones, también se extirpa el tejido entre el recto y la pared abdominal. Se extirpan los ganglios linfáticos cercanos al recto y se examinan al microscopio para detectar signos de cáncer.
- Ablación por radiofrecuencia: Consiste en el uso de una sonda especial con electrodos diminutos que destruyen las células cancerosas. En ocasiones, la sonda se inserta directamente a través de la piel y solo se requiere anestesia local . En otros casos, se inserta mediante una incisión en el abdomen . Este procedimiento se realiza en el hospital con anestesia general .
- Criocirugía: Tratamiento que utiliza un instrumento para congelar y destruir tejido anormal . Este tipo de tratamiento también se conoce como crioterapia. Obtenga más información sobre la criocirugía para el tratamiento del cáncer .
- Exenteración pélvica: Si el cáncer se ha extendido a otros órganos cercanos al recto, se extirpan la parte inferior del colon, el recto y la vejiga . En las mujeres, se pueden extirpar el cuello uterino, la vagina, los ovarios y los ganglios linfáticos cercanos. En los hombres, se puede extirpar la próstata . Se crean aberturas artificiales ( estomas ) para que la orina y las heces fluyan del cuerpo hacia una bolsa recolectora.
Después de extirpar el cáncer, el cirujano hará lo siguiente:
- Una anastomosis, que consiste en coser las partes sanas del recto, unir el recto restante al colon o conectar el colon al ano);
o
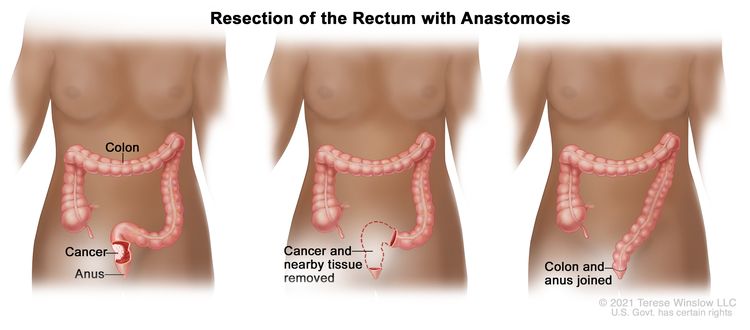
Resección del recto con anastomosis. Se extirpan el recto y parte del colon, y posteriormente se unen el colon y el ano.
- Se crea un estoma (una abertura) desde el recto hacia el exterior del cuerpo para que las heces salgan. Este procedimiento se realiza si el cáncer está muy cerca del ano y se denomina colostomía . Se coloca una bolsa alrededor del estoma para recoger las heces. A veces, la colostomía solo es necesaria hasta que el recto haya cicatrizado, y luego se puede revertir. Sin embargo, si se extirpa todo el recto, la colostomía puede ser permanente.
La radioterapia y/o la quimioterapia pueden administrarse antes de la cirugía para reducir el tamaño del tumor, facilitar la extirpación del cáncer y ayudar con el control intestinal después de la cirugía. El tratamiento administrado antes de la cirugía se denomina terapia neoadyuvante . Después de extirpar todo el cáncer visible durante la cirugía, algunos pacientes pueden recibir radioterapia y/o quimioterapia después de la cirugía para eliminar las células cancerosas restantes. El tratamiento administrado después de la cirugía, para disminuir el riesgo de que el cáncer reaparezca, se denomina terapia adyuvante .
Si el cáncer se ha extendido al hígado y no puede extirparse mediante cirugía convencional, se puede realizar una hepatectomía total seguida de un trasplante de hígado después de la quimioterapia. La hepatectomía total y el trasplante de hígado implican la extirpación completa del hígado mediante cirugía, seguida del trasplante de un hígado sano proveniente de un donante.
Radioterapia
La radioterapia utiliza rayos X de alta energía u otros tipos de radiación para destruir las células cancerosas o impedir su crecimiento. El cáncer de recto a veces se trata con radioterapia externa . Este tipo de radioterapia utiliza una máquina externa al cuerpo para enviar radiación hacia la zona afectada por el cáncer.
La radioterapia preoperatoria de corta duración se utiliza en algunos tipos de cáncer de recto. Este tipo de radioterapia externa utiliza dosis de radiación más bajas y en menor cantidad que el tratamiento estándar, seguida de cirugía varios días después de la última dosis.
Learn more about External Beam Radiation Therapy for Cancer and Radiation Therapy Side Effects.
Quimioterapia
Chemotherapy (also called chemo) uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing.
La quimioterapia sistémica consiste en la administración oral o intravenosa de fármacos quimioterapéuticos, o bien mediante inyección intramuscular. Al administrarse de esta forma, los fármacos entran en el torrente sanguíneo y pueden llegar a las células cancerosas de todo el cuerpo. La quimioterapia sistémica utilizada para tratar el cáncer de recto incluye:
- capecitabine
- Fluorouracilo (5-FU)
- Irinotecán
- leucovorin (a vitamin that improves the effectiveness of 5-FU)
- oxaliplatin
- Trifluridina y tipiracilo
Combinations of these drugs may be used. Other chemotherapy drugs not listed here may also be used.
La quimioterapia también puede combinarse con otros tipos de fármacos. Por ejemplo, podría combinarse con los fármacos de terapia dirigida bevacizumab, cetuximab o panitumumab .
La quimioterapia regional para el cáncer de recto consiste en la administración de fármacos directamente en la arteria hepática (la arteria principal que irriga el hígado) mediante un procedimiento llamado quimioembolización. La quimioembolización de la arteria hepática puede utilizarse para tratar el cáncer que se ha diseminado al hígado . Esto se logra bloqueando la arteria hepática e inyectando fármacos anticancerígenos entre el bloqueo y el hígado. Las arterias hepáticas transportan entonces los fármacos al hígado. Solo una pequeña cantidad del fármaco llega a otras partes del cuerpo. El bloqueo puede ser temporal o permanente, según el método utilizado para bloquear la arteria. El hígado continúa recibiendo algo de sangre de la vena porta hepática, que transporta sangre desde el estómago y el intestino .
La forma en que se administra la quimioterapia depende del tipo y estadio del cáncer que se esté tratando.
Para obtener más información sobre cómo funciona la quimioterapia, cómo se administra, los efectos secundarios comunes y mucho más, visite Quimioterapia para tratar el cáncer y Quimioterapia y usted: Apoyo para personas con cáncer .
Chemoradiation therapy
Chemoradiation therapy combines chemotherapy and radiation therapy to increase the effects of both.
Vigilancia activa
La vigilancia activa consiste en seguir de cerca el estado del paciente sin aplicar ningún tratamiento, a menos que haya cambios en los resultados de las pruebas. Se utiliza para identificar signos tempranos de que la enfermedad está empeorando. En la vigilancia activa, a los pacientes se les realizan ciertos exámenes y pruebas para verificar si el cáncer está creciendo. Cuando el cáncer empieza a crecer, se administra un tratamiento para curar el cáncer. Las pruebas incluyen:
Terapia dirigida
Targeted therapy uses drugs or other substances to identify and attack specific cancer cells. Your doctor may suggest biomarker tests to help predict your response to certain targeted therapy drugs. Learn more about Biomarker Testing for Cancer Treatment.
Las terapias dirigidas utilizadas para tratar el cáncer de recto incluyen:
Obtenga más información en Terapia dirigida para tratar el cáncer.
Inmunoterapia
Immunotherapy helps a person's immune system fight cancer. Your doctor may suggest biomarker tests to help predict your response to certain immunotherapy drugs. Learn more about Biomarker Testing for Cancer Treatment.
Los medicamentos de inmunoterapia utilizados para tratar el cáncer de recto son:
Obtenga más información sobre la inmunoterapia para el tratamiento del cáncer .
New types of treatment are being tested in clinical trials.
For some people, joining a clinical trial may be an option. There are different types of clinical trials for people with cancer. For example, a treatment trial tests new treatments or new ways of using current treatments. Supportive care and palliative care trials look at ways to improve quality of life, especially for those who have side effects from cancer and its treatment.
You can use the clinical trial search to find NCI-supported cancer clinical trials accepting participants. The search allows you to filter trials based on the type of cancer, your age, and where the trials are being done. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Para más información sobre ensayos clínicos, cómo encontrarlos y participar en uno de ellos, visite la web Información sobre estudios clínicos para pacientes y cuidadores.
El tratamiento para el cáncer de recto puede causar efectos secundarios.
For information about side effects caused by treatment for cancer, visit our Side Effects page.
Es posible que se necesiten cuidados de seguimiento.
A medida que avanza el tratamiento, se le realizarán pruebas o controles de seguimiento. Es posible que se repitan algunas pruebas para diagnosticar o estadificar el cáncer con el fin de evaluar cómo está funcionando el tratamiento. Las decisiones sobre si continuar, modificar o suspender el tratamiento pueden basarse en los resultados de estas pruebas.
Algunas pruebas seguirán realizándose de manera periódica después de terminar el tratamiento. Los resultados pueden indicar si su afección ha cambiado o si el cáncer ha redicivado (regresado).
Después del tratamiento para el cáncer de recto, se puede realizar un análisis de sangre para medir los niveles de antígeno carcinoembrionario. Esta sustancia puede aumentar en presencia de cáncer, por lo que su evaluación ayuda a determinar si la enfermedad ha reaparecido.
Treatment of Stage 0 (carcinoma in situ)
El tratamiento de la etapa 0 puede incluir los siguientes tipos de cirugía:
- Polipectomía simple
- Local escisión
- Resección (cuando el tumor es demasiado grande para extirparlo mediante escisión local)
Learn more about these treatments in the Treatment Option Overview.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del cáncer de recto en estadio I
El tratamiento del cáncer de recto en estadio I puede incluir:
- Local escisión
- Resección
- resección con radioterapia y quimioterapia después de la cirugía
Learn more about these treatments in the Treatment Option Overview.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del cáncer de recto en estadios II y III
El tratamiento del cáncer de recto en estadio II y estadio III puede incluir:
- Quimiorradiación seguida de cirugía
- Quimioterapia sola seguida de cirugía, para personas con enfermedad de menor riesgo
- Radioterapia de corta duración seguida de cirugía y quimioterapia
- Cirugía seguida de quimiorradiación
- Cirugía
- Quimiorradiación seguida de vigilancia activa y posiblemente cirugía si el cáncer reaparece (vuelve).
- Inmunoterapia con dostarlimab (para el tratamiento de tumores que pueden presentar un defecto en los genes implicados en la reparación del ADN )
Learn more about these treatments in the Treatment Option Overview.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del cáncer de recto en estadio IV y recurrente
El tratamiento del cáncer de recto en estadio IV y recurrente puede incluir:
- cirugía con o sin quimioterapia o radioterapia
- quimioterapia sistémica con o sin terapia dirigida ( bevacizumab, fruquintinib, panitumumab, ramucirumab, regorafenib o ziv-aflibercept )
- quimioterapia sistémica con o sin inmunoterapia con dostarlimab (para el tratamiento de tumores que pueden tener un defecto en los genes implicados en la reparación del ADN ), nivolumab o pembrolizumab.
- Quimioterapia para controlar el crecimiento del tumor
- radioterapia, quimioterapia o una combinación de ambas, como terapia paliativa para aliviar los síntomas y mejorar la calidad de vida.
- Colocación de un stent para mantener abierto el recto abierto en caso de obstrucción parcial por un tumor, como terapia paliativa para aliviar los síntomas y mejorar la calidad de vida del paciente
- Terapia dirigida con encorafenib y cetuximab en pacientes con una determinada alteración en el gen BRAF.
- Inmunoterapia (nivolumab o pembrolizumab, o nivolumab e ipilimumab combinados)
El tratamiento del cáncer de recto que se ha diseminado a otros órganos dependerá del órgano afectado y la extensión de la enfermedad.
- El tratamiento para áreas de cáncer diseminadas al hígado puede incluir:
- Quimioterapia para reducir el tamaño del tumor, si es necesario, seguida de cirugía
- criocirugía o ablación por radiofrecuencia
- Quimioembolización y/o quimioterapia sistémica
- Trasplante de hígado después de la quimioterapia para pacientes con metástasis hepáticas que no se pueden extirpar mediante cirugía
- Un ensayo clínico de quimioembolización combinada con radioterapia para los tumores en el hígado
Learn more about these treatments in the Treatment Option Overview.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Más información sobre el cáncer de recto
Para obtener más información del Instituto Nacional del Cáncer sobre el cáncer de recto, visite:
- Página principal sobre el cáncer colorrectal
- Exámenes para detectar el cáncer colorrectal y los pólipos
- Medicamentos aprobados para el cáncer de colon y de recto
- Pruebas genéticas para detectar el riesgo de cáncer hereditario
For general cancer information and other resources from the National Cancer Institute, visit:
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen del PDQ sobre el cáncer contiene información actualizada del tratamiento del cáncer de recto. El propósito es informar y ayudar a los pacientes, sus familiares y cuidadores. No da pautas ni recomendaciones formales para tomar decisiones relacionadas con la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre el tratamiento de adultos de PDQ®. Tratamiento del cáncer de recto (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Actualizado:
URL de origen: https://www.cancer.gov/node/4214/syndication
Agencia de origen: National Cancer Institute (NCI)
Fecha de captura: 2013-09-14 09:02:05.0