








Tratamiento del cáncer de endometrio
Access exceptional care for endometrial cancer and other types of gynecologic cancers at Montefiore Einstein Comprehensive Cancer Center. Our multidisciplinary team has extensive experience caring for this cancer. As one of the first NCI-designated cancer centers, for more than 50 years, we’ve been a leader in the research, diagnosis and treatment of over 200 types of cancer.
We’re at the forefront of treatment and research for endometrial cancer and other gynecologic cancers. We deliver comprehensive treatment plans individualized to our patients’ needs. At Montefiore Einstein Comprehensive Cancer Center, we provide access to leading-edge, innovative care informed by the latest cancer research, as well as the opportunity to enroll in clinical trials.
When you need endometrial cancer care, turn to our providers who are passionate about ending cancer and addressing your whole health needs.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Endometrial Cancer Treatment (PDQ®)–Patient Version
General Information About Endometrial Cancer
Puntos clave
- Endometrial cancer is a disease in which malignant (cancer) cells form in the tissues of the endometrium.
- Obesity and having metabolic syndrome may increase the risk of endometrial cancer.
- Taking tamoxifen for breast cancer or taking estrogen alone (without progesterone) can increase the risk of endometrial cancer.
- Signs and symptoms of endometrial cancer include unusual vaginal bleeding or pain in the pelvis.
- Tests that examine the endometrium are used to diagnose endometrial cancer.
- Certain factors affect prognosis (chance of recovery) and treatment options.
Endometrial cancer is a disease in which malignant (cancer) cells form in the tissues of the endometrium.
The endometrium is the lining of the uterus, a hollow, muscular organ in a woman’s pelvis. The uterus is where a fetus grows. In most nonpregnant women, the uterus is about 3 inches long. The lower, narrow end of the uterus is the cervix, which leads to the vagina.
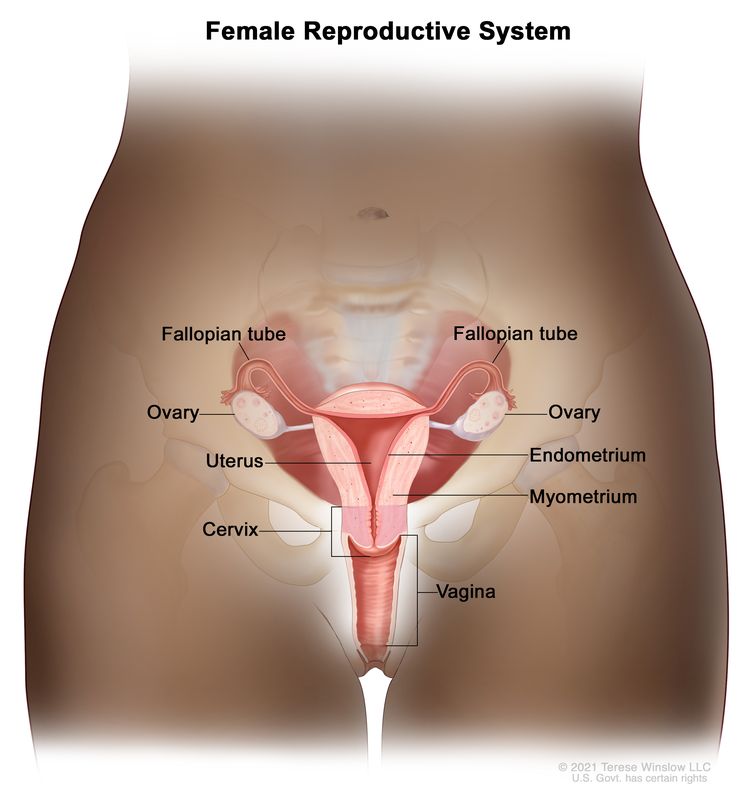
Anatomía del aparato reproductor femenino. Entre los órganos del aparato reproductor femenino están el útero, los ovarios, las trompas de Falopio, el cuello uterino y la vagina. El útero tiene una capa muscular externa, llamada miometrio, y una capa de tejido interno que lo reviste, llamada endometrio.
Cancer of the endometrium is different from cancer of the muscle of the uterus, which is called sarcoma of the uterus. See the PDQ summary on Uterine Sarcoma Treatment for more information about uterine sarcoma.
Obesity and having metabolic syndrome may increase the risk of endometrial cancer.
Anything that increases your chance of getting a disease is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn't mean that you will not get cancer. Talk to your doctor if you think you may be at risk for endometrial cancer.
Risk factors for endometrial cancer include the following:
- Taking estrogen-only hormone replacement therapy (HRT) after menopause.
- Taking tamoxifen to prevent or treat breast cancer.
- Obesidad.
- Having metabolic syndrome.
- Having type 2 diabetes.
- Exposure of endometrial tejidos hacia el estrogen made by the body. This may be caused by:
- Never giving birth.
- Menstruating at an early age.
- Starting menopause at a later age.
- Having polycystic ovary syndrome.
- Having a family history of endometrial cancer in a first-degree relative (mother, sister, or daughter).
- Having certain genetic conditions, such as Lynch syndrome.
- Having endometrial hyperplasia.
La edad avanzada es el principal factor de riesgo para la mayoría de los cánceres. La probabilidad de padecer cáncer aumenta con la edad.
Taking tamoxifen for breast cancer or taking estrogen alone (without progesterone) can increase the risk of endometrial cancer.
Endometrial cancer may develop in breast cancer patients who have been treated with tamoxifen. A patient who takes this drug and has abnormal vaginal bleeding should have a follow-up exam and a biopsy of the endometrial lining if needed. Women taking estrogen (a hormone that can affect the growth of some cancers) alone also have an increased risk of endometrial cancer. Taking estrogen combined with progesterone (another hormone) does not increase a woman’s risk of endometrial cancer.
Signs and symptoms of endometrial cancer include unusual vaginal bleeding or pain in the pelvis.
These and other signs and symptoms may be caused by endometrial cancer or by other conditions. Check with your doctor if you have any of the following:
Tests that examine the endometrium are used to diagnose endometrial cancer.
Because endometrial cancer begins inside the uterus, it does not usually show up in the results of a Pap test. For this reason, a sample of endometrial tissue must be removed and checked under a microscope to look for cancer cells. One of the following procedures may be used:
- Endometrial biopsy: The removal of tissue from the endometrium (inner lining of the uterus) by inserting a thin, flexible tube through the cervix and into the uterus. The tube is used to gently scrape a small amount of tissue from the endometrium and then remove the tissue samples. A pathologist views the tissue under a microscope to look for cancer cells.
- Dilatación y curetaje: A procedure to remove samples of tissue from the inner lining of the uterus. The cervix is dilatado and a cureta (spoon-shaped instrument) is inserted into the uterus to remove tissue. The tissue samples are checked under a microscope for signs of disease. This procedure is also called a D&C.
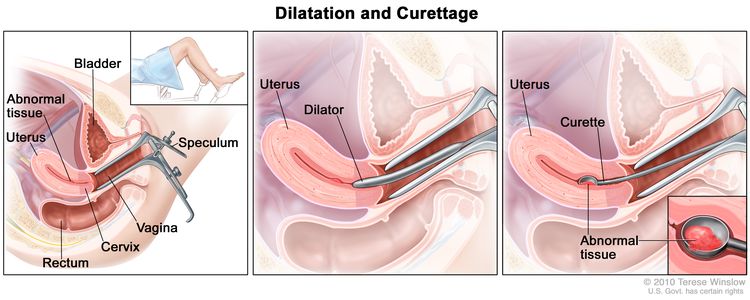
Dilatación y curetaje (D y C). Se inserta un espéculo en la vagina para ensancharla y observar el cuello uterino (primer gráfico). Se utiliza un dilatador para ensanchar el cuello uterino (gráfico del medio). Se coloca una cureta a través del cuello uterino hasta el útero para raspar el tejido anómalo (último gráfico).
- Hysteroscopy: A procedure to look inside the uterus for abnormal areas. A hysteroscope is inserted through the vagina and cervix into the uterus. A hysteroscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove tissue samples, which are checked under a microscope for signs of cancer.
Other tests and procedures used to diagnose endometrial cancer include the following:
- Reconocimiento físico e historial de salud: un examen del cuerpo para evaluar el estado general de salud, incluida la detección de signos de enfermedad, como bultos o cualquier otra anomalía. También se toma nota de los hábitos de salud del paciente y de sus enfermedades y tratamientos previos.
- Transvaginal ultrasound exam: A procedure used to examine the vagina, uterus, trompas de Falopio, and bladder. An ultrasound transducer (probe) is inserted into the vagina and used to bounce high-energy sound waves (ultrasound) off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a ecograma. The doctor can identify tumores by looking at the sonogram.
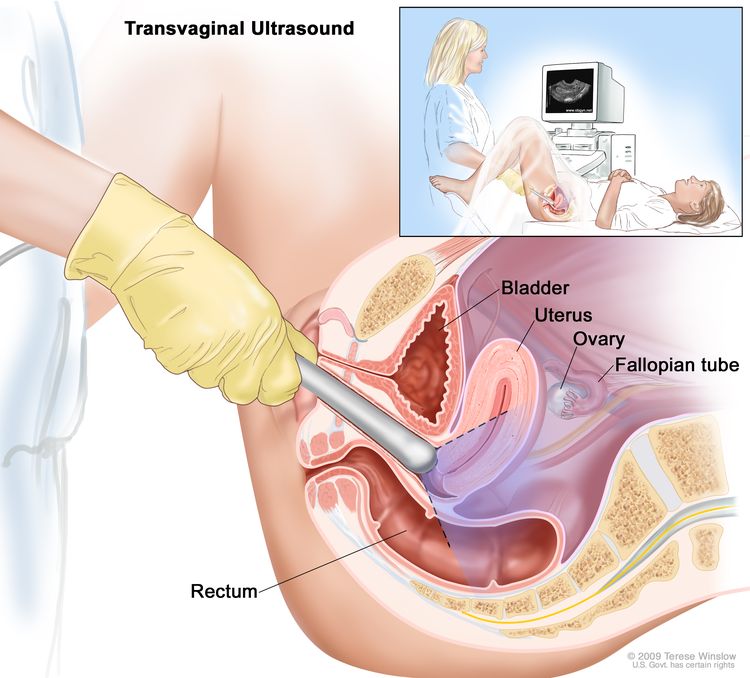
Ecografía transvaginal. Se introduce en la vagina una sonda de ecografía conectada a una computadora y se mueve suavemente para visualizar diferentes órganos. La sonda emite ondas sonoras en los órganos y tejidos internos para generar ecos que forman un ecograma (imagen computarizada).
Certain factors affect prognosis (chance of recovery) and treatment options.
El pronóstico y las opciones de tratamiento dependen de los siguientes factores:
- The stage of the cancer (whether it is in the endometrium only, involves the uterus wall, or has spread to other places in the body).
- How the cancer cells look under a microscope.
- Whether the cancer cells are affected by progesterone.
Endometrial cancer can usually be cured because it is usually diagnosed early.
Stages of Endometrial Cancer
Puntos clave
- After endometrial cancer has been diagnosed, tests are done to find out if cancer cells have spread within the uterus or to other parts of the body.
- There are three ways that cancer spreads in the body.
- El cáncer puede extenderse desde donde comenzó a otras partes del cuerpo.
- The following stages are used for endometrial cancer:
- Estadio I
- Estadio II
- Estadio III
- Estadio IV
- Endometrial cancer may be grouped for treatment as follows:
- Low-risk endometrial cancer
- High-risk endometrial cancer
- Endometrial cancer can recur (come back) after it has been treated.
After endometrial cancer has been diagnosed, tests are done to find out if cancer cells have spread within the uterus or to other parts of the body.
The process used to find out whether the cancer has spread within the uterus or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment. Certain tests and procedures are used in the staging process. A hysterectomy (an operation in which the uterus is removed) will usually be done to treat endometrial cancer. Tissue samples are taken from the area around the uterus and checked under a microscope for signs of cancer to help find out whether the cancer has spread.
The following procedures may be used in the staging process:
- Examen pélvico: An exam of the vagina, cuello uterino, útero, trompas de Falopio, ovarios, and recto. Un espéculo se introduce en la vagina y el médico o enfermero examina la vagina y el cuello uterino en busca de signos de enfermedad. Un Prueba de Papanicolaou del cuello uterino por lo general se hace. El médico o enfermero también inserta uno o dos lubricados, dedos enguantados de una mano en la vagina y coloca la otra mano sobre la parte inferior del abdomen to feel the size, shape, and position of the uterus and ovaries. The doctor or nurse also inserts a lubricated, gloved finger into the rectum to feel for lumps or anómalas zonas.
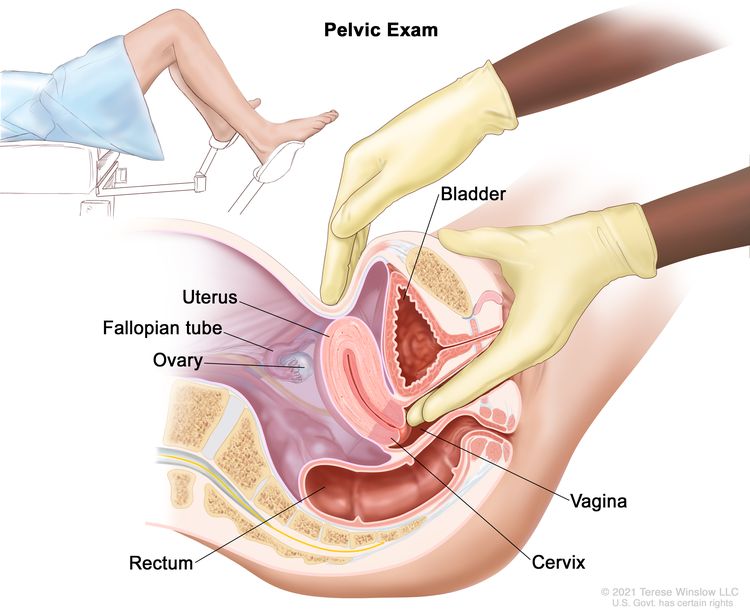
Examen pélvico. Un médico o enfermero introduce uno o dos dedos de una mano, con guantes y lubricados, en la vagina, mientras presiona la parte inferior del abdomen con la otra mano. Esto se hace para palpar el tamaño, la forma y la posición del útero y los ovarios. También se examinan la vagina, el cuello uterino, las trompas de Falopio y el recto.
- Radiografía del tórax: radiografía de los órganos y huesos del interior del tórax. Los rayos X son un tipo de haz de energía que puede atravesar el cuerpo, plasmarse en una película y generar una imagen de áreas del interior del cuerpo.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- Resonancia magnética (RM): se utilizan un imán, ondas de radio y una computadora para generar imágenes detalladas de las estructuras internas del cuerpo. Este procedimiento también se denomina resonancia magnética nuclear (RMN).
- PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
- Lymph node dissection: A surgical procedure in which the lymph nodes are removed from the pelvic area and a sample of tissue is checked under a microscope for signs of cancer. This procedure is also called lymphadenectomy.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
El cáncer puede extenderse desde donde comenzó a otras partes del cuerpo.
Cuando el cáncer se extiende a otra parte del cuerpo se denomina metástasis. Las células cancerosas se desprenden de donde comenzaron (tumor primario) y viajan a través del sistema linfático o la sangre.
- Sistema linfático: el cáncer entra en el sistema linfático, viaja a través de los vasos linfáticos y forma un tumor (tumor metastásico) en otra parte del cuerpo.
- Sangre: el cáncer llega a la sangre, viaja a través de los vasos sanguíneos y forma un tumor (tumor metastásico) en otra parte del cuerpo.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if endometrial cancer spreads to the lung, the cancer cells in the lung are actually endometrial cancer cells. The disease is metastatic endometrial cancer, not lung cancer.
The following stages are used for endometrial cancer:
Estadio I

Stage IA and stage IB endometrial cancer. In stage IA, cancer is in the endometrium only or less than halfway through the myometrium (the muscle layer of the uterus). In stage IB, cancer has spread halfway or more into the myometrium.
In stage I, cancer is found in the uterus only. Stage I is divided into stages IA and IB, based on how far the cancer has spread.
- Stage IA: Cancer is in the endometrium only or less than halfway through the myometrium (muscle layer of the uterus).
- Stage IB: Cancer has spread halfway or more into the myometrium.
Estadio II
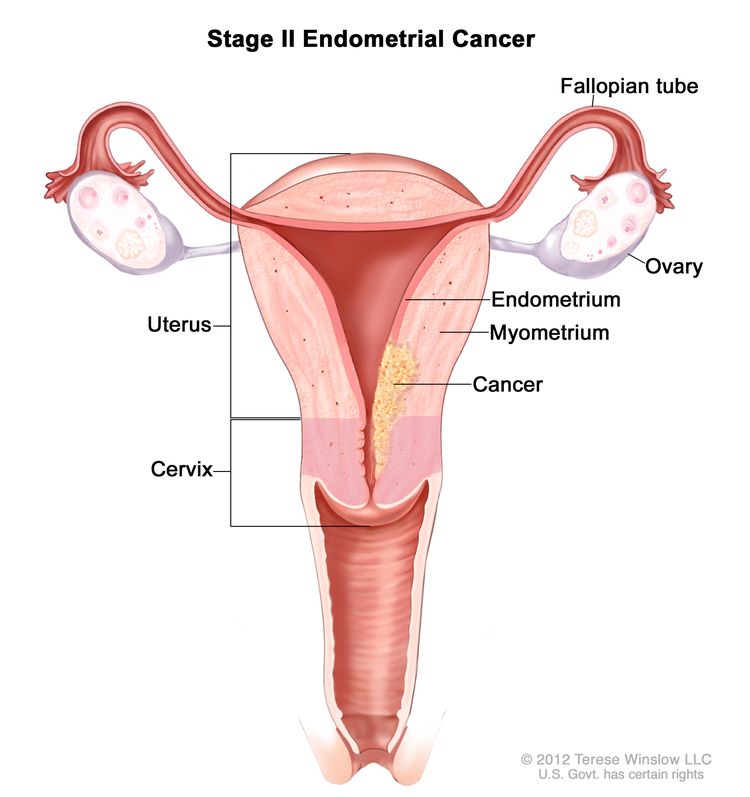
Stage II endometrial cancer. Cancer has spread into connective tissue of the cervix, but has not spread outside the uterus.
In stage II, cancer has spread into connective tissue of the cervix, but has not spread outside the uterus.
Estadio III
In stage III, cancer has spread beyond the uterus and cervix, but has not spread beyond the pelvis. Stage III is divided into stages IIIA, IIIB, and IIIC, based on how far the cancer has spread within the pelvis.
- Stage IIIA: Cáncer has spread to the outer layer of the útero and/or to the trompas de Falopio, ovarios, and ligaments of the uterus.
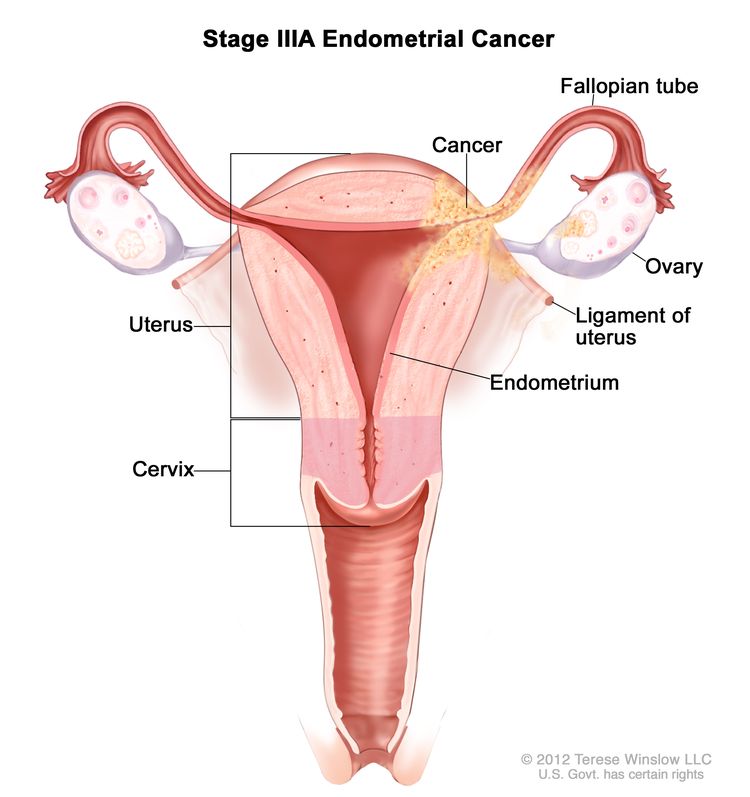
Stage IIIA endometrial cancer. Cancer has spread to the outer layer of the uterus and/or to the fallopian tubes, ovaries, or ligaments of the uterus.
- Estadio IIIB: Cáncer se ha extendido a la vagina and/or to the parametrium (tejido conjuntivo and fat around the útero).
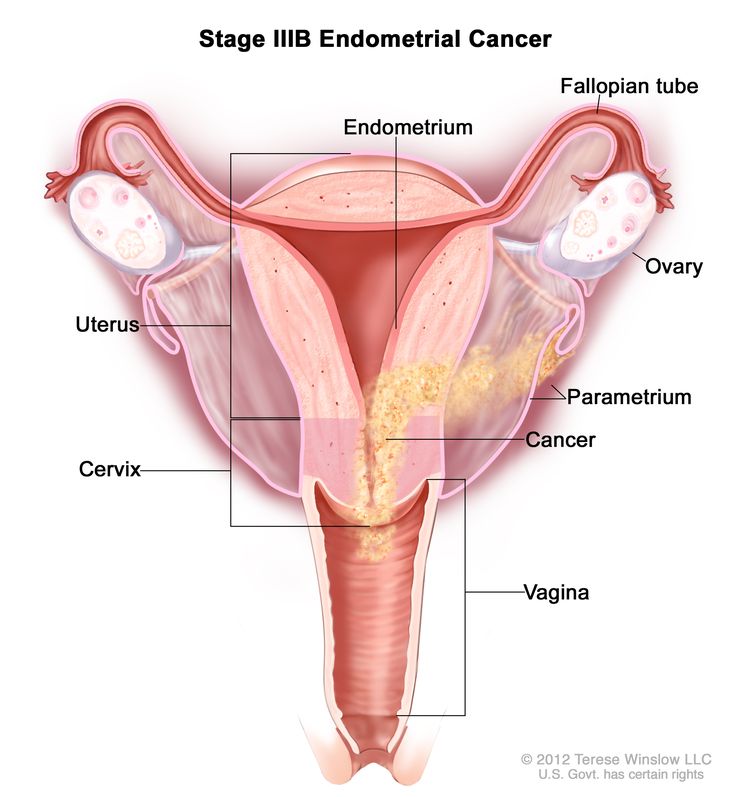
Stage IIIB endometrial cancer. Cancer has spread to the vagina and/or to the parametrium (connective tissue and fat around the uterus and cervix).
- Stage IIIC: Cáncer se ha extendido a los ganglios linfáticos en la pelvis and/or around the aorta (largest artería in the body, which carries sangre away from the heart).
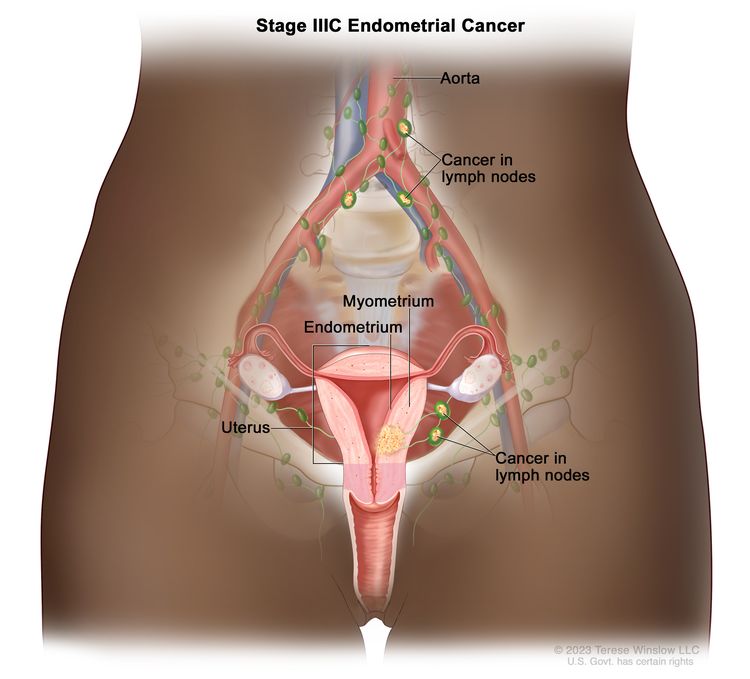
Stage IIIC endometrial cancer. Cancer has spread to lymph nodes in the pelvis and/or around the aorta (the largest artery in the body that carries blood away from the heart).
Estadio IV
In stage IV, cancer has spread beyond the pelvis. Stage IV is divided into stages IVA and IVB, based on how far the cancer has spread.
- Estadio IVA: Cáncer se ha extendido a la bladder and/or intestino wall.
- Estadio IVB: Cáncer has spread to other parts of the body beyond the pelvis, incluido el abdomen and/or ganglios linfáticos en la groin.
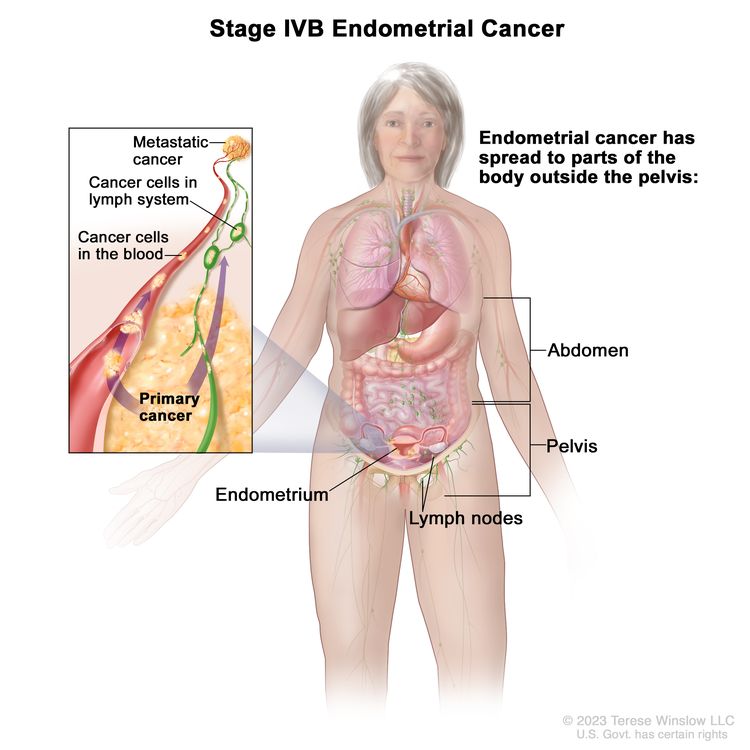
Stage IVB endometrial cancer. The cancer has spread to parts of the body outside the pelvis, including the abdomen and/or lymph nodes in the groin.

Endometrial cancer may be grouped for treatment as follows:
Low-risk endometrial cancer
Grades 1 and 2 tumors are usually considered low-risk. They usually do not spread to other parts of the body.
High-risk endometrial cancer
Grade 3 tumors are considered high-risk. They often spread to other parts of the body. Uterine papillary serous, clear cell, and carcinosarcoma are three subtypes of endometrial cancer that are considered grade 3.
Endometrial cancer can recur (come back) after it has been treated.
The cancer may come back in the uterus, the pelvis, in lymph nodes in the abdomen, or in other parts of the body.
Treatment Option Overview
Puntos clave
- There are different types of treatment for patients with endometrial cancer.
- Five types of standard treatment are used:
- Cirugía
- Radioterapia
- Quimioterapia
- Terapia hormonal
- Terapia dirigida
- New types of treatment are being tested in clinical trials.
- Treatment for endometrial cancer may cause side effects.
- Patients may want to think about taking part in a clinical trial.
- Patients can enter clinical trials before, during, or after starting their cancer treatment.
- Pueden ser necesarias pruebas de seguimiento.
There are different types of treatment for patients with endometrial cancer.
Different types of treatment are available for patients with endometrial cancer. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Five types of standard treatment are used:
Cirugía
Surgery (removing the cancer in an operation) is the most common treatment for endometrial cancer. The following surgical procedures may be used:
- Histerectomía total: Surgery to remove the útero, incluido el cuello uterino. If the uterus and cervix are taken out through the vagina, the operation is called a vaginal hysterectomy. If the uterus and cervix are taken out through a large incisión (corte) en el abdomen, the operation is called a total abdominal hysterectomy. If the uterus and cervix are taken out through a small incision (cut) in the abdomen using a laparoscopio, la operación se llama histerectomía laparoscópica total.
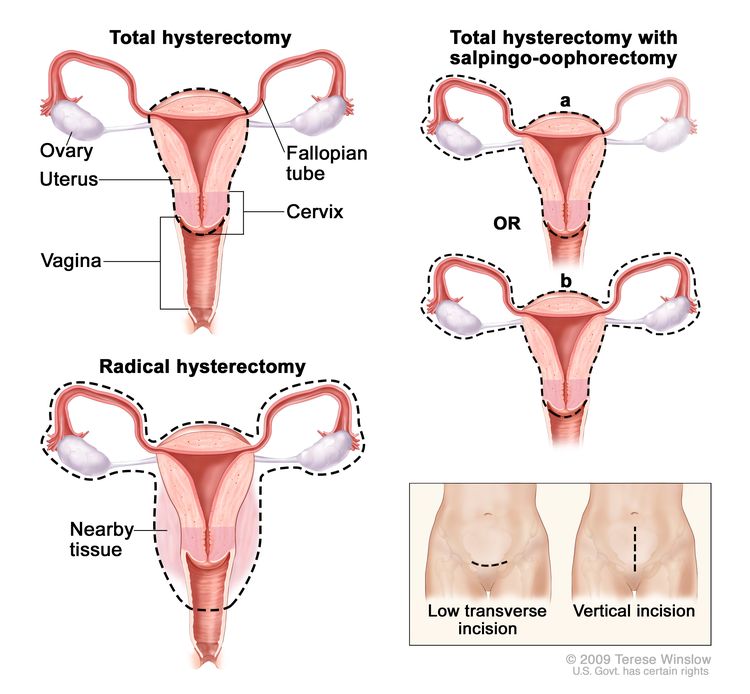
Histerectomía. El útero se extirpa quirúrgicamente con o sin otros órganos o tejidos. En una histerectomía total, se extirpan el útero y el cuello uterino. En una histerectomía total con salpingooforectomía, (a) se extirpan el útero, un ovario y una trompa de Falopio (unilaterales) o (b) se extirpan el útero, ambos ovarios y trompas de Falopio (bilaterales). En una histerectomía radical, se extirpan el útero, el cuello uterino, ambos ovarios, ambas trompas de Falopio y el tejido circundante. Estos procedimientos se realizan mediante una incisión transversal baja o una incisión vertical.
- Bilateral salpingo-oophorectomy: Surgery to remove both ovaries and both fallopian tubes.
- Radical hysterectomy: Surgery to remove the uterus, cervix, and part of the vagina. The ovaries, fallopian tubes, or nearby lymph nodes may also be removed.
- Lymph node dissection: A surgical procedure in which the lymph nodes are removed from the pelvic area and a sample of tissue is checked under a microscope for signs of cancer. This procedure is also called lymphadenectomy.
After the doctor removes all the cancer that can be seen at the time of the surgery, some patients may be given radiation therapy or hormone treatment after surgery to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
Radioterapia
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
- La radioterapia externa utiliza una máquina que envía radiación desde el exterior del cuerpo hacia la zona donde se encuentra el cáncer.
- La radioterapia interna utiliza una sustancia radiactiva sellada en agujas, semillas, cables o catéteres que se colocan directamente en el cáncer o cerca de él.
The way the radiation therapy is given depends on the type and stage of the cancer being treated. External and internal radiation therapy are used to treat endometrial cancer, and may also be used as palliative therapy to relieve symptoms and improve quality of life.
Quimioterapia
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping the cells from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid, an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas (regional chemotherapy).
The way the chemotherapy is given depends on the type and stage of the cancer being treated.
Terapia hormonal
Hormone therapy is a cancer treatment that removes hormones or blocks their action and stops cancer cells from growing. Hormones are substances made by glands in the body and circulated in the bloodstream. Some hormones can cause certain cancers to grow. If tests show that the cancer cells have places where hormones can attach (receptors), drugs, surgery, or radiation therapy is used to reduce the production of hormones or block them from working.
Terapia dirigida
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells. Targeted therapies usually cause less harm to normal cells than chemotherapy or radiation therapy do. Monoclonal antibodies, mTOR inhibitors, and signal transduction inhibitors are three types of targeted therapy used to treat endometrial cancer.
- Terapia con anticuerpos monoclonales: Monoclonal anticuerpos are sistema inmunitario proteínas made in the laboratory to treat many diseases, including cancer. As a cancer treatment, these antibodies can attach to a specific target on cancer cells or other cells that may help cancer cells grow. The antibodies are able to then kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusión. Pueden utilizarse solos o para transportar medicamentos, toxinas, o material radiactivo directamente a las células cancerosas. Bevacizumab is used to treat estadio III, estadio IV, and recurrente endometrial cancer.
- mTOR inhibitor therapy: mTOR inhibitors block a protein called mTOR, which helps control cell division. mTOR inhibitors may keep cancer cells from growing and prevent the growth of new blood vessels that tumors need to grow. Everolimus and ridaforolimus are used to treat stage III, stage IV, and recurrent endometrial cancer.
- Signal transduction inhibitor therapy: Signal transduction inhibitors block signals that are passed from one molecule to another inside a cell. Blocking these signals may kill cancer cells. Metformin is being studied to treat stage III, stage IV, and recurrent endometrial cancer.
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the NCI website.
Treatment for endometrial cancer may cause side effects.
Para obtener información sobre los efectos secundarios causados por el tratamiento para el cáncer, visite la página de efectos secundarios.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Pueden ser necesarias pruebas de seguimiento.
A medida que avanza el tratamiento, se le realizarán pruebas o controles de seguimiento. Es posible que se repitan algunas pruebas para diagnosticar o estadificar el cáncer con el fin de evaluar cómo está funcionando el tratamiento. Las decisiones sobre si continuar, modificar o suspender el tratamiento pueden basarse en los resultados de estas pruebas.
Algunas pruebas seguirán realizándose de manera periódica después de terminar el tratamiento. Los resultados pueden indicar si su afección ha cambiado o si el cáncer ha redicivado (regresado).
Treatment of Stage I and Stage II Endometrial Cancer
For information about the treatments listed below, see the Treatment Option Overview section.
Low-risk endometrial cancer (grade 1 or grade 2)
Treatment of low-risk stage I endometrial cancer and stage II endometrial cancer may include the following:
- Surgery (total hysterectomy and bilateral salpingo-oophorectomy). Lymph nodes in the pelvis and abdomen may also be removed and viewed under a microscope to check for cancer cells.
- Surgery (total hysterectomy and bilateral salpingo-oophorectomy, with or without removal of lymph nodes in the pelvis and abdomen) followed by internal radiation therapy. In certain cases, external radiation therapy to the pelvis may be used in place of internal radiation therapy.
- Radiation therapy alone for patients who cannot have surgery.
- A clinical trial of a new chemotherapy regimen.
If cancer has spread to the cervix, a radical hysterectomy with bilateral salpingo-oophorectomy may be done.
High-risk endometrial cancer (grade 3)
Treatment of high-risk stage I endometrial cancer and stage II endometrial cancer may include the following:
- Surgery (radical hysterectomy and bilateral salpingo-oophorectomy). Lymph nodes in the pelvis and abdomen may also be removed and viewed under a microscope to check for cancer cells.
- Surgery (radical hysterectomy and bilateral salpingo-oophorectomy) followed by chemotherapy and sometimes radiation therapy.
- A clinical trial of a new chemotherapy regimen.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Treatment of Stage III, Stage IV, and Recurrent Endometrial Cancer
For information about the treatments listed below, see the Treatment Option Overview section.
Treatment of stage III endometrial cancer, stage IV endometrial cancer, and recurrent endometrial cancer may include the following:
- Surgery (radical hysterectomy and removal of lymph nodes in the pelvis so they can be viewed under a microscope to check for cancer cells) followed by adjuvant chemotherapy and/or radiation therapy.
- Chemotherapy and internal and external radiation therapy for patients who cannot have surgery.
- Hormone therapy for patients who cannot have surgery or radiation therapy.
- Targeted therapy with mTOR inhibitors (everolimus or ridaforolimus) or a monoclonal antibody (bevacizumab).
- A clinical trial of a new treatment regimen that may include combination chemotherapy, targeted therapy, such as an mTOR inhibitor (everolimus) or signal transduction inhibitor (metformin), and/or hormone therapy, for patients with advanced or recurrent endometrial cancer.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
To Learn More About Endometrial Cancer
For more information from the National Cancer Institute about endometrial cancer, see the following:
- Uterine Cancer Home Page
- Prevención del cáncer de endometrio
- Detección del cáncer de endometrio
- Terapia hormonal para el cáncer de mama
For general cancer information and other resources from the National Cancer Institute, visit:
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
This PDQ cancer information summary has current information about the treatment of endometrial cancer. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
PDQ® Adult Treatment Editorial Board. PDQ Endometrial Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/uterine/patient/endometrial-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389334]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Updated:
Source URL: https://www.cancer.gov/node/4306/syndication
Agencia de origen: National Cancer Institute (NCI)
Captured Date: 2013-09-14 09:02:08.0