








Tratamiento del carcinoma de origen primario desconocido
Acceda a una atención excepcional para todo tipo de cáncer, incluidos los cánceres de origen primario desconocido (también conocidos como carcinomas de origen primario desconocido) en Montefiore Einstein Comprehensive Cancer Center. Somos uno de los primeros centros de cáncer designados por el NCI, desde hace más de 50 años, y como tales, hemos liderado la investigación, diagnóstico y tratamiento de más de 200 tipos de cáncer.
Si le diagnostican cáncer y no está claro dónde se originó la enfermedad en su cuerpo, necesita atención especializada de expertos para lograr el mejor resultado posible. Elija un centro del cáncer reconocido por desarrollar pruebas diagnósticas y tratamientos innovadores mediante investigación de vanguardia. Nuestro Cancer Center Integral está clasificado entre el 1 % de los mejores hospitales del país en atención médica del cáncer según U.S. News & World Report y es reconocido como uno de los mejores del país en atención médica del cáncer. Encuentre respuestas y un plan de tratamiento personalizado a sus necesidades con un equipo multidisciplinario y compasivo en el Montefiore Einstein Comprehensive Cancer Center.
Si necesita atención médica, confíe en nuestros profesionales, que se dedican con pasión a acabar con el cáncer y a atender todas sus necesidades de salud.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Tratamiento del carcinoma de origen primario desconocido (PDQ)–Versión para pacientes
Información general sobre el carcinoma de origen primario desconocido
Puntos clave
- El carcinoma de origen primario desconocido (CUP) es una enfermedad poco común en la que se encuentran células malignas (cancerosas) en el cuerpo pero no se conoce el lugar donde comenzó el cáncer.
- A veces el cáncer primario nunca se detecta.
- Los signos y síntomas del CUP son diferentes, dependiendo de dónde se haya propagado el cáncer en el cuerpo.
- Debido a que no se conoce el lugar donde comenzó el cáncer, se pueden realizar muchas pruebas y procedimientos para buscar el cáncer primario.
- Si las pruebas muestran que puede haber cáncer, se realiza una biopsia.
- Cuando el tipo de células cancerosas o tejido extirpado es diferente del tipo de células cancerosas que se esperaba encontrar, se puede hacer un diagnóstico de CUP.
- Las pruebas y procedimientos utilizados para encontrar el cáncer primario dependen de dónde se ha propagado el cáncer.
- Hay ciertos factores que afectan al pronóstico (la probabilidad de recuperación).
El carcinoma de origen primario desconocido (CUP) es una enfermedad poco común en la que se encuentran células malignas (cancerosas) en el cuerpo pero no se conoce el lugar donde comenzó el cáncer.
El cáncer puede formarse en cualquier tejido del cuerpo. El cáncer primario (el cáncer que se formó inicialmente) puede propagarse a otras partes del cuerpo. Este proceso se llama metástasis . Las células cancerosas suelen parecerse a las células del tipo de tejido en el que se originó el cáncer. Por ejemplo, las células de cáncer de mama pueden propagarse al pulmón . Dado que el cáncer se originó en la mama, las células cancerosas del pulmón se parecen a las células de cáncer de mama .
A veces, los médicos detectan la propagación del cáncer, pero no pueden determinar en qué parte del cuerpo comenzó a crecer. Este tipo de cáncer se denomina cáncer de origen primario desconocido (CUP) o tumor primario oculto .
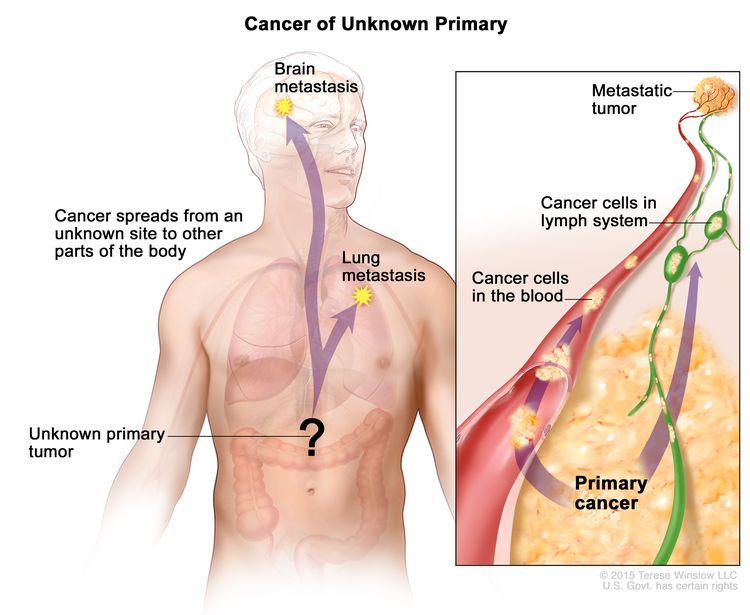
En el cáncer de origen primario desconocido, las células cancerosas se han diseminado en el cuerpo, pero no se conoce el lugar donde comenzó el cáncer primario.
Se realizan pruebas para determinar dónde se originó el cáncer primario y obtener información sobre su propagación. Cuando las pruebas detectan el cáncer primario, este deja de ser un CUP y el tratamiento se basa en el tipo de cáncer primario.
A veces el cáncer primario nunca se detecta.
Es posible que no se detecte el cáncer primario (el cáncer que se formó primero) por una de las siguientes razones:
- El cáncer primario es muy pequeño y crece lentamente.
- El sistema inmunitario del cuerpo mató el cáncer primario.
- El cáncer primario se extirpó durante una cirugía por otra afección y los médicos desconocían la formación del cáncer. Por ejemplo, un útero con cáncer puede extirparse durante una histerectomía para tratar una infección grave.
Los signos y síntomas del CUP son diferentes, dependiendo de dónde se haya propagado el cáncer en el cuerpo.
A veces, el CUP no causa signos ni síntomas . Estos signos y síntomas pueden deberse al CUP o a otras afecciones. Consulte con su doctor si presenta alguno de los siguientes síntomas:
- Bulto o engrosamiento en cualquier parte del cuerpo.
- Dolor que está en una parte del cuerpo y no desaparece.
- Tos que no desaparece o ronquera en la voz.
- Cambio en los hábitos intestinales o de vejiga, como constipación, diarrea o micción frecuente.
- Sangrado o alta médica inusual.
- Fiebre sin causa conocida que no desaparece.
- Sudores nocturnos profusos.
- Pérdida de peso sin razón conocida o pérdida de apetito .
Debido a que no se conoce el lugar donde comenzó el cáncer, se pueden realizar muchas pruebas y procedimientos para buscar el cáncer primario.
Se pueden utilizar las siguientes pruebas y procedimientos:
- Reconocimiento físico e historial de salud: un examen del cuerpo para evaluar el estado general de salud, incluida la detección de signos de enfermedad, como bultos o cualquier otra anomalía. También se toma nota de los hábitos de salud del paciente y de sus enfermedades y tratamientos previos.
- Análisis de orina: una prueba para comprobar el color de la orina y su contenido, como azúcar, proteínas, sangre y bacterias .
- Estudios de química sanguínea: pruebas por las que se examina una muestra de sangre para medir las cantidades de ciertas sustancias liberadas a la sangre por los órganos y tejidos del cuerpo. Una cantidad inusual (mayor o menor de lo normal) de una sustancia puede ser un signo de enfermedad.
- Hemograma completo: procedimiento en el que se extrae una muestra de sangre y se examina:
- La cantidad de glóbulos rojos, glóbulos blancos y plaquetas
- La cantidad de hemoglobina (la proteína que transporta el oxígeno) en los glóbulos rojos
- La parte de la muestra que está formada por glóbulos rojos.
- análisis de sangre oculta en heces: Prueba para detectar sangre en las heces (residuos sólidos) que solo se puede ver con un microscopio . Se colocan pequeñas muestras de heces en tarjetas especiales y se envían al doctor o al laboratorio para su análisis. Dado que algunos cánceres sangran, la presencia de sangre en las heces puede ser un signo de cáncer de colon o recto .
Si las pruebas muestran que puede haber cáncer, se realiza una biopsia.
Una biopsia es la extracción de células o tejidos para que un patólogo los observe al microscopio. El patólogo examina el tejido al microscopio para detectar células cancerosas y determinar el tipo de cáncer. El tipo de biopsia que se realiza depende de la parte del cuerpo que se esté examinando. Se puede utilizar uno de los siguientes tipos de biopsia:
- Biopsia escisional: extirpación de un bulto completo de tejido
- Biopsia incisional: extracción de parte de un bulto o de una muestra de tejido
- Biopsia central: extracción de tejido mediante una aguja ancha
- Biopsia por aspiración con aguja fina (AAF): extracción de tejido o líquido mediante una aguja fina.
Si se detecta cáncer, se pueden utilizar una o más de las siguientes pruebas de laboratorio para estudiar las muestras de tejido y determinar el tipo de cáncer:
- Análisis genético: Prueba de laboratorio en la que se estudia el ADN de una muestra de células o tejido canceroso para verificar si hay mutaciones (cambios) que puedan ayudar a predecir el mejor tratamiento para el carcinoma de origen primario desconocido.
- Estudio histológico: Prueba de laboratorio en la que se añaden tinciones a una muestra de células o tejido canceroso y se observan al microscopio para detectar ciertos cambios en las células. Ciertos cambios en las células se relacionan con ciertos tipos de cáncer.
- Inmunohistoquímica: Prueba de laboratorio que utiliza anticuerpos para detectar ciertos antígenos ( marcadores ) en una muestra de tejido de un paciente. Los anticuerpos suelen estar unidos a una enzima o un colorante fluorescente. Tras unirse a un antígeno específico en la muestra de tejido, la enzima o el colorante se activan y el antígeno puede observarse al microscopio. Este tipo de prueba se utiliza para diagnosticar el cáncer y distinguirlo de otros.
- Prueba de reacción en cadena de la polimerasa con transcriptasa inversa (RT-PCR): Una prueba de laboratorio en la que se mide la cantidad de una sustancia genética llamada ARNm producida por un gen específico. Una enzima llamada transcriptasa inversa se utiliza para convertir un fragmento específico de ARN en un fragmento coincidente de ADN, que puede ser amplificado (producido en grandes cantidades) por otra enzima llamada ADN polimerasa. Las copias de ADN amplificadas ayudan a determinar si un ARNm específico está siendo producido por un gen. La RT-PCR se puede utilizar para verificar la activación de ciertos genes que pueden indicar la presencia de células cancerosas. Esta prueba puede usarse para buscar ciertos cambios en un gen o cromosoma, lo que puede ayudar a diagnosticar el cáncer.
- Análisis citogenético: Prueba de laboratorio en la que se cuentan los cromosomas de las células de una muestra de tejido tumoral y se analizan para detectar cualquier cambio, como cromosomas rotos, faltantes, reorganizados o adicionales. Los cambios en ciertos cromosomas pueden ser un signo de cáncer. El análisis citogenético se utiliza para diagnosticar el cáncer, planificar el tratamiento o determinar su eficacia. Los cambios en ciertos cromosomas están relacionados con ciertos tipos de cáncer.
- Microscopía óptica y electrónica: prueba de laboratorio en la que se observan las células de una muestra de tejido bajo microscopios regulares y de alta potencia para buscar ciertos cambios en las células.
Cuando el tipo de células cancerosas o tejido extirpado es diferente del tipo de células cancerosas que se esperaba encontrar, se puede hacer un diagnóstico de CUP.
Las células del cuerpo tienen una apariencia específica que depende del tipo de tejido del que provienen. Por ejemplo, se espera que una muestra de tejido canceroso extraída de la mama esté compuesta de células mamarias. Sin embargo, si la muestra de tejido es de un tipo diferente (no está compuesta de células mamarias), es probable que las células se hayan propagado a la mama desde otra parte del cuerpo. Para planificar el tratamiento, los médicos primero intentan encontrar el cáncer primario (el cáncer que se formó inicialmente).
Las pruebas y procedimientos utilizados para encontrar el cáncer primario dependen de dónde se ha propagado el cáncer.
En algunos casos, la parte del cuerpo donde se encuentran primero las células cancerosas ayuda al doctor a decidir qué pruebas de diagnóstico serán más útiles.
- Cuando el cáncer se encuentra por encima del diafragma (el músculo delgado debajo de los pulmones que ayuda con la respiración), es probable que el sitio primario del cáncer esté en la parte superior del cuerpo, como en el pulmón o la mama.
- Cuando el cáncer se encuentra debajo del diafragma, es probable que el sitio primario del cáncer esté en la parte inferior del cuerpo, como el páncreas, el hígado u otro órgano del abdomen .
- Algunos cánceres se propagan comúnmente a ciertas zonas del cuerpo. En el caso del cáncer localizado en los ganglios linfáticos del cuello, es probable que el foco primario del cáncer sea la cabeza o el cuello, ya que estos cánceres suelen propagarse a los ganglios linfáticos del cuello.
Se pueden realizar las siguientes pruebas y procedimientos para encontrar dónde comenzó el cáncer por primera vez:
- tomografía computarizada (TC): Procedimiento que genera una serie de imágenes detalladas de áreas internas del cuerpo, como el tórax o el abdomen, tomadas desde diferentes ángulos. Las imágenes se generan mediante una computadora conectada a un equipo de rayos X. Se puede inyectar un tinte en una vena o ingerirlo para que los órganos o tejidos se visualicen con mayor claridad. Este procedimiento también se denomina tomografía axial computarizada (TAC) o escáner axial computarizado..
- Resonancia magnética (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- PET (tomografía por emisión de positrones): procedimiento para encontrar células tumorales malignas en el cuerpo. Se inyecta una pequeña cantidad de glucosa (azúcar) radiactiva en una vena. El escáner PET gira alrededor del cuerpo y genera una imagen de dónde se utiliza la glucosa en el cuerpo. Las células tumorales malignas aparecen más brillantes en la imagen porque son más activas y absorben más glucosa que las células normales.
- Mamografía: Una radiografía de la mama.
- Endoscopia: Procedimiento para examinar los órganos y tejidos del cuerpo y detectar áreas anormales . Se inserta un endoscopio a través de una incisión (corte) en la piel o una abertura en el cuerpo, como la boca. Un endoscopio es un instrumento delgado, similar a un tubo, con una luz y una lente para observar. También puede tener una herramienta para extraer muestras de tejido o ganglios linfáticos, que se examinan al microscopio para detectar signos de enfermedad. Por ejemplo, se puede realizar una colonoscopia .
- Prueba de marcadores tumorales: Procedimiento en el que se analiza una muestra de sangre, orina o tejido para medir la cantidad de ciertas sustancias producidas por órganos, tejidos o células tumorales del cuerpo. Ciertas sustancias se relacionan con tipos específicos de cáncer cuando se detectan en niveles elevados en el cuerpo. Estas se denominan marcadores tumorales . Se pueden analizar los niveles de sangre de CA-125, CgA, alfa-fetoproteína (AFP), gonadotropina coriónica humana beta (beta-hCG) o antígeno prostático específico (PSA) .
A veces, ninguna prueba puede encontrar la localización primaria del cáncer. En estos casos, el tratamiento puede basarse en el tipo de cáncer que el doctor considere más probable.
Hay ciertos factores que afectan al pronóstico (la probabilidad de recuperación).
El pronóstico depende de los siguientes factores:
- Dónde comenzó el cáncer en el cuerpo y dónde se ha propagado.
- El número de órganos con cáncer en ellos.
- El aspecto que tienen las células tumorales cuando se observan bajo un microscopio.
- Si el paciente es hombre o mujer.
- Si el cáncer acaba de ser diagnosticado o ha recidivado (regresado)
Para la mayoría de los pacientes con CUP, los tratamientos actuales no curan el cáncer. Es posible que los pacientes deseen participar en uno de los numerosos ensayos clínicos que se realizan para mejorar el tratamiento. Se están realizando ensayos clínicos para el CUP en muchas partes del país. Puede encontrar información sobre ensayos clínicos en el sitio web del NCI .
Estadios del carcinoma de origen primario desconocido
Puntos clave
- No existe un sistema de estadificación estándar para el carcinoma de origen primario desconocido (CUP).
- La información que se conoce sobre el cáncer se utiliza para planificar el tratamiento.
No existe un sistema de estadificación estándar para el carcinoma de origen primario desconocido (CUP).
La extensión o propagación del cáncer suele describirse en estadios . El estadio del cáncer suele utilizarse para planificar el tratamiento. Sin embargo, el carcinoma de origen primario desconocido (CUP) ya se ha propagado a otras partes del cuerpo cuando se detecta. No existe un sistema de estadificación estándar para el CUP.
A veces el CUP reaparece (regresa) después del tratamiento.
La información que se conoce sobre el cáncer se utiliza para planificar el tratamiento.
Los médicos utilizan los siguientes tipos de información para planificar el tratamiento:
- El lugar del cuerpo donde se encuentra el cáncer, como el peritoneo o los ganglios linfáticos cervicales (cuello), axilares (axila) o inguinales ( ingle ).
- El tipo de célula cancerosa, como el melanoma .
- Si la célula cancerosa está poco diferenciada (se ve muy diferente de las células normales cuando se observa bajo un microscopio ).
- Los signos y síntomas causados por el cáncer.
- Los resultados de pruebas y procedimientos.
- Si el cáncer se ha diagnosticado recientemente o ha reaparecido (regresado).
Treatment Option Overview
Puntos clave
- Existen diferentes tipos de tratamiento para los pacientes con carcinoma de primario desconocido (CUP).
- Se utilizan cuatro tipos de tratamiento estándar:
- Cirugía
- Radioterapia
- Quimioterapia
- Terapia hormonal
- New types of treatment are being tested in clinical trials.
- El tratamiento del carcinoma de origen primario desconocido puede provocar efectos secundarios.
- Patients may want to think about taking part in a clinical trial.
- Patients can enter clinical trials before, during, or after starting their cancer treatment.
Existen diferentes tipos de tratamiento para los pacientes con carcinoma de primario desconocido (CUP).
Existen diferentes tipos de tratamiento disponibles para pacientes con CUP . Algunos tratamientos son estándar (el tratamiento que se utiliza actualmente) y otros se están probando en ensayos clínicos . Un ensayo clínico de tratamiento es un estudio de investigación cuyo objetivo es mejorar los tratamientos actuales u obtener información sobre nuevos tratamientos para pacientes con cáncer . Cuando los ensayos clínicos demuestran que un nuevo tratamiento es mejor que el tratamiento estándar, este puede convertirse en el tratamiento estándar. Los pacientes podrían considerar participar en un ensayo clínico. Algunos ensayos clínicos están abiertos solo a pacientes que no han comenzado el tratamiento.
Se utilizan cuatro tipos de tratamiento estándar:
Cirugía
La cirugía es un tratamiento común para el CUP. El doctor puede extirpar el cáncer y parte del tejido sano circundante.
Después de que el doctor extirpe todo el cáncer visible en el momento de la cirugía, algunos pacientes podrían recibir quimioterapia o radioterapia para eliminar cualquier célula cancerosa restante. El tratamiento que se administra después de la cirugía para reducir el riesgo de reaparición del cáncer se denomina terapia adyuvante .
Radioterapia
La radioterapia es un tratamiento contra el cáncer que utiliza rayos X de alta energía u otros tipos de radiación para matar las células cancerosas o evitar que crezcan. Hay dos tipos de radioterapia:
- Radioterapia externa Utiliza una máquina externa al cuerpo para enviar radiación hacia la zona con cáncer. Ciertas formas de administrar radioterapia pueden ayudar a evitar que la radiación dañe el tejido sano cercano. Este tipo de radioterapia puede incluir lo siguiente:
- Radioterapia de intensidad modulada (IMRT): La IMRT es un tipo de radioterapia tridimensional (3D) que utiliza una computadora para generar imágenes del tamaño y la forma del tumor . Se dirigen delgados haces de radiación de diferentes intensidades al tumor desde diversos ángulos. Este tipo de radioterapia externa causa menos daño al tejido sano circundante y es menos probable que cause sequedad bucal, dificultad deglución y daño a la piel.
- La radioterapia interna utiliza una sustancia radiactiva sellada en agujas, semillas, cables o catéteres que se colocan directamente en el cáncer o cerca de él.
La forma de administrar la radioterapia depende del tipo y el estadio del cáncer que se esté tratando. La radioterapia externa e interna se utiliza para tratar el carcinoma de origen primario desconocido.
Quimioterapia
La quimioterapia es un tratamiento contra el cáncer que utiliza medicamentos para detener el crecimiento de las células cancerosas, ya sea destruyéndolas o impidiendo su división. Cuando la quimioterapia se administra por vía oral o se inyecta en una vena o músculo, los medicamentos ingresan al torrente sanguíneo y pueden alcanzar las células cancerosas de todo el cuerpo ( quimioterapia sistémica ). Cuando la quimioterapia se administra directamente en el líquido cefalorraquídeo, un órgano o una cavidad corporal como el abdomen, los medicamentos afectan principalmente a las células cancerosas en esas áreas ( quimioterapia regional ). La quimioterapia combinada es el uso de dos o más medicamentos contra el cáncer.
Terapia hormonal
La terapia hormonal es un tratamiento contra el cáncer que elimina las hormonas o bloquea su acción e impide el crecimiento de las células cancerosas. Las hormonas son sustancias producidas por las glándulas del cuerpo y que circulan por el torrente sanguíneo. Algunas hormonas pueden provocar el crecimiento de ciertos tipos de cáncer. Si las pruebas muestran que las células cancerosas tienen receptores (lugares donde las hormonas pueden adherirse), se utilizan medicamentos, cirugía o radioterapia para reducir la producción de hormonas o impedir su acción.
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the NCI website.
El tratamiento del carcinoma de origen primario desconocido puede provocar efectos secundarios.
For information about side effects caused by treatment for cancer, visit our Side Effects page.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Tratamiento del carcinoma recién diagnosticado de origen primario desconocido
Ganglios linfáticos cervicales (cuello)
For information about the treatments listed below, see the Treatment Option Overview section.
El cáncer detectado en los ganglios linfáticos cervicales (cuello) puede haberse propagado desde un tumor en la cabeza o el cuello. El tratamiento del carcinoma ganglionar cervical de origen primario desconocido (CUP) puede incluir lo siguiente:
- Cirugía para extirpar las amígdalas .
- Radioterapia sola. Se puede utilizar radioterapia de intensidad modulada (IMRT).
- Radioterapia seguida de cirugía para extirpar los ganglios linfáticos.
- Cirugía para extirpar los ganglios linfáticos, con o sin radioterapia.
- Un ensayo clínico de nuevos tipos de tratamiento.
Consulte el resumen del PDQ sobre el cáncer de cuello escamoso metastásico con tratamiento primario oculto para obtener más información.
Carcinomas pobremente diferenciados
For information about the treatments listed below, see the Treatment Option Overview section.
Las células cancerosas poco diferenciadas tienen un aspecto muy diferente al de las células normales. Se desconoce el tipo de célula de la que provienen. El tratamiento del carcinoma poco diferenciado de origen primario desconocido, incluidos los tumores del sistema neuroendocrino (la parte del cerebro que controla las glándulas productoras de hormonas en todo el cuerpo), puede incluir lo siguiente:
- Quimioterapia combinada.
- Un ensayo clínico de nuevos tipos de tratamiento.
Mujeres con cáncer peritoneal
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento para mujeres con carcinoma peritoneal (revestimiento del abdomen ) de origen primario desconocido puede ser el mismo que para el cáncer de ovario . El tratamiento puede incluir lo siguiente:
- Quimioterapia.
- Un ensayo clínico de nuevos tipos de tratamiento.
Consulte el resumen del PDQ sobre el tratamiento del cáncer epitelial de ovario, de las trompas de Falopio y primario de peritoneo para obtener más información.
Metástasis aislada de ganglios linfáticos axilares
For information about the treatments listed below, see the Treatment Option Overview section.
El cáncer que se encuentra únicamente en los ganglios linfáticos axilares puede haberse propagado desde un tumor en la mama .
El tratamiento de la metástasis de los ganglios linfáticos axilares suele ser:
- Cirugía para extirpar los ganglios linfáticos.
El tratamiento también puede incluir uno o más de los siguientes:
- Cirugía para extirpar la mama.
- Radioterapia en la mama.
- Quimioterapia.
- Un ensayo clínico de nuevos tipos de tratamiento.
Metástasis en los ganglios linfáticos inguinales
For information about the treatments listed below, see the Treatment Option Overview section.
El cáncer que se encuentra solo en los ganglios linfáticos inguinales ( ingle ) probablemente se originó en la zona genital, anal o rectal . El tratamiento de la metástasis en los ganglios linfáticos inguinales puede incluir lo siguiente:
- Cirugía para extirpar el cáncer y/o los ganglios linfáticos de la ingle.
- Cirugía para extirpar el cáncer y/o los ganglios linfáticos de la ingle, seguida de radioterapia o quimioterapia .
Melanoma en un solo área de ganglio linfático
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento del melanoma que se encuentra sólo en una zona de ganglio linfático suele ser:
- Cirugía para extirpar los ganglios linfáticos.
Consulte el resumen del PDQ sobre el tratamiento del melanoma para obtener más información.
Participación múltiple
For information about the treatments listed below, see the Treatment Option Overview section.
No existe un tratamiento estándar para el carcinoma de origen primario desconocido que se encuentra en diversas zonas del cuerpo. El tratamiento puede incluir lo siguiente:
- Terapia hormonal.
- Radioterapia interna.
- Quimioterapia con uno o más medicamentos contra el cáncer.
- Un ensayo clínico .
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del carcinoma recurrente de origen primario desconocido
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento del carcinoma recurrente de origen primario desconocido suele realizarse en un ensayo clínico . El tratamiento depende de lo siguiente:
- El tipo de cáncer .
- Cómo se trataba el cáncer antes.
- Dónde ha regresado el cáncer en el cuerpo.
- La condición y los deseos del paciente.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Para Más información sobre el carcinoma de origen primario desconocido
Para obtener más información del National Cancer Institute sobre el carcinoma de origen primario desconocido, consulte lo siguiente:
For general cancer information and other resources from the National Cancer Institute, visit:
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen de información sobre el cáncer del PDQ contiene información actualizada sobre el tratamiento de carcinoma de origen primario desconocido. Su objetivo es informar y ayudar a los pacientes, las familias y los cuidadores. No proporciona directrices ni recomendaciones formales para tomar decisiones sobre la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre el tratamiento para adultos. Tratamiento del carcinoma de origen primario desconocido (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA].
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Actualizado:
URL de origen: https://www.cancer.gov/node/1187/syndication
Agencia de origen: National Cancer Institute (NCI)
Fecha de captura: 14/09/2013 09:00:15.0