Acceda a una atención excepcional para el melanoma en Montefiore Einstein Comprehensive Cancer Center. Como uno de los primeros centros oncológicos del país designados por el Instituto Nacional del Cáncer (NCI), hemos sido líderes en la investigación, el diagnóstico y el tratamiento de más de 200 tipos de cáncer. Somos uno de los pocos centros oncológicos de la región que ofrece interleucina-2 (IL-2) para el tratamiento del melanoma metastásico. También ofrecemos inmunoterapias y terapias dirigidas, incluyendo la terapia de linfocitos infiltrantes de tumores (TIL), recientemente aprobada por la Administración de Alimentos y Medicamentos (FDA). Los pacientes también tienen la oportunidad de participar en ensayos clínicos en etapa temprana donde pueden recibir los tratamientos más recientes mucho antes de que estén disponibles en cualquier otro lugar.
Nuestros especialistas en cáncer e investigadores del cáncer están comprometidos con el descubrimiento de los últimos enfoques de diagnóstico y tratamientos que puedan mejorar los resultados.
Aquí recibirá una atención compasiva y personalizada que cumple con los más altos estándares de calidad y seguridad. El tratamiento del melanoma en Montefiore Einstein Comprehensive Cancer Center es uno de los más completos del país, y estamos comprometidos con la atención integral de la persona en su totalidad. También ofrecemos una amplia variedad de servicios de apoyo, desde orientación nutricional hasta terapias complementarias y alternativas.
Cuando necesite atención para el melanoma, recurra a nuestros proveedores, a quienes les apasiona acabar con el cáncer y abordar todas sus necesidades de salud.
El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Tratamiento del melanoma (PDQ®): versión para pacientes
El melanoma es una enfermedad en la que se forman células malignas (cancerosas) en los melanocitos (células que dan color a la piel).
Hay diferentes tipos de cáncer que comienzan en la piel.
El melanoma puede desarrollarse en cualquier parte de la piel.
Los lunares inusuales, la exposición a la luz solar y el historial de salud pueden afectar el riesgo de desarrollar melanoma.
Algunos de los signos de melanoma son un cambio en la apariencia de un lunar o un área pigmentada.
Para diagnosticar el melanoma se utilizan pruebas que examinan la piel.
Una vez que se ha diagnosticado el melanoma, se pueden realizar pruebas para determinar si las células cancerosas se han diseminado dentro de la piel o a otras partes del cuerpo.
Some people decide to get a second opinion.
Certain factors affect prognosis (chance of recovery) and treatment options.
El melanoma es una enfermedad en la que se forman células malignas (cancerosas) en los melanocitos (células que dan color a la piel).
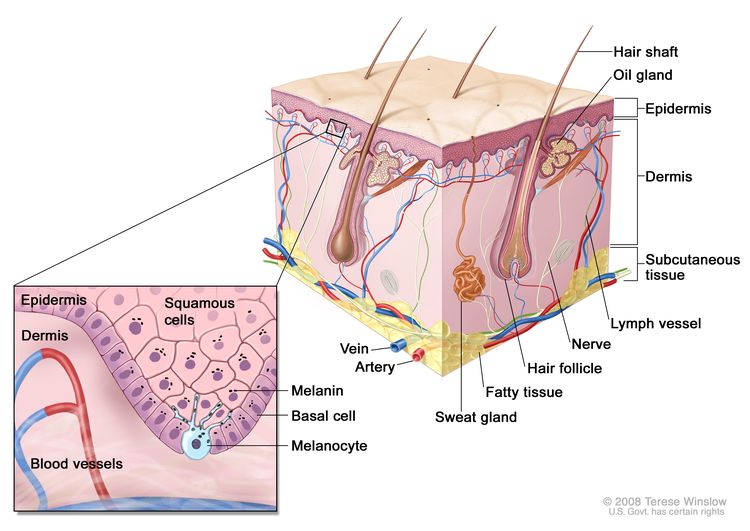
La piel es el órgano más grande del cuerpo. Protege del calor, la luz solar, las lesiones y las infecciones . También ayuda a controlar la temperatura corporal y almacena agua, grasa y vitamina D. La piel tiene varias capas, pero las dos principales son la epidermis (capa superior o externa) y la dermis (capa inferior o interna). El cáncer de piel se origina en la epidermis, que está compuesta por tres tipos de células:
Células escamosas: son células delgadas y planas que forman la capa superior de la epidermis.
Células basales: son células redondas que se encuentran debajo de las células escamosas.
Melanocitos: son células que fabrican melanina y se encuentran en la parte inferior de la epidermis. La melanina es el pigmento que le da a la piel su color natural. Cuando la piel se expone al sol o a la luz artificial, los melanocitos producen más pigmento y hacen que la piel se oscurezca.
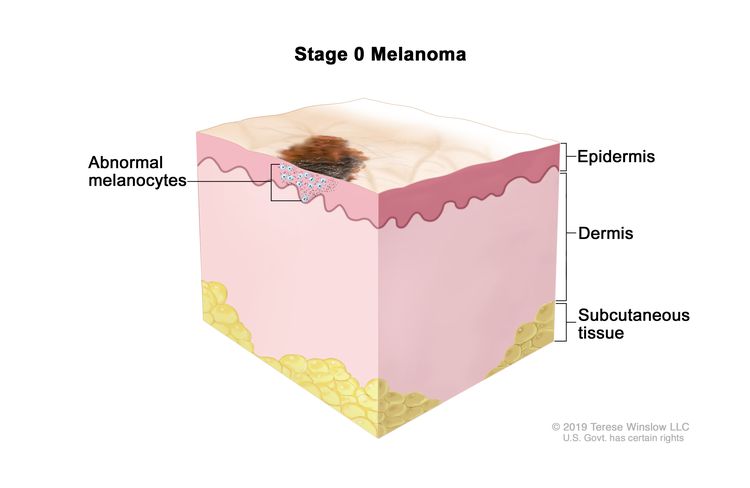
Anatomía de la piel, que muestra la epidermis, la dermis y el tejido subcutáneo. Los melanocitos se encuentran en la capa de células basales, en la parte más profunda de la epidermis.
Hay diferentes tipos de cáncer que comienzan en la piel.
Hay dos formas principales de cáncer de piel: melanoma y no melanoma.
El melanoma es una forma rara de cáncer de piel. Es más probable que invada los tejidos cercanos y se propague a otras partes del cuerpo que otros tipos de este cáncer. Cuando el melanoma comienza en la piel, se denomina melanoma cutáneo. El melanoma también puede aparecer en las membranas mucosas (capas delgadas y húmedas de tejido que cubren superficies como los labios). Este resumen trata sobre el melanoma cutáneo (de la piel) y el que afecta las membranas mucosas.
Las tasas de melanoma en personas menores a 50 años son más altas en mujeres que en hombres. Después de los 50 años, son mucho más altas en hombres. El melanoma es más común en adultos, pero a veces se presenta en niños y adolescentes. Más información sobre el tratamiento del melanoma infantil.
El melanoma puede desarrollarse en cualquier parte de la piel.
En los hombres, el melanoma suele aparecer en el tronco (la zona que abarca desde los hombros hasta la cadera) o en la cabeza y el cuello. En las mujeres, se forma con mayor frecuencia en los brazos y las piernas.
Los lunares inusuales, la exposición a la luz solar y el historial de salud pueden afectar el riesgo de desarrollar melanoma.
Un factor de riesgo es cualquier circunstancia que aumente la probabilidad de contraer una enfermedad. Algunos factores de riesgo del melanoma, como el uso de camas solares, se pueden modificar. Sin embargo, hay otros factores de riesgo que las personas no pueden cambiar, como su genética y el historial de salud de su familia. Aprender sobre los factores de riesgo del melanoma puede ayudarle a implementar cambios que podrían reducir su riesgo de desarrollarlo.
Los factores de riesgo del melanoma son:
Tener una tez clara, lo cual puede ser:
Piel clara que se llena de pecas y se quema fácilmente, no se broncea o se broncea mal.
Ojos azules, verdes o de color claro
Cabello rojo o rubio
Estar expuesto a la luz solar natural o artificial (como la de las camas solares).
Estar expuesto a ciertos factores, como radiación, solventes, cloruro de vinilo y PCB en el medioambiente (en el aire, en su hogar o lugar de trabajo y en sus alimentos o agua)
Tener un historial de muchas quemaduras solares con ampollas, especialmente cuando era niño o adolescente.
Tener varios lunares grandes o muchos lunares pequeños.
Tener ciertos cambios en los genes relacionados con el melanoma.
Si bien ser blanco o tener una tez blanca aumenta el riesgo de desarrollar melanoma, cualquier persona puede tenerlo, incluso si su piel es más oscura.
Algunos de los signos de melanoma son un cambio en la apariencia de un lunar o un área pigmentada.
Estos y otros signos y síntomas pueden ser causados por un melanoma o por otras afecciones. Consulte con su médico si tiene:
Un lunar que:
Presenta cambios de tamaño, forma o color.
Tiene bordes o límites irregulares.
Es de más de un color.
Es asimétrico (si el lunar se divide por la mitad, las dos mitades son diferentes en tamaño o forma).
Le causa comezón.
Supura, sangra o presenta ulceración (se forma un orificio en la piel cuando se rompe la capa superior de células y el tejido de abajo puede verse a través de ella).
Un cambio en la piel pigmentada (coloreada).
Lunares satélites (lunares nuevos que crecen cerca de uno existente).
El acrónimo ABCDE puede ayudarle a recordar los signos del melanoma:
Asimétrico
Borde
Color
Diámetro (el melanoma suele medir más de 6 milímetros)
Evolución (el lunar cambia de tamaño, forma o color con el tiempo)
Para diagnosticar el melanoma se utilizan pruebas que examinan la piel.
El melanoma suele diagnosticarse con pruebas que examinan la piel. El proceso que se utiliza para determinar si las células cancerosas se han propagado a otros lugares se denomina estadificación. Para planificar el tratamiento, es importante conocer el estadio de la enfermedad.
Además de preguntarle sobre su historial de saludpersonal y de su familia y realizarle un reconocimiento físico, su médico puede realizar las siguientes pruebas y procedimientos para encontrar y diagnosticar el melanoma:
Un examen de la piel es una evaluación en la que un médico o enfermero revisa la piel para detectar lunares, marcas de nacimiento u otras áreas pigmentadas que parecen anómalas en cuanto al color, tamaño, forma o textura.
Biopsy es la extracción de células o tejidos para poder observarlos con un microscopio y comprobar si hay signos de cáncer. Puede resultar difícil diferenciar un lunar de color de un melanoma en etapa temprana. lesiónLos pacientes podrían querer que un segundo patólogo analizase la muestra de tejido. Si el lunar o lesión anómala es canceroso, también se podría analizar la muestra para detectar ciertos cambios genéticos. Esto puede ayudar a planificar el tratamiento. Obtenga más información sobre lo que encontrará en el informe de un patólogo sobre las células o el tejido extraído durante una biopsia en Informes de patología.
Hay cuatro tipos principales de biopsias de piel. El tipo de biopsia que se realiza depende de dónde se formó la zona anómala y del tamaño de la misma.
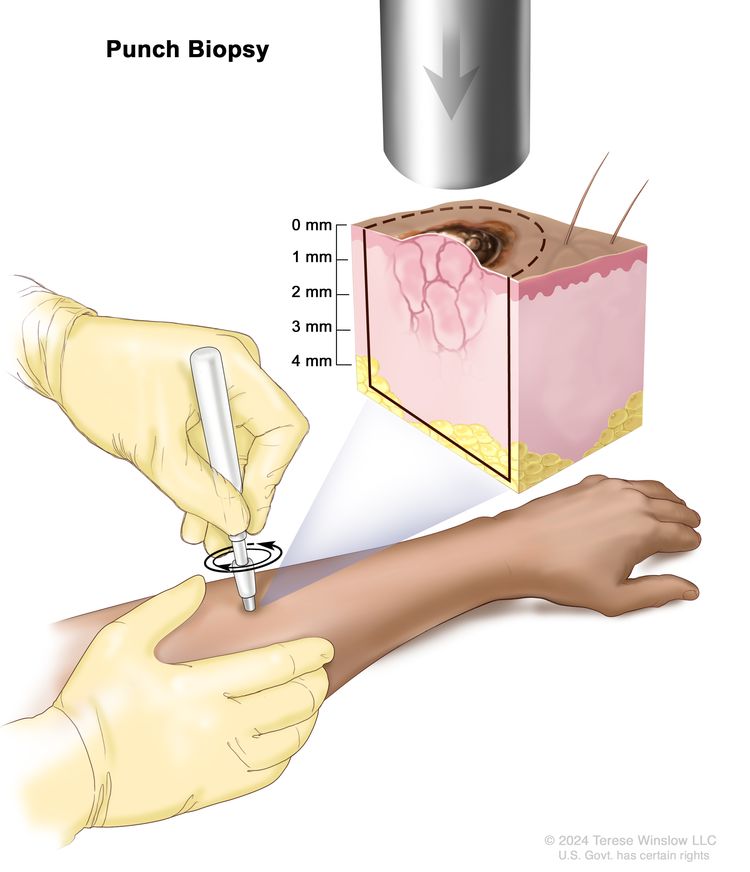
Biopsia por punción: se utiliza un instrumento circular, hueco y afilado para extraer un pequeño trozo redondo de tejido de una lesión en la piel. El instrumento se gira en el sentido de las agujas del reloj y luego en el sentido contrario para cortar unos 4 milímetros (mm) hasta la capa de tejido graso que se encuentra debajo de la piel y extraer la muestra de tejido. El grosor de la piel es diferente según la parte del cuerpo.
La escisional utiliza un bisturí para remover el crecimiento entero.
Una vez que se ha diagnosticado el melanoma, se pueden realizar pruebas para determinar si las células cancerosas se han diseminado dentro de la piel o a otras partes del cuerpo.
El proceso que se utiliza para determinar si el cáncer se ha propagado dentro de la piel o a otras partes del cuerpo se denomina estadificación. La información obtenida del proceso de estadificación determina el estadio de la enfermedad. Es importante conocer el estadio para planificar el tratamiento.
En el caso de un melanoma con un bajo riesgo de propagación a otras partes del cuerpo y de recidiva, es posible que no se necesiten más pruebas. En cambio, en el caso de un melanoma que es probable que se propague a otras partes del cuerpo o que recidive, se pueden realizar las siguientes pruebas y procedimientos después de la cirugía para extirpar el melanoma:
El mapeo de ganglios linfáticos y la biopsia del ganglio centinela incluyen la extirpación del ganglio centinela durante la cirugía. El ganglio centinela es el primer ganglio linfático de un grupo que recibe el drenaje linfático del tumor primario . Es el primer ganglio linfático al que es probable que se disemine el cáncer desde el tumor primario. Se inyecta una sustancia radiactiva o un tinte azul cerca del tumor. La sustancia o el tinte fluye a través de los conductoslinfáticos hacia los ganglios linfáticos. Se extirpa el primer ganglio linfático que recibe la sustancia o el tinte. Un patólogo examina el tejido al microscopio para buscar células cancerosas. Si no se encuentran células cancerosas, puede que no sea necesario extirpar más ganglios linfáticos. A veces, se encuentra un ganglio centinela en más de un grupo de ganglios.
La tomografía computarizada (TC) es un procedimiento que toma una serie de imágenes detalladas de áreas internas del cuerpo desde diferentes ángulos. Las imágenes se crean mediante una computadora conectada a una máquina de rayos X. Se puede inyectar un tinte en una vena o ingerirlo para permitir que los órganos o tejidos se visualicen con mayor claridad. Este procedimiento también se denomina tomografía axial computarizada. En el caso del melanoma, se pueden tomar imágenes del cuello, el tórax, el abdomen y la pelvis.
La tomografía por emisión de positrones (PET) es un procedimiento para detectar células tumorales malignas en el cuerpo. Se inyecta una pequeña cantidad de glucosa (azúcar) radiactiva en una vena. El escáner PET gira alrededor del cuerpo y toma una imagen de las zonas en las que se utiliza la glucosa. Las células tumorales malignas se ven más brillantes en la imagen porque tienen más actividad y absorben más glucosa que las células normales.
La resonancia magnética (RM) con gadolinio es un procedimiento que utiliza un imán, ondas de radio y una computadora para crear una serie de imágenes detalladas de áreas internas del cuerpo, como el cerebro. Se inyecta una sustancia llamada gadolinio en una vena, el cual se acumula alrededor de las células cancerosas para que aparezcan más brillantes en la imagen. Este procedimiento también se llama resonancia magnética nuclear (RMN).
La ecografía es un procedimiento en el que se hacen rebotar ondas sonoras de alta energía (ultrasonido) en los tejidos internos, como los ganglios linfáticos o los órganos, y se generan ecos. Estos ecos forman una imagen de los tejidos corporales que recibe el nombre de ecograma. La imagen se puede imprimir para su analisis posterior.
Los estudios de química sanguínea son un procedimiento en el que se analiza una muestra de sangre para medir las cantidades de ciertas sustancias que liberan los órganos y los tejidos del cuerpo. En el caso del melanoma, se analiza la sangre para detectar una enzima llamada lactato deshidrogenasa (LDH). Los niveles altos de esta enzima pueden predecir una respuesta deficiente al tratamiento en personas con enfermedad metastásica.
Los resultados de estas pruebas se ven junto con los de la biopsia del tumor para conocer el estadio del melanoma.
Some people decide to get a second opinion.
Es posible que desee obtener una segunda opinión para confirmar su diagnóstico de melanoma y su plan de tratamiento. Si busca una segunda opinión, deberá obtener los resultados de las pruebas médicas y los informes del primer médico para compartirlos con el segundo, quien revisará el informe patológico, las laminas histológicas y las exploraciones. Es posible que esté de acuerdo con el primer médico, sugiera cambios u otro enfoque de tratamiento o le ofrezca más información sobre su cáncer.
Si el cáncer tiene ciertas mutaciones (cambios) en un gen llamado BRAF.
La edad y salud general del paciente
Estadios del melanoma
Puntos clave
El estadio del melanoma depende del espesor del tumor, de si el cáncer se ha diseminado a los ganglios linfáticos o a otras partes del cuerpo y de otros factores.
El melanoma se puede estadificar de la siguiente manera:
Estadio 0 (melanoma in situ)
Melanoma en estadio I (también llamado estadio 1)
Melanoma en estadio II (también llamado estadio 2)
Melanoma en estadio III (también llamado estadio 3)
Melanoma en estadio 4 (también llamado estadio IV)
El melanoma puede recidivar (regresar) después de haber sido tratado.
El estadio del cáncer describe la extensión de la enfermedad en el cuerpo, como el tamaño del tumor, si se ha propagado y, en caso de que sí, hastá donde. Es importante conocer el estadio del melanoma para planificar el tratamiento.
Existen varios sistemas de estadificación del cáncer que describen la extensión de la enfermedad. La estadificación del melanoma generalmente utiliza el sistema de estadificación TNM. El cáncer puede describirse mediante este sistema de estadificación en el informe patológico. Según los resultados, se le asigna un estadio (1, 2, 3 o 4, también escrito como I, II, III o IV) al cáncer. Cuando el médico hable con usted sobre su diagnóstico, describirá su cáncer utilizando uno de estos estadios.
El estadio del melanoma depende del espesor del tumor, de si el cáncer se ha diseminado a los ganglios linfáticos o a otras partes del cuerpo y de otros factores.
Para determinar el estadio del melanoma, se extirpa por completo el tumor y se examinan los ganglios linfáticos cercanos para detectar signos de cáncer. El estadio del cáncer se utiliza para determinar cuál será el tratamiento más adecuado. Consulte con su médico para conocer en qué estadio del cáncer se encuentra.
El estadio del melanoma depende de:
El espesor del tumor, que se mide desde la superficie de la piel hasta su parte más profunda. Ampliar
Si el tumor está ulcerado (ha atravesado la piel). Ampliar
Si se detecta la presencia de cáncer en los ganglios linfáticos, ya sea durante un reconocimiento físico, al realizar una prueba de diagnóstico por imágenes, o una biopsia de ganglio linfático centinela. Ampliar
Si los ganglios linfáticos están adheridos (unidos entre sí). Ampliar
Si hay:
Tumores satélite: son pequeños grupos de células tumorales que se han diseminado dentro de los 2 centímetros del tumor primario.
Tumores microsatélite: son pequeños grupos de células tumorales que se han diseminado a un área justo al lado o debajo del tumor primario.
Metástasis en tránsito: significa que se han diseminado los tumores a los vasos linfáticos de la piel a más de 2 centímetros de distancia del tumor primario, pero no a los ganglios linfáticos.
El melanoma se puede estadificar de la siguiente manera:
Estadio 0 (melanoma in situ)
En el estadio 0, se encuentran melanocitos anormales en la epidermis. Estos melanocitos anormales pueden volverse cancerosos y propagarse al tejido normal cercano. El estadio 0 también se denomina melanoma in situ.
Melanoma en estadio 0. Los melanocitos anómalos se encuentran en la epidermis (capa externa de la piel). Estos melanocitos pueden convertirse en cáncer y diseminarse al tejido normal cercano.
Melanoma en estadio I (también llamado estadio 1)
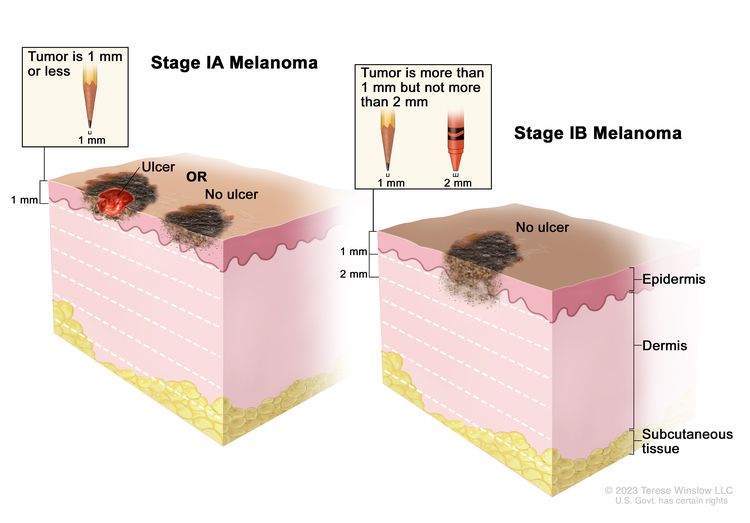
En la etapa I, el cáncer ya se ha formado. La etapa I se divide en etapas IA y IB.
Melanoma en estadio I: en el estadio IA, el tumor no mide más de 1 milímetro de espesor, con o sin ulceración (una ruptura en la piel). En el estadio IB, el tumor mide entre 1 y 2 milímetros de espesor, sin ulceración. El grosor de la piel varía según la parte del cuerpo.
Melanoma en estadio II (también llamado estadio 2)
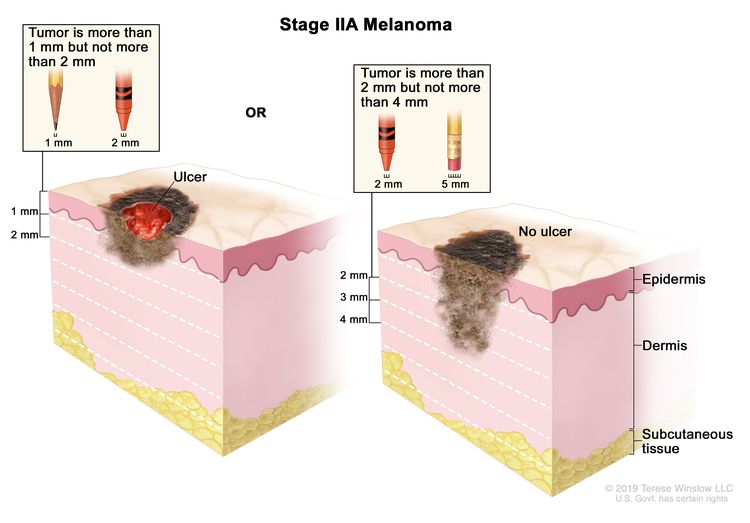
El estadio II se divide en los estadios IIA, IIB y IIC.
En el estadio IIA, el tumor tiene alguna de las siguientes medidas:
Melanoma en estadio IIA: el tumor entre 1 y 2 milímetros de espesor, con ulceración (una ruptura en la piel) O tiene entre 2 y 4 milímetros de espesor, sin ulceración. El grosor de la piel varía según la parte del cuerpo.
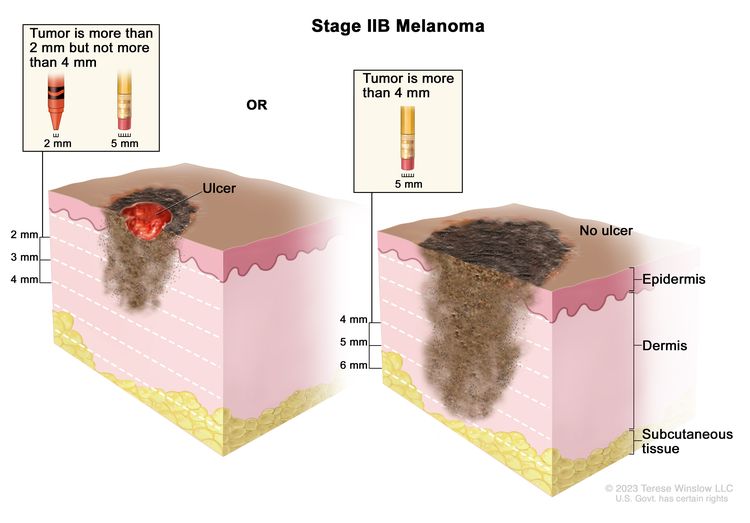
En el estadio IIB, el tumor tiene alguna de las siguientes medidas:
Melanoma en estadio IIB: el tumor tiene entre 2 y 4 milímetros de espesor, con ulceración (una ruptura en la piel) O tiene más de 4 milímetros de espesor, sin ulceración. El grosor de la piel varía según la parte del cuerpo.
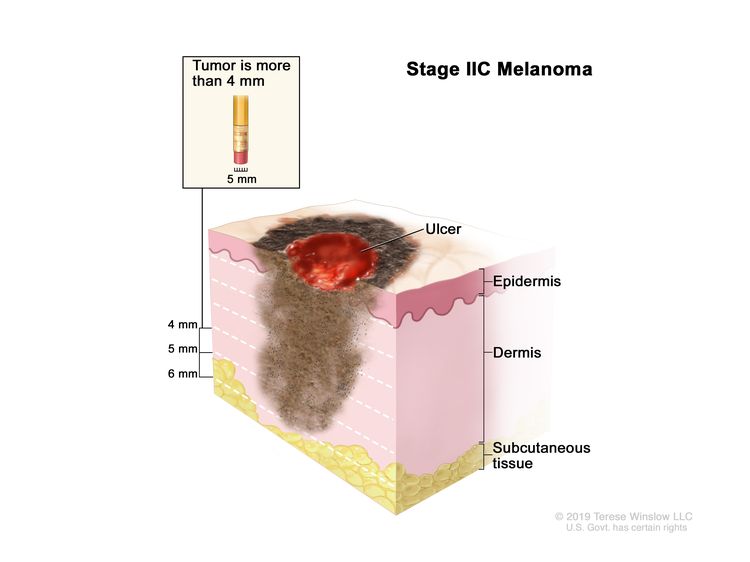
En el estadio IIC, el tumor mide más de 4 milímetros de espesor, con ulceración.
Melanoma en estadio IIC. El tumor tiene más de 4 milímetros de espesor, con ulceración (una ruptura en la piel). El grosor de la piel varía según la parte del cuerpo.
Melanoma en estadio III (también llamado estadio 3)
El estadio III se divide en los estadios IIIA, IIIB, IIIC y IIID.
(2) El tumor no mide más de 1 milímetro de espesor, con ulceración, o no más de 2 milímetros de espesor, sin ulceración, y se presenta alguna de las siguientes situaciones:
Se detecta cáncer en uno a tres ganglios linfáticos mediante un reconocimiento físico o diagnóstico por imágenes.
Hay tumores microsatélite, tumores satélite y/o metástasis en tránsito sobre o debajo de la piel.
o
(3) El tumor tiene entre 1 y 2 milímetros de espesor, con ulceración, o entre 2 y 4 milímetros de espesor, sin ulceración, y se presenta alguna de las siguientes situaciones:
El cáncer se encuentra en uno a tres ganglios linfáticos.
Hay tumores microsatélite, tumores satélite y/o metástasis en tránsito sobre o debajo de la piel.
Estadio IIIC:
(1) No se sabe dónde comenzó el cáncer y el tumor primario ya no se puede ver. El cáncer se encuentra:
En cuatro o más ganglios linfáticos o en cualquier grupo ganglionar que esté adherido entre sí.
En dos o más ganglios linfáticos y/o en cualquier grupo ganglionar que esté adherido entre sí. Hay tumores microsatélite, tumores satélite y/o metástasis en tránsito sobre o debajo de la piel.
o
(2) El tumor no tiene más de 2 milímetros de espesor, con o sin ulceracióno no más de 4 milímetros de espesor, sin ulceración. El cáncer se encuentra:
En un ganglio linfático y hay tumores microsatélite, tumores satélite y/o metástasis en tránsito sobre o debajo de la piel.
En cuatro o más ganglios linfáticos o en cualquier grupo ganglionar que esté adherido entre sí.
En dos o más ganglios linfáticos y/o en cualquier grupo ganglionar que esté adherido entre sí. Hay tumores microsatélite, tumores satélite y/o metástasis en tránsito sobre o debajo de la piel.
o
(3) El tumor tiene un espesor de entre 2 y 4 milímetros, con ulceración, o más de 4 milímetros, sin ulceración. El cáncer se encuentra en uno o más ganglios linfáticos y/o en cualquier grupo ganglionar que esté adherido entre sí. Puede haber tumores microsatélite, tumores satélite y/o metástasis en tránsito sobre o debajo de la piel.
o
(4) El tumor tiene más de 4 milímetros de espesor, con ulceración. El cáncer se encuentra en uno o más ganglios linfáticos y/o hay tumores microsatélite, tumores satélite y/o metástasis en tránsito sobre o debajo de la piel.
Estadio IIID: el tumor mide más de 4 milímetros de espesor, con ulceración. Se detecta cáncer:
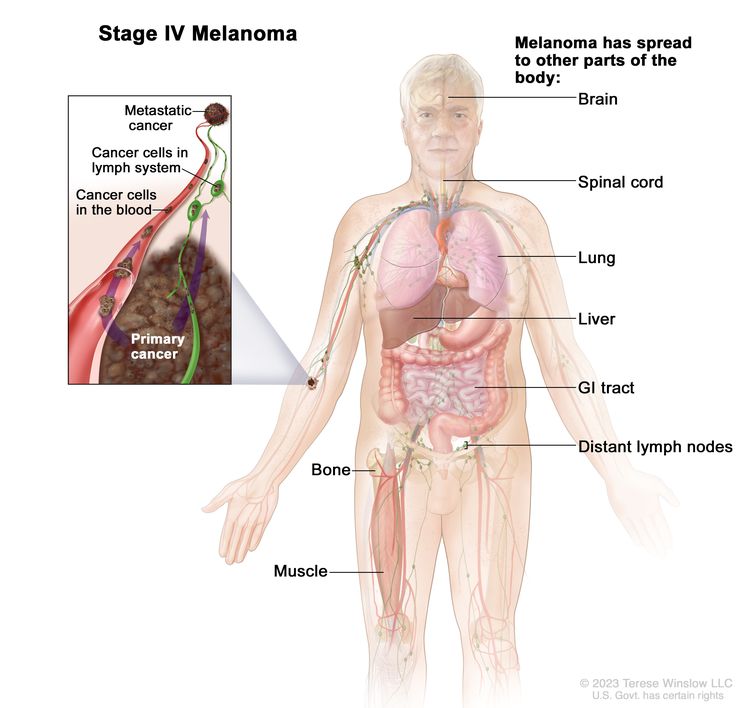
El melanoma en estadio IV también se denomina melanoma metastásico. El cáncer metastásico se produce cuando las células cancerosas se desplazan por el sistema linfático o la sangre y forman tumores en otras partes del cuerpo. El tumor metastásico es el mismo tipo de cáncer que el tumor primario. Por ejemplo, si el melanoma se propaga al pulmón, las células cancerosas en el pulmón son en realidad células de melanoma. La enfermedad se denomina melanoma metastásico, no cáncer de pulmón. Obtenga más información en Cáncer metastásico: Cuando el cáncer se propaga .
Melanoma en estadio IV: el cáncer se ha propagado a otras partes del cuerpo, como el cerebro, la médula espinal, los pulmones, el hígado, el tracto gastrointestinal (GI), los huesos, los músculos o los ganglios linfáticos distantes. Es posible que el cáncer se haya diseminado a lugares de la piel que están alejados del lugar donde se originó.
El melanoma puede recidivar (regresar) después de haber sido tratado.
El melanoma recurrente es un melanoma que ha reaparecido después de haber sido tratado. Si el melanoma regresa, puede hacerlo en la zona donde se originó o en otras partes del cuerpo, como los pulmones o el hígado . Las pruebas ayudarán a determinar en qué parte del cuerpo ha regresado el cáncer. El tipo de tratamiento que reciba para el melanoma recurrente dependerá de dónde haya reaparecido.
Existen diferentes tipos de tratamiento para personas con melanoma.
The following types of treatment are used:
Cirugía
Quimioterapia
Radioterapia
Inmunoterapia
Terapia dirigida
New types of treatment are being tested in clinical trials.
Terapia de vacunas
El tratamiento del melanoma puede producir efectos secundarios.
Es posible que se necesiten cuidados de seguimiento.
Existen diferentes tipos de tratamiento para personas con melanoma.
Existen diferentes tipos de tratamiento para las personas con melanoma. Algunos tratamientos son estándar (el tratamiento que se utiliza actualmente) y otros se están probando en ensayos clínicos . Un ensayo clínico de tratamiento es un estudio de investigación cuyo objetivo es mejorar los tratamientos actuales u obtener información sobre nuevos tratamientos para personas con cáncer. Cuando los ensayos clínicos demuestran que un nuevo tratamiento es mejor que el tratamiento estándar, este puede convertirse en el tratamiento estándar. Es posible que las personas consideren participar en un ensayo clínico. Algunos ensayos clínicos están abiertos solo a personas que no han comenzado el tratamiento.
The following types of treatment are used:
Cirugía
La cirugía para extirpar el tumor es el tratamiento principal para todos los estadios del melanoma. Se utiliza una escisión local amplia para extirpar el melanoma y parte del tejido normal que lo rodea. Se puede realizar un injerto de piel (tomar piel de otra parte del cuerpo para reemplazar la piel que se extrae) para cubrir la herida causada por la cirugía.
Si solo se encuentra una pequeña cantidad de células cancerosas durante una biopsia del ganglio linfático centinela, se puede recomendar llevar a cabo una vigilancia activa con ultrasonido en lugar de más cirugía.
Después de que el médico extirpe todo el melanoma visible en el momento de la cirugía, algunas personas podrían recibir quimioterapia para eliminar cualquier célula cancerosa restante. La quimioterapia administrada después de la cirugía para reducir el riesgo de reaparición del cáncer se denomina terapia adyuvante .
La quimioterapia (también llamada quimio) utiliza medicamentos para detener el crecimiento de las células cancerosas, ya sea destruyéndolas o impidiendo su división. Cuando la quimioterapia se administra por vía oral o se inyecta en una vena o músculo, los medicamentos ingresan al torrente sanguíneo y pueden alcanzar las células cancerosas de todo el cuerpo ( quimioterapia sistémica ). Cuando la quimioterapia se administra directamente en el líquido cefalorraquídeo, un órgano o una cavidad corporal como el abdomen, los medicamentos afectan principalmente a las células cancerosas en esas áreas (quimioterapia regional).
Un tipo de quimioterapia regional es la perfusión aislada de una extremidad con hipertermia. Con este método, los medicamentos para el cáncer se dirigen directamente al brazo o la pierna donde se encuentra la enfermedad. El flujo de sangre hacia y desde la extremidad se detiene temporalmente con un torniquete. Se coloca una solución tibia con el medicamento directamente en la sangre de la extremidad. Esto proporciona una dosis alta de medicamentos al área donde se encuentra el cáncer.
La forma en que se administra la quimioterapia depende del tipo y estadio del cáncer que se esté tratando.
La radioterapia utiliza rayos X de alta energía u otros tipos de radiación para destruir las células cancerosas o impedir su crecimiento. La radioterapia externa utiliza una máquina externa al cuerpo para enviar radiación hacia la zona con cáncer. La radioterapia externa se utiliza para tratar el melanoma y también puede utilizarse como terapia paliativa para aliviar los síntomas y mejorar la calidad de vida.
Immunotherapy helps a person's immune system fight cancer. Your doctor may suggest biomarker tests to help predict your response to certain immunotherapy drugs. Learn more about Biomarker Testing for Cancer Treatment.
Los medicamentos de inmunoterapia utilizados para tratar el melanoma son:
Targeted therapy uses drugs or other substances to identify and attack specific cancer cells. Your doctor may suggest biomarker tests to help predict your response to certain targeted therapy drugs. Learn more about Biomarker Testing for Cancer Treatment.
Las terapias dirigidas utilizadas para tratar el melanoma son:
New types of treatment are being tested in clinical trials.
Terapia de vacunas
La terapia con vacunas es un tratamiento para el cáncer que utiliza una sustancia o un grupo de ellas para estimular el sistema inmunitario a fin de que detecte el tumor y lo elimine. La terapia con vacunas se está estudiando para el tratamiento del melanoma en estadio III que se puede extirpar mediante cirugía.
El tratamiento del melanoma puede producir efectos secundarios.
Es posible que se necesiten cuidados de seguimiento.
A medida que avanza el tratamiento, se le realizarán pruebas o controles de seguimiento. Es posible que se repitan algunas pruebas para diagnosticar o estadificar el cáncer con el fin de evaluar cómo está funcionando el tratamiento. Las decisiones sobre si continuar, modificar o suspender el tratamiento pueden basarse en los resultados de estas pruebas.
Algunas pruebas seguirán realizándose de manera periódica después de terminar el tratamiento. Los resultados pueden indicar si su afección ha cambiado o si el cáncer ha redicivado (regresado).
Tratamiento del estadio 0 (Melanoma in Situ)
El tratamiento del estadio 0 suele consistir en una cirugía para extirpar el área de células anómalas y una pequeña cantidad de tejido normal a su alrededor.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del melanoma en estadio II
El tratamiento del melanoma en estadio II puede consistir en:
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del melanoma en estadio III que se puede extirpar mediante cirugía
El tratamiento del melanoma en estadio III que se puede extirpar mediante cirugía puede consistir en:
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tratamiento del melanoma en estadio III que no se puede extirpar mediante cirugía, melanoma en estadio III y melanoma recidivante
El tratamiento del melanoma en estadio III que no se puede extirpar mediante cirugía, el melanoma en estadio IV y el melanoma recurrente puede incluir:
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen del PDQ sobre el cáncer contiene información actualizada del tratamiento del melanoma. El propósito es informar y ayudar a los pacientes, sus familiares y cuidadores. No da pautas ni recomendaciones formales para tomar decisiones relacionadas con la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre el tratamiento para adultos. Tratamiento del melanoma (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA]. Disponible en: https://www.cancer.gov/es/tipos/piel/paciente/tratamiento-del-melanoma-pdq. Consultado el [DD/MM/AAAA]. [PMID: 26389388]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Actualizado:
Este contenido ha sido facilitado por el National Cancer Institute (www.cancer.gov)










; drawing shows different depths of cancer invasion (0, 1.0, 2.0, 3.0, 4.0, and 5.0 mm) into the epidermis (outer layer of the skin), the dermis (inner layer of the skin), and the subcutaneous tissue below the dermis.")
; drawing shows a tumor that is ulcerated (has broken through the skin) and a tumor that is not ulcerated.")
; drawing shows cancer that has spread from the primary tumor to the lymph nodes.")
; drawing shows matted lymph nodes with cancer.")
; drawing shows in-transit metastases in a lymph vessel more than 2 centimeters away from the primary tumor and satellite tumors within 2 centimeters of the primary tumor. Microsatellite tumors are not shown because they can only be seen with a microscope.")
; drawing shows cancer cells spreading from the primary cancer, through the blood and lymph system, to another part of the body where a metastatic tumor has formed.")