








Tratamiento del cáncer de mama en hombres
Obtenga una atención excepcional para el cáncer de mama en hombres en el Montefiore Einstein Comprehensive Cancer Center. Como uno de los primeros centros del cáncer designados por el NCI, llevamos más de 50 años liderando en la investigación, el diagnóstico y el tratamiento de más de 200 tipos de cáncer.
Encuentre atención integral y personalizada de algunos de los principales expertos en cáncer de mama del país. El Montefiore Einstein Comprehensive Cancer Center está clasificado dentro del 1 % de los mejores hospitales del país en atención médica del cáncer según U.S. News & World Report . Nuestro programa de cáncer de mama también está acreditado por el Programa Nacional de Acreditación para Centros de Cáncer de Mama (NAPBC), siguiendo los estándares más altos para la atención cáncer de mama de calidad.
Usted será el centro de atención de un equipo multidisciplinario de especialistas en cáncer de mama compuesto por oncólogos médicos, oncólogos quirúrgicos, cirujanos plásticos y reconstructivos, radioterapeutas y otros profesionales dedicados. Puede confiar en que su equipo le recomendará y le ofrecerá las opciones de tratamiento más innovadoras y efectivas que utilizan la tecnología más avanzada disponible para diagnosticar y tratar el cáncer de mama, así como atención de apoyo y recursos para mejorar su bienestar. También se beneficiará del trabajo de un equipo de investigación clínica en cáncer de mama que está definiendo el futuro de la atención mediante descubrimientos científicos, colaboraciones con grupos de investigación nacionales e internacionales y acciones de defensa que buscan eliminar las barreras de acceso a la atención.
Cuando elija a Montefiore Einstein Comprehensive Cancer Center para el tratamiento del cáncer de mama, usted se beneficiará de:
- Las pruebas de diagnóstico, tratamientos y tecnología avanzada más innovadores y efectivos, entre ellos:
- Pruebas de diagnóstico en el mismo día para mamografía utilizando tomosíntesis 3D de última generación, ultrasonido y biopsia con aguja mínimamente invasiva
- Navegación quirúrgica para la cirugía de conservación de mama, lo que nos convierte en uno de los pocos programas de cáncer de mama en EE. UU. que ofrece esta opción, que le permite alcanzar el mejor resultado en la menor cantidad de cirugías posible.
- Técnicas de radioterapia, como tratamientos de radiación de dosis única durante la cirugía, para tratar el cáncer más rápidamente que la radioterapia tradicional
- Técnicas de lumpectomía que usan tecnología de imágenes durante la cirugía para extirpar completamente el cáncer en el 90 % de los pacientes, más que el promedio nacional del 65 % en otros programas.
- Acceso a nuevos tratamientos prometedores a través de ensayos clínicos
- Prevención y terapias de linfedema de renombre mundial, como el enfoque curativo preventivo microquirúrgico linfático (LYMPHA), que se desarrolló en nuestro centro del cáncer.
- Enfoque de atención holístico y centrado en el paciente, incluida la atención integral y de apoyo, recursos para mejorar su bienestar y citas combinadas el mismo día para su comodidad.
- Entorno moderno y tranquilo diseñado para promover su curación
- Educación y apoyo para tomar decisiones informadas sobre su atención
Cuando necesite atención para el cáncer de mama, recurra a nuestros proveedores que se apasionan por acabar con el cáncer y abordar todas sus necesidades de salud.
Acuda al Centro de Salud Mamaria para recibir una atención médica coordinada y especializada en un entorno moderno, acceder a algunos de los mejores especialistas multidisciplinarios del país y contar con toda la información y orientación personalizada que necesita para dar los próximos pasos.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Tratamiento del cáncer de mama en hombres (PDQ®): versión para pacientes
Información general sobre el cáncer de mama en hombres
Puntos clave
- El cáncer de mama en hombres es una enfermedad en la que se forman células malignas (cancerosas) en los tejidos de la mama.
- Un historial de salud familiar de cáncer de mama y otros factores pueden aumentar el riesgo de que un hombre desarrolle la enfermedad.
- El cáncer de mama en hombres a veces está causado por mutaciones (cambios) genéticos hereditarios.
- Los hombres con cáncer de mama generalmente presentan bultos que se pueden palpar.
- Para diagnosticar el cáncer de mama en los hombres se utilizan pruebas que examinan las mamas.
- Si se detecta cáncer, se realizan pruebas para estudiar las células cancerosas.
- La supervivencia de los hombres con cáncer de mama es similar a la supervivencia de las mujeres con la misma enfermedad.
- Certain factors affect prognosis (chance of recovery) and treatment options.
El cáncer de mama en hombres es una enfermedad en la que se forman células malignas (cancerosas) en los tejidos de la mama.
El cáncer de mama puede presentarse en hombres de cualquier edad, pero en general afecta a hombres de entre 60 y 70 años. El cáncer de mama en hombres representa menos del 1 % de todos los casos de cáncer de mama.
A continuación se detallan los tipos de cáncer de mama que se presentan en los hombres:
- Carcinoma ductal infiltrante: el cáncer se ha propagado fuera de las células que recubren los conductos de la mama. Es el tipo de cáncer de mama más común en los hombres.
- Carcinoma ductal in situ: hay presencia de células anómalas en el revestimiento de un conducto. También se denomina carcinoma intraductal.
- Cáncer de mama inflamatorio: es un tipo de cáncer en el que la mama presenta enrojecimiento e hinchazón y se siente caliente.
- Enfermedad de Paget del pezón: es un tumor que ha crecido desde los conductos debajo del pezón hasta la superficie del mismo.
El carcinoma lobulillar in situ (células anómalas que se encuentran en uno de los lóbulos o secciones de la mama), que a veces se presenta en mujeres, no se ha observado en hombres.
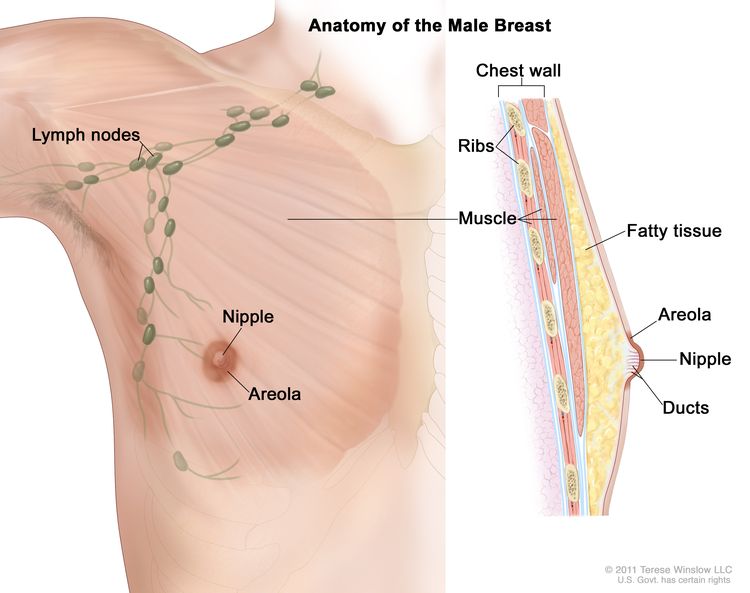
Anatomía de la mama masculina. El pezón y la areola se muestran en la parte exterior de la mama. También se muestran los ganglios linfáticos, el tejido adiposo, los conductos y otras partes del interior de la mama.
Un historial de salud familiar de cáncer de mama y otros factores pueden aumentar el riesgo de que un hombre desarrolle la enfermedad.
Todo lo que aumenta el riesgo de desarrollar una enfermedad se denomina factor de riesgo. Tener un factor de riesgo no significa que desarrollará la enfermedad; no tener factores de riesgo tampoco significa que no lo hará. Hable con su médico si cree que puede estar en riesgo. Los factores de riesgo de cáncer de mama en hombres pueden ser:
- Tratamiento con radioterapia en la mama o el tórax
- Tener una enfermedad relacionada con niveles elevados de estrógeno en el cuerpo, como cirrosis (enfermedad hepática) o síndrome de Klinefelter (un trastorno genético)
- Tener una o más familiares mujeres que hayan tenido cáncer de mama.
- Tener mutaciones (cambios) en genes como BRCA2
El cáncer de mama en hombres a veces está causado por mutaciones (cambios) genéticos hereditarios.
Los genes en las células portan la información hereditaria que se recibe de los padres. El cáncer de mama hereditario representa entre el 5 % y el 10 % de todos los casos. Algunos genes mutados relacionados con el cáncer de mama, como el BRCA2, son más comunes en ciertos grupos étnicos. Los hombres que tienen un gen mutado relacionado con el cáncer de mama tienen un mayor riesgo de padecer esta enfermedad.
Existen pruebas que pueden detectar (encontrar) genes mutados. Estas pruebas genéticas a veces se realizan a miembros de familias con un riesgo elevado de desarrollar cáncer. Consulte los siguientes resúmenes del PDQ para obtener más información:
Los hombres con cáncer de mama generalmente presentan bultos que se pueden palpar.
Los bultos y otros signos pueden ser causados por el cáncer de mama en hombres o por otras afecciones. Consulte con su médico si presenta alguno de los siguientes síntomas:
- Un bulto o engrosamiento en la mama o cerca de esta o en el área de la axila
- Un cambio en el tamaño o la forma de la mama
- Un hoyuelo o arrugas en la piel de la mama
- Un pezón invertido hacia el interior de la mama
- Líquido proveniente del pezón, especialmente si tiene sangre
- Piel escamosa, enrojecida o hinchada en la mama, el pezón o la areola (el área oscura de la piel alrededor del pezón)
- Hoyuelos en la mama que hacen que la piel se vea como la de una naranja, lo que se conoce como peau d’orange.
Para diagnosticar el cáncer de mama en los hombres se utilizan pruebas que examinan las mamas.
Se pueden utilizar las siguientes pruebas y procedimientos:
- Reconocimiento físico e historial de salud: un examen del cuerpo para evaluar el estado general de salud, incluida la detección de signos de enfermedad, como bultos o cualquier otra anomalía. También se toma nota de los hábitos de salud del paciente y de sus enfermedades y tratamientos previos.
- Examen clínico de senos (ECS): es un examen de los senos realizado por un médico u otro profesional de la salud. El médico palpará cuidadosamente las mamas y las axilas para detectar bultos o cualquier anomalía.
- Mamografía: es una radiografía de la mama.
- Examen por medio de ecografía: es un procedimiento en el que ondas sonoras de alta energía (ultrasonido) rebotan en tejidos u órganos internos y producen ecos. Los ecos forman una imagen de los tejidos del cuerpo llamada ecografía. La imagen se puede imprimir para su posterior análisis.
- Resonancia magnética (imagen por resonancia magnética): es un procedimiento que utiliza un imán, ondas de radio y una computadora para generar una serie de imágenes detalladas de ambos senos. Este procedimiento también se llama resonancia magnética nuclear (NMRI).
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- Biopsy: es la extracción de células o tejidos para que puedan ser analizados con un microscope por un pathologist para detectar signos de cáncer. Existen cuatro tipos de biopsias para detectar el cáncer de mama:
- Biopsia escisional: extirpación de un bulto completo de tejido
- Biopsia incisional: extracción de parte de un bulto o de una muestra de tejido
- Biopsia central: extracción de tejido mediante una aguja ancha
- Biopsia por aspiración con aguja fina (PAAF): extracción de tejido o líquido con una aguja fina
Si se detecta cáncer, se realizan pruebas para estudiar las células cancerosas.
Las decisiones sobre el tratamiento más adecuado se basan en los resultados de estas pruebas. Las pruebas ofrecen información sobre:
- Qué tan rápido puede crecer el cáncer.
- La probabilidad de que el cáncer se propague por el cuerpo.
- Qué tan bien podrían funcionar ciertos tratamientos.
- La probabilidad de que el cáncer recidive (regrese).
Las pruebas son las siguientes:
- Prueba de receptores de estrógeno y progesterona: es una prueba para medir la cantidad de receptores de estrógeno y progesterona (hormonas) en el tejido canceroso. Si hay más receptores de estrógeno y progesterona de lo normal, el cáncer se denomina positivo para receptores de estrógeno y/o progesterona. Este tipo de cáncer de mama puede crecer más rápidamente. Los resultados de la prueba muestran si el tratamiento para bloquear el estrógeno y la progesterona puede detener el crecimiento del cáncer.
- Prueba de HER2: es una prueba de laboratorio para medir cuántos genes HER2/neu hay y cuánta proteína HER2/neu se produce en una muestra de tejido. Si hay más genes HER2/neu o niveles más altos de la proteína HER2/neu de lo normal, el cáncer se denomina positivo para HER2/neu. Este tipo de cáncer de mama puede crecer más rápidamente y es más probable que se propague a otras partes del cuerpo. Puede tratarse con medicamentos que atacan la proteína HER2/neu, como trastuzumab y pertuzumab.
La supervivencia de los hombres con cáncer de mama es similar a la supervivencia de las mujeres con la misma enfermedad.
La supervivencia de los hombres con cáncer de mama es similar a la de las mujeres cuando el estadio en el momento del diagnóstico es el mismo. Sin embargo, el cáncer de mama en los hombres suele diagnosticarse en un estadio más avanzado. Cuando este es el caso, puede tener menos probabilidades de curarse.
Certain factors affect prognosis (chance of recovery) and treatment options.
El pronóstico y las opciones de tratamiento dependen de los siguientes factores:
- El estadio del cáncer (el tamaño del tumor y si está sólo en la mama o se ha diseminado a los ganglios linfáticos u otras partes del cuerpo).
- El tipo de cáncer de mama
- Niveles de receptores de estrógeno y de progesterona en el tejido tumoral
- Si también se detecta cáncer en la otra mama.
- La edad del hombre y su estado de salud general.
- Si el cáncer se acaba de diagnosticar o recidivó (volvió).
Estadios del cáncer de mama en hombres
Puntos clave
- Después de diagnosticar el cáncer de mama, se realizan pruebas para determinar si las células cancerosas se han diseminado dentro de la mama o a otras partes del cuerpo.
- There are three ways that cancer spreads in the body.
- El cáncer puede extenderse desde donde comenzó a otras partes del cuerpo.
- En el cáncer de mama, el estadio se basa en el tamaño y la ubicación del tumor primario, la propagación del cáncer a los ganglios linfáticos cercanos u otras partes del cuerpo, el grado del tumor y la presencia de ciertos biomarcadores.
- El sistema TNM se usa para describir el tamaño del tumor primario y la diseminación del cáncer a los ganglios linfáticos cercanos u otras partes del cuerpo.
- Tumor (T): el tamaño y la ubicación del tumor
- Nódulos linfáticos (N): el tamaño y la ubicación de los ganglios linfáticos a los que se ha propagado el cáncer.
- Metástasis (M): la propagación del cáncer a otras partes del cuerpo
- El sistema de gradación se usa para describir qué tan rápido es probable que un tumor de mama crezca y se propague.
- La prueba de biomarcadores se utiliza para determinar si las células del cáncer de mama tienen ciertos receptores.
- El sistema TNM, el sistema de gradación y el estado de los biomarcadores se combinan para determinar el estadio del cáncer de mama.
- Hable con su médico para saber cuál es su estadio de cáncer de mama y cómo se utiliza para planificar el tratamiento más adecuado para usted.
- El tratamiento del cáncer de mama en hombres depende en parte del estadio de la enfermedad.
Después de diagnosticar el cáncer de mama, se realizan pruebas para determinar si las células cancerosas se han diseminado dentro de la mama o a otras partes del cuerpo.
Después de que se ha diagnosticado el cáncer de mama, se realizan pruebas para determinar si las células cancerosas se han propagado dentro de la mama o a otras partes del cuerpo. Este proceso se llama estadificación. La información obtenida en este proceso determina el estadio de la enfermedad. Es importante conocer el estadio para planificar el tratamiento. El cáncer de mama en los hombres se estadifica de la misma manera que en las mujeres. La propagación del cáncer desde la mama a los ganglios linfáticos y otras partes del cuerpo parece ser similar en hombres y mujeres.
En el proceso de estadificación pueden utilizarse las siguientes pruebas y procedimientos:
- Biopsia del ganglio linfático centinela: consiste en la extirpación del ganglio linfático centinela durante la cirugía. El ganglio linfático centinela es el primer ganglio linfático de un grupo ganglionar que recibe drenaje linfático del tumor primario. Es el primer ganglio linfático al que es probable que se propague el cáncer desde el tumor primario. Se inyecta una sustancia radiactiva y/o un tinte azul cerca del tumor. La sustancia o tinte fluye a través de los conductos linfáticos hasta los ganglios linfáticos. Se extirpa el primer ganglio linfático que recibirá la sustancia o el tinte. Un patólogo observa el tejido bajo un microscopio para buscar células cancerosas. Si no se encuentran, es posible que no sea necesario extirpar más ganglios linfáticos. A veces, hay un ganglio linfático centinela en más de un grupo de ganglios.
- Radiografía del tórax: radiografía de los órganos y huesos del interior del tórax. Los rayos X son un tipo de haz de energía que puede atravesar el cuerpo, plasmarse en una película y generar una imagen de áreas del interior del cuerpo.
- Exploración por tomografía computarizada (TAC): es un procedimiento que genera una serie de imágenes detalladas de áreas internas del cuerpo, tomadas desde diferentes ángulos. Las imágenes son tomadas por una computadora conectada a una máquina de rayos X. Se puede inyectar un tinte en una vena o ingerirlo para permitir que los órganos o tejidos se visualicen con más claridad. Este procedimiento también se llama tomografía axial computarizada.
- Exploración ósea: es un procedimiento para comprobar si hay células que se dividen rápidamente, como células cancerosas, en el hueso. Se inyecta una cantidad muy pequeña de material radiactivo en una vena y viaja a través del torrente sanguíneo. El material radiactivo se acumula en los huesos con cáncer y es detectado por un escáner.
- Exploración PET (tomografía por emisión de positrones): es un procedimiento para encontrar células tumorales malignas en el cuerpo. Se inyecta una pequeña cantidad de glucosa (azúcar) radiactiva en una vena. El escáner PET gira alrededor del cuerpo y genera una imagen del lugar donde más se utiliza la glucosa en el cuerpo. Las células tumorales malignas aparecen más brillantes en la imagen porque presentar un mayor nivel de actividad y absorben más glucosa que las células normales.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
El cáncer puede extenderse desde donde comenzó a otras partes del cuerpo.
Cuando el cáncer se extiende a otra parte del cuerpo se denomina metástasis. Las células cancerosas se desprenden de donde comenzaron (tumor primario) y viajan a través del sistema linfático o la sangre.
- Sistema linfático: el cáncer entra en el sistema linfático, viaja a través de los vasos linfáticos y forma un tumor (tumor metastásico) en otra parte del cuerpo.
- Sangre: el cáncer llega a la sangre, viaja a través de los vasos sanguíneos y forma un tumor (tumor metastásico) en otra parte del cuerpo.
El tumor metastásico es el mismo tipo de cáncer que el tumor primario. Por ejemplo, si el cáncer de mama se propaga al hueso, las células cancerosas del hueso son, en realidad, células de cáncer de mama. La enfermedad es cáncer de mama metastásico, en lugar de cáncer de hueso.
En el cáncer de mama, el estadio se basa en el tamaño y la ubicación del tumor primario, la propagación del cáncer a los ganglios linfáticos cercanos u otras partes del cuerpo, el grado del tumor y la presencia de ciertos biomarcadores.
Para planificar el mejor tratamiento posible y comprender su pronóstico, es importante conocer el estadio del cáncer de mama.
Existen tres tipos de grupos de estadios del cáncer de mama:
- El estadio pronóstico clínico se utiliza inicialmente para asignar un estadio a todos los pacientes según su historial de salud, un reconocimiento físico, las pruebas de diagnóstico por imágenes (si se realizan) y las biopsias. El estadio pronóstico clínico se describe mediante el sistema TNM, el grado del tumor y el estado de los biomarcadores (ER, PR, HER2). En la estadificación clínica, se utiliza la mamografía o la ecografía para examinar los ganglios linfáticos en busca de signos de cáncer.
- El estadio pronóstico patológico se utiliza luego para pacientes que se realicen una cirugía como primer tratamiento. El estadio pronóstico patológico se basa en toda la información clínica, el estado de los biomarcadores y los resultados de las pruebas de laboratorio del tejido mamario y los ganglios linfáticos extirpados durante la cirugía.
- El estadio anatómico se basa en el tamaño y la propagación del cáncer según lo describe el sistema TNM. El estadio anatómico se utiliza en partes del mundo donde las pruebas de biomarcadores no están disponibles. No se utiliza en Estados Unidos.
El sistema TNM se usa para describir el tamaño del tumor primario y la diseminación del cáncer a los ganglios linfáticos cercanos u otras partes del cuerpo.
En el caso del cáncer de mama, el sistema TNM describe el tumor de la siguiente manera:
Tumor (T): el tamaño y la ubicación del tumor
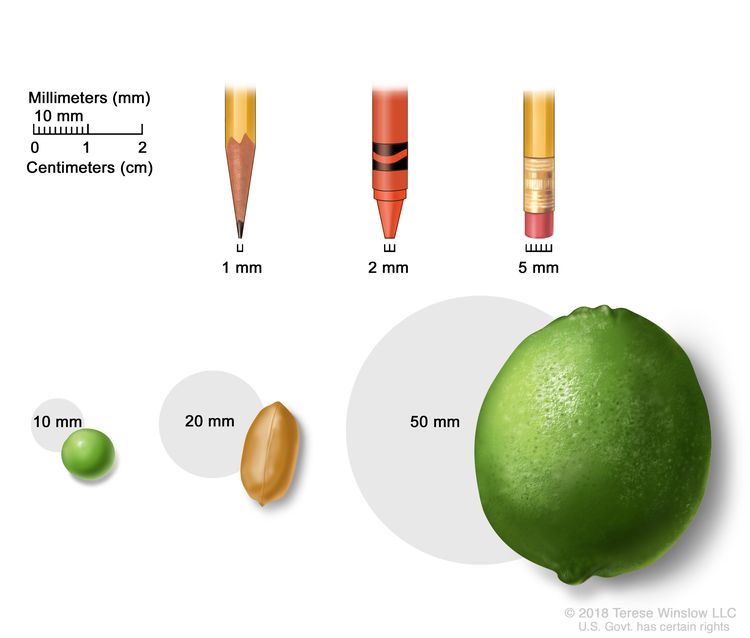
A menudo, el tamaño de los tumores se miden en milímetros (mm) o centímetros. Los elementos comunes que se pueden usar para mostrar el tamaño del tumor en mm son: una punta de lápiz afilada (1 mm), una punta de un crayón nuevo (2 mm), un borrador de lápiz (5 mm), un guisante (10 mm), un maní (20 mm) y una lima (50 mm).
- TX: no se puede evaluar el tumor primario.
- T0: no hay signos de un tumor primario en la mama.
- Tis: carcinoma in situ: hay dos tipos de carcinoma de mama in situ:
- Tis (DCIS): el CDIS es una afección en la que hay presencia de células anómalas en el revestimiento de un conducto mamario. Las células anómalas no se han propagado fuera del conducto a otros tejidos de la mama. En algunos casos, el CDIS puede convertirse en cáncer de mama invasivo que puede propagarse a otros tejidos. En este momento, no hay forma de saber qué lesiones pueden volverse invasivas.
- Tis (enfermedad de Paget): la enfermedad de Paget del pezón es una afección en la que hay presencia de células anómalas en las células de la piel del pezón y pueden propagarse a la areola. No se clasifica según el sistema TNM. Si hay enfermedad de Paget Y cáncer de mama invasivo, se utiliza el sistema TNM para clasificar el cáncer de mama invasivo.
- T1: el tumor mide 20 milímetros o menos. Hay cuatro subtipos de un tumor T1 dependiendo del tamaño del tumor:
- T1mi: el tumor mide 1 milímetro o menos.
- T1a: el tumor mide más de 1 milímetro, pero no más de 5 milímetros.
- T1b: el tumor mide más de 5 milímetros, pero no más de 10 milímetros.
- T1c: el tumor mide más de 10 milímetros, pero no más de 20 milímetros.
- T2: el tumor mide más de 20 milímetros, pero no más de 50 milímetros.
- T3: el tumor mide más de 50 milímetros.
- T4: el tumor se describe como uno de los siguientes:
- T4a: el tumor ha crecido hacia la pared torácica.
- T4b: el tumor ha invadido la piel: se ha formado una úlcera en la superficie de la piel de la mama, se han formado pequeños nódulos tumorales en la misma mama que el tumor primario y/o hay hinchazón de la piel de la mama.
- T4c: el tumor ha crecido hacia la pared torácica y la piel.
- T4d: cáncer de mama inflamatorio: un tercio o más de la piel de la mama está roja e hinchada (lo que se denomina peau d'orange).
Nódulos linfáticos (N): el tamaño y la ubicación de los ganglios linfáticos a los que se ha propagado el cáncer.
Cuando se extirpan los ganglios linfáticos mediante cirugía y un patólogo los estudia bajo un microscopio, se utiliza la estadificación patológica para describirlos. A continuación se describe la estadificación patológica de los ganglios linfáticos.
- NX: no se pueden evaluar los ganglios linfáticos.
- N0: no hay signos de cáncer en los ganglios linfáticos o solo hay pequeños grupos de células cancerosas de no más de 0.2 milímetros en ellos.
- N1: el cáncer se describe como uno de los siguientes:
- N1mi: el cáncer se ha diseminado a los ganglios linfáticos axilares (área de la axila) y mide más de 0.2 milímetros, pero no más de 2 milímetros.
- N1a: el cáncer se diseminó a entre uno y tres ganglios linfáticos axilares y el cáncer en al menos uno de los ganglios linfáticos mide más de 2 milímetros.
- N1b: el cáncer se ha diseminado a los ganglios linfáticos cerca del esternón en el mismo lado del cuerpo que el tumor primario. El cáncer mide más de 0.2 milímetros y se detecta mediante una biopsia del ganglio linfático centinela; no está presente en los ganglios linfáticos axilares.
- N1c: el cáncer se diseminó a entre uno y tres ganglios linfáticos axilares y el cáncer en al menos uno de los ganglios linfáticos mide más de 2 milímetros. También se detecta cáncer en una biopsia de ganglio linfático centinela en los ganglios linfáticos cerca del esternón en el mismo lado del cuerpo que el tumor primario.
- N2: el cáncer se describe como uno de los siguientes:
- N2a: el cáncer se diseminó a entre cuatro y nueve ganglios linfáticos axilares y, en al menos uno de los ganglios linfáticos, mide más de 2 milímetros.
- N2b: el cáncer se ha diseminado a los ganglios linfáticos cerca del esternón y se detecta mediante pruebas de imagen. No se detecta cáncer en los ganglios linfáticos axilares mediante una biopsia del ganglio linfático centinela o una disección de los ganglios linfáticos.
- N3: el cáncer se describe como uno de los siguientes:
- N3a: el cáncer se ha diseminado a diez o más ganglios linfáticos axilares y, en al menos uno de los ganglios linfáticos, mide más de 2 milímetros o se ha diseminado a los ganglios linfáticos debajo de la clavícula.
- N3b: el cáncer se diseminó a entre uno y nueve ganglios linfáticos axilares y, en al menos uno de los ganglios linfáticos, mide más de 2 milímetros. También se diseminó a los ganglios linfáticos cerca del esternón y se detecta mediante pruebas de imagen.
o
El cáncer se diseminó a entre cuatro y nueve ganglios linfáticos axilares y, en al menos uno de los ganglios linfáticos, mide más de 2 milímetros. También se diseminó a los ganglios linfáticos cerca del esternón en el mismo lado del cuerpo que el tumor primario y mide más de 0.2 milímetros; se detecta mediante una biopsia de ganglio linfático centinela.
- N3c: el cáncer se diseminó a los ganglios linfáticos por encima de la clavícula en el mismo lado del cuerpo que el tumor primario.
Cuando los ganglios linfáticos se examinan mediante mamografía o ecografía, se denomina estadificación clínica. La estadificación clínica de los ganglios linfáticos no se describe en esta página.
Metástasis (M): la propagación del cáncer a otras partes del cuerpo
- M0: no hay señales de que el cáncer se haya propagado a otras partes del cuerpo.
- M1: el cáncer se ha propagado a otras partes del cuerpo, con mayor frecuencia a los huesos, los pulmones, el hígado o el cerebro. Si el cáncer se ha propagado a ganglios linfáticos distantes, el cáncer en ellos mide más de 0.2 milímetros. El cáncer se denomina cáncer de mama metastásico.
El sistema de gradación se usa para describir qué tan rápido es probable que un tumor de mama crezca y se propague.
El sistema de gradación describe un tumor basándose en cuán anómalas se ven las células y el tejido canceroso bajo un microscopio y qué tan rápido es probable que las células crezcan y se propaguen. Las células cancerosas de bajo grado se parecen más a las células normales y tienden a crecer y diseminarse más lentamente que las de alto grado. Para describir cuán anómalas son las células y el tejido canceroso, el patólogo evaluará las tres características siguientes:
- Qué proporción del tejido tumoral conserva conductos mamarios normales.
- El tamaño y la forma de los núcleos de las células tumorales
- Cuántas células en división están presentes, lo cual indica la velocidad con que las células del tumor crecen y se dividen.
Para cada característica, el patólogo asigna una puntuación del 1 a 3; una puntuación de 1 significa que las células y el tejido tumoral se parecen más a las células y el tejido normales, mientras que una puntuación de 3 significa que las células y el tejido tienen una apariencia más anómala. Las puntuaciones de cada característica se suman para obtener una puntuación total entre 3 y 9.
Hay tres grados posibles:
- Puntuación total de 3 a 5: G1 (grado bajo o bien diferenciado)
- Puntuación total de 6 a 7: G2 (grado intermedio o moderadamente diferenciado)
- Puntuación total de 8 a 9: G3 (grado alto o poco diferenciado)
La prueba de biomarcadores se utiliza para determinar si las células del cáncer de mama tienen ciertos receptores.
Las células mamarias sanas y algunas células de cáncer de mama tienen receptores (biomarcadores) que se adhieren a las hormonas estrógeno y progesterona. Estas hormonas son necesarias para que las células sanas y algunas células de cáncer de mama crezcan y se dividan. Para verificar la presencia de estos biomarcadores, se extraen muestras de tejido que contienen células de cáncer de mama durante una biopsia o cirugía. Las muestras se analizan en un laboratorio para determinar si las células de cáncer de mama tienen receptores de estrógeno o progesterona.
Otro tipo de receptor (biomarcador) que se encuentra en la superficie de todas las células del cáncer de mama se llama HER2. Los receptores HER2 son necesarios para que las células del cáncer de mama crezcan y se dividan.
En el caso del cáncer de mama, las pruebas de biomarcadores incluyen lo siguiente:
- Receptor de estrógeno (ER): si las células del cáncer de mama tienen receptores de estrógeno, se las denomina ER positivas (ER+). Si no los tienen, se las denomina ER negativas (ER-).
- Receptor de progesterona (PR): si las células del cáncer de mama tienen receptores de progesterona, se las denomina PR positivas (PR+). Si no los tienen, se las denomina PR negativas (PR-).
- Receptor del factor de crecimiento epidérmico humano tipo 2 (HER2/neu o HER2): si las células del cáncer de mama tienen cantidades mayores de lo normal de receptores HER2 en su superficie, las células cancerosas se denominan HER2 positivas (HER2+). Si las células del cáncer de mama tienen una cantidad normal de HER2 en su superficie, las células cancerosas se denominan HER2 negativas (HER2-). El cáncer de mama HER2+ tiene más probabilidades de crecer y dividirse más rápido que el cáncer de mama HER2-.
A veces, las células de cáncer de mama se describen como triple negativas o triple positivas.
- Triple negativo: si las células del cáncer de mama no tienen receptores de estrógeno, receptores de progesterona o una cantidad mayor de lo normal de receptores HER2, se las denomina triple negativo.
- Triple positivo: si las células del cáncer de mama tienen receptores de estrógeno, receptores de progesterona y una cantidad mayor de lo normal de receptores HER2, se las denomina triple positivo.
Es importante conocer el estado de los receptores de estrógeno, progesterona y HER2 para elegir el mejor tratamiento. Existen medicamentos que pueden impedir que los receptores se adhieran a las hormonas estrógeno y progesterona y detener el crecimiento del cáncer. Se pueden utilizar otros medicamentos para bloquear los receptores HER2 en la superficie de las células del cáncer de mama y detener el crecimiento del cáncer.
El sistema TNM, el sistema de gradación y el estado de los biomarcadores se combinan para determinar el estadio del cáncer de mama.
A continuación se presentan tres ejemplos que combinan el sistema TNM, el sistema de gradación y el estado de los biomarcadores para determinar el estadio pronóstico patológico del cáncer de mama para una mujer cuyo primer tratamiento fue una cirugía:
Si el tamaño del tumor es de 30 milímetros (T2), no se ha diseminado a los ganglios linfáticos cercanos (N0), no se ha propagado a partes distantes del cuerpo (M0) y es:
- Grado 1
- HER2+
- ER-
- PR-
El cáncer está en estadio IIA.
Si el tamaño del tumor es de 53 milímetros (T3), se ha diseminado a entre cuatro y nueve ganglios linfáticos axilares (N2), no se ha diseminado a otras partes del cuerpo (M0) y es:
- Grado 2
- HER2+
- ER+
- PR-
El tumor está en estadio IIIA.
Si el tamaño del tumor es de 65 milímetros (T3), se ha diseminado a tres ganglios linfáticos axilares (N1a), se ha propagado a los pulmones (M1) y es:
- Grado 1
- HER2+
- ER-
- PR-
El cáncer está en estadio IV (cáncer de mama metastásico).
Hable con su médico para saber cuál es su estadio de cáncer de mama y cómo se utiliza para planificar el tratamiento más adecuado para usted.
Después de la cirugía, su médico recibirá un informe patológico que describe el tamaño y la ubicación del tumor primario, la propagación del cáncer a los ganglios linfáticos cercanos, el grado del tumor y la presencia de determinados biomarcadores. El informe patológico y los resultados de otras pruebas se utilizan para determinar el estadio del cáncer de mama.
Es probable que tenga muchas preguntas. Pídale a su médico que le explique cómo se utiliza la estadificación para decidir cuáles son las mejores opciones de tratamiento para su tipo de cáncer y si existen ensayos clínicos que podrían ser adecuados para usted.
El tratamiento del cáncer de mama en hombres depende en parte del estadio de la enfermedad.
Para conocer las opciones de tratamiento para el cáncer de mama en estadio I, II, IIIA y IIIC operable, consulte la sección Tratamiento del cáncer de mama temprano/localizado/operable en hombres.
Para conocer las opciones de tratamiento para el cáncer que ha recidivado (regresado) cerca del área donde se formó originalmente, consulte la sección Tratamiento del cáncer de mama recidivante locorregional en hombres.
Para conocer las opciones de tratamiento para el cáncer de mama en estadio IV (metastásico) o el cáncer de mama que ha recidivado en otras partes del cuerpo, consulte la sección Tratamiento del cáncer de mama metastásico en hombres.
Cáncer de mama inflamatorio en hombres
En el cáncer de mama inflamatorio, el cáncer se ha propagado a la piel de la mama y presenta enrojecimiento e hinchazón y se siente caliente al tacto. El enrojecimiento y el calor se producen porque las células cancerosas bloquean los vasos linfáticos de la piel. La piel de la mama también puede tener una apariencia con hoyuelos llamada peau d’orange (como la piel de una naranja). Es posible que no haya ningún bulto en la mama que se pueda palpar. El cáncer de mama inflamatorio puede estar en estadio IIIB, IIIC o IV.
Treatment Option Overview
Puntos clave
- Existen diferentes tipos de tratamiento para los hombres con cáncer de mama.
- Se utilizan cinco tipos de tratamiento estándar para tratar a los hombres con cáncer de mama:
- Cirugía
- Quimioterapia
- Terapia hormonal
- Radioterapia
- Terapia dirigida
- El tratamiento para el cáncer de mama en hombres puede provocar efectos secundarios.
Existen diferentes tipos de tratamiento para los hombres con cáncer de mama.
Existen distintos tipos de tratamiento disponibles para los hombres con cáncer de mama. Algunos de ellos son estándar (es decir, son los tratamientos que se utilizan actualmente) y otros se están probando en ensayos clínicos. Un ensayo clínico de tratamiento es un estudio de investigación cuyo objetivo es ayudar a mejorar los tratamientos actuales u obtener información sobre nuevos tratamientos para pacientes con cáncer. Cuando los ensayos clínicos muestran que un nuevo tratamiento es mejor que el que se utiliza actualmente, este puede convertirse en el tratamiento estándar.
Para algunos pacientes, participar en un ensayo clínico puede ser la mejor opción de tratamiento. Muchos de los tratamientos estándar para el cáncer que se utilizan en la actualidad se basan en ensayos clínicos anteriores. Los pacientes que participan en un ensayo clínico pueden recibir el tratamiento estándar o ser de los primeros en recibir un nuevo tratamiento.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Algunos ensayos clínicos solo incluyen pacientes que aún no han recibido tratamiento. Otros ensayos prueban tratamientos para pacientes cuyo cáncer no ha mejorado. También hay ensayos clínicos que prueban nuevas formas de evitar que el cáncer reaparezca (regrese) o reduzcan los efectos secundarios del tratamiento del cáncer.
Se están realizando ensayos clínicos en muchas partes del país. La información sobre los ensayos clínicos está disponible en el sitio web del NCI. Elegir el tratamiento más adecuado para el cáncer es una decisión que, idealmente, involucra al paciente, la familia y el equipo de atención médica.
Se utilizan cinco tipos de tratamiento estándar para tratar a los hombres con cáncer de mama:
Cirugía
La cirugía para los hombres con cáncer de mama suele ser una mastectomía radical modificada, que es una cirugía para extirpar toda la mama con cáncer. Esto puede incluir la extirpación del pezón, la areola (la piel de color oscuro alrededor del pezón) y la piel que cubre la mama. También se extirpan la mayoría de los ganglios linfáticos debajo del brazo.
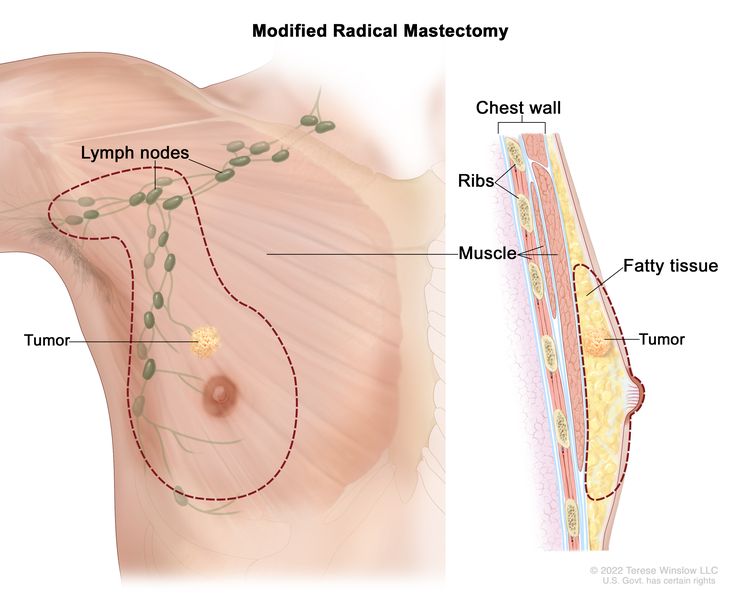
Mastectomía radical modificada: se extirpa toda la mama y la mayoría de los ganglios linfáticos debajo del brazo.
La cirugía conservadora de mama, una operación para extirpar el cáncer pero no la mama en sí, también se utiliza en algunos hombres con cáncer de mama. Se realiza una tumorectomía para extirpar el tumor (bulto) y una pequeña cantidad de tejido normal a su alrededor. Después de la cirugía se administra radioterapia para destruir cualquier célula cancerosa que haya quedado.
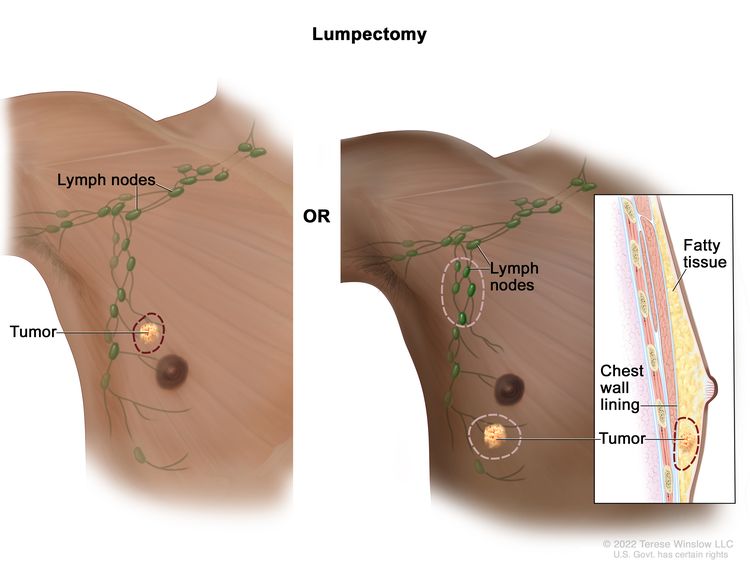
Lumpectomía. Se extirpa el tumor y parte del tejido sano circundante, pero no la mama en sí. También se pueden extirpar algunos ganglios linfáticos de la axila. Si el cáncer se encuentra cerca de la pared torácica, es posible que también se extirpe parte del revestimiento de la pared torácica.
Quimioterapia
La quimioterapia es un tratamiento contra el cáncer que utiliza medicamentos para detener el crecimiento de las células cancerosas, ya sea matándolas o impidiendo que se dividan. Cuando la quimioterapia se toma por vía oral o se inyecta en una vena o músculo, los medicamentos entran en el torrente sanguíneo y pueden llegar a las células cancerosas de todo el cuerpo (quimioterapia sistémica).
Consulte la página de Medicamentos aprobados para el cáncer de mama para obtener más información.
Terapia hormonal
La terapia hormonal es un tratamiento contra el cáncer que elimina hormonas o bloquea su acción, lo que detiene el crecimiento de las células cancerosas. Las hormonas son sustancias producidas por las glándulas del cuerpo y que circulan por el torrente sanguíneo. Algunas pueden favorecer el crecimiento de ciertos cánceres. Si las pruebas muestran que las células cancerosas tienen sitios donde las hormonas pueden adherirse (receptores), se pueden utilizar medicamentos, cirugía o radioterapia para reducir la producción hormonal o bloquear su funcionamiento.
La terapia hormonal con tamoxifeno suele administrarse a pacientes con cáncer de mama positivo para receptores de estrógeno y progesterona y a pacientes con cáncer de mama metastásico (cáncer que se ha propagado a otras partes del cuerpo).
A algunos hombres que tienen cáncer de mama metastásico se les administra terapia hormonal con un inhibidor de la aromatasa. Los inhibidores de la aromatasa disminuyen el estrógeno del cuerpo al bloquear una enzima llamada aromatasa que convierte el andrógeno en estrógeno. El anastrozol, el letrozol y el exemestano son tipos de inhibidores de la aromatasa.
A algunos hombres que tienen cáncer de mama metastásico se les administra terapia hormonal con un agonista de la hormona liberadora de hormona luteinizante (LHRH, por sus siglas en inglés). Estos agonistas actúan sobre la glándula pituitaria, que regula la cantidad de testosterona que producen los testículos. En los hombres que reciben esta terapia, la glándula pituitaria envía señales a los testículos para que produzcan menos testosterona. La leuprolida y la goserelina son tipos de agonistas de LHRH.
Otros tipos de terapia hormonal son el acetato de megestrol o la terapia antiestrógeno, como el fulvestrant.
Consulte la página de Medicamentos aprobados para el cáncer de mama para obtener más información.
Radioterapia
La radioterapia es un tratamiento contra el cáncer que utiliza rayos X de alta energía u otros tipos de radiación para matar las células cancerosas o evitar que crezcan. Para la radioterapia externa se usa una máquina que envía la radiación hacia la zona con cáncer desde el exterior del cuerpo.
Terapia dirigida
La terapia dirigida es un tipo de tratamiento que utiliza medicamentos u otras sustancias para identificar y atacar células cancerosas específicas. Las terapias dirigidas suelen causar menos daño a las células normales que la quimioterapia o la radioterapia. La terapia con anticuerpos monoclonales, los inhibidores de la tirosina quinasa, los inhibidores de las quinasas dependientes de ciclina y los inhibidores de la diana de rapamicina en mamíferos (mTOR, por sus siglas en inglés) son tipos de terapias dirigidas que se utilizan para tratar a los hombres con cáncer de mama.
Los anticuerpos monoclonales son proteínas del sistema inmunológico producidas en el laboratorio para tratar muchas enfermedades, incluido el cáncer. Como tratamiento contra el cáncer, estos anticuerpos pueden adherirse a un objetivo específico en las células cancerosas u otras células que podrían favorecer el crecimiento de las cancerosas. Luego, los anticuerpos pueden destruir las células cancerosas, bloquear su crecimiento o evitar que se propaguen. Los anticuerpos monoclonales se administran mediante infusión. Pueden usarse solos o para transportar medicamentos, toxinas o material radiactivo directamente a las células cancerosas.
Los tipos de terapia con anticuerpos monoclonales son:
- El trastuzumab es un anticuerpo monoclonal que bloquea los efectos de la proteína del factor de crecimiento HER2.
- El pertuzumab es un anticuerpo monoclonal que puede combinarse con el trastuzumab y la quimioterapia para tratar el cáncer de mama.
- El ado-trastuzumab emtansina es un anticuerpo monoclonal asociado a un medicamento contra el cáncer. Esto se denomina conjugado anticuerpo-fármaco. Puede utilizarse para tratar a los hombres con cáncer de mama positivo para receptores hormonales que se ha propagado a otras partes del cuerpo.
Los inhibidores de la tirosina quinasa son medicamentos de terapia dirigida que bloquean las señales necesarias para que los tumores crezcan. El lapatinib es un inhibidor de la tirosina quinasa que puede usarse para tratar a los hombres con cáncer de mama metastásico.
Los inhibidores de las quinasas dependientes de ciclina son medicamentos de terapia dirigida que bloquean proteínas llamadas quinasas dependientes de ciclina, responsables del crecimiento de las células cancerosas. El palbociclib es un inhibidor de este tipo que se utiliza para tratar a hombres con cáncer de mama metastásico.
Los inhibidores de la diana de la rapamicina en mamíferos (mTOR) bloquean una proteína llamada mTOR, que puede impedir el crecimiento de las células cancerosas y prevenir el crecimiento de nuevos vasos sanguíneos que necesitan los tumores para crecer.
Consulte la página de Medicamentos aprobados para el cáncer de mama para obtener más información.
El tratamiento para el cáncer de mama en hombres puede provocar efectos secundarios.
For information about side effects caused by treatment for cancer, visit our Side Effects page.
Tratamiento del cáncer de mama en hombres en estadio temprano, localizado y operable
For information about the treatments listed below, see the Treatment Option Overview section.
El tratamiento del cáncer de mama temprano, localizado u operable puede incluir lo siguiente:
Cirugía inicial
El tratamiento para los hombres diagnosticados con cáncer de mama suele ser una mastectomía radical modificada.
En algunos hombres se puede realizar la cirugía conservadora de la mama con lumpectomía seguida de radioterapia.
Terapia adyuvante
La terapia que se administra después de una operación, cuando ya no se observan las células cancerosas, se llama terapia adyuvante. Incluso si el médico extirpa todo el cáncer visible al momento de la operación, es posible que el paciente reciba radioterapia, quimioterapia, terapia hormonal y/o terapia dirigida después de la cirugía, para intentar destruir cualquier célula cancerosa que pueda haber quedado.
- Sin afectación ganglionar: en el caso de los hombres cuyo cáncer no presenta afectación ganglionar (el cáncer no se ha propagado a los ganglios linfáticos), la terapia adyuvante se debe considerar de la misma manera que para una mujer con cáncer de mama porque no hay evidencia de que la respuesta al tratamiento sea diferente entre hombres y mujeres.
- Con afectación ganglionar: en el caso de los hombres cuyo cáncer presenta afectación ganglionar (el cáncer se diseminó a los ganglios linfáticos), la terapia adyuvante puede incluir lo siguiente:
- Chemotherapy.
- Terapia hormonal con tamoxifeno (para bloquear el efecto del estrógeno) o, con menos frecuencia, inhibidores de la aromatasa (para reducir la cantidad de estrógeno en el cuerpo).
- Terapia dirigida con un anticuerpo monoclonal (trastuzumab o pertuzumab)
Estos tratamientos parecen aumentar la supervivencia en hombres, al igual que en mujeres. La respuesta del paciente a la terapia hormonal depende de la presencia de receptores hormonales ( proteínas ) en el tumor . La mayoría de los cánceres de mama en hombres presentan estos receptores. La terapia hormonal suele recomendarse para pacientes masculinos con cáncer de mama, pero puede tener muchos efectos secundarios, como sofocos e impotencia (la incapacidad de lograr una erección suficiente para la relación sexual).
Tratamiento del cáncer de mama recidivante locorregional en hombres
For information about the treatments listed below, see the Treatment Option Overview section.
Para los hombres con enfermedad recidivante local (cáncer que ha regresado en un área limitada después del tratamiento), las opciones de tratamiento son:
- Cirugía.
- Radioterapia en combinación con quimioterapia
Tratamiento del cáncer de mama metastásico en hombres
For information about the treatments listed below, see the Treatment Option Overview section.
Las opciones de tratamiento para el cáncer de mama metastásico (cáncer que se ha propagado a partes distantes del cuerpo) pueden ser las siguientes:
Terapia hormonal
En los hombres a quienes se les acaba de diagnosticar cáncer de mama metastásico positivo para receptores hormonales o cuyo estado de receptores hormonales es desconocido, el tratamiento puede incluir:
- Tamoxifeno terapia.
- Terapia con inhibidores de la aromatasa (anastrozol, letrozol o exemestano) con o sin un agonista de LHRH. A veces también se administra terapia con inhibidores de las quinasas dependientes de ciclinas (palbociclib).
En hombres cuyos tumores tienen receptores hormonales positivos o receptores hormonales desconocidos, con diseminación solo al hueso o tejido blando y que han sido tratados con tamoxifeno, el tratamiento puede incluir:
- Terapia con inhibidores de la aromatasa con o sin agonista LHRH.
- Otra terapia hormonal como acetato de megestrol, terapia con estrógenos o andrógenos, o terapia antiestrógeno como fulvestrant
Terapia dirigida
En los hombres con cáncer de mama metastásico positivos para receptores hormonales que no ha respondido a otros tratamientos, las opciones pueden consistir en terapia dirigida, como:
- Trastuzumab, lapatinib, pertuzumab o inhibidores de mTOR
- Terapia conjugada anticuerpo-fármaco con ado-trastuzumab emtansina
- Tratamiento con inhibidores de las quinasas dependientes de ciclinas (palbociclib) combinado con letrozol
En los hombres con cáncer de mama metastásico positivo para HER2/neu, el tratamiento puede consistir en:
- Terapia dirigida como trastuzumab, pertuzumab, ado-trastuzumab emtansine o lapatinib
Quimioterapia
En los hombres con cáncer de mama metastásico negativo para receptores hormonales, que no ha respondido a la terapia hormonal, que se ha propagado a otros órganos o que ha producido síntomas, el tratamiento puede incluir:
- Quimioterapia con uno o más medicamentos
Cirugía
- Mastectomía total para hombres con lesiones mamarias abiertas o dolorosas. Se puede administrar radioterapia después de la cirugía.
- Cirugía para extirpar el cáncer que se ha diseminado al cerebro o la columna vertebral. Se puede administrar radioterapia después de la cirugía.
- Cirugía para extirpar el cáncer que se ha diseminado al pulmón.
- Cirugía para reparar o reforzar huesos débiles o fracturados. La radioterapia se puede administrar después de la cirugía.
- Cirugía para eliminar el líquido que se ha acumulado alrededor de los pulmones o el corazón.
Radioterapia
- Radioterapia dirigida a los huesos, el cerebro, la médula espinal, la mama o la pared torácica para aliviar los síntomas y mejorar la calidad de vida.
- Estroncio-89 (un radionúclido) para aliviar el dolor producido por el cáncer que se ha diseminado a los huesos de todo el cuerpo.
Otras opciones de tratamiento
Otras opciones de tratamiento para el cáncer de mama metastásico pueden ser:
- Tratamiento con medicamentos, como bifosfonatos o denosumab, para reducir la enfermedad ósea y el dolor cuando el cáncer se ha propagado a los huesos. (Consulte el resumen del PDQ sobre el Dolor por cáncer para obtener más información sobre los bifosfonatos).
- Ensayos clínicos que evalúan nuevos medicamentos contra el cáncer, nuevas combinaciones de medicamentos y nuevas formas de administrar tratamientos.
Más información sobre el cáncer de mama en hombres
Para obtener más información del National Cancer Institute sobre el cáncer de mama en hombres, consulte las siguientes páginas:
- Página de inicio sobre el cáncer de mama
- Medicamentos aprobados para el cáncer de mama
- Terapia hormonal para el cáncer de mama
- Terapias dirigidas contra el cáncer
- Pruebas genéticas para síndromes hereditarios de susceptibilidad al cáncer
- Alteraciones en el gen BRCA: riesgo de cáncer y pruebas genéticas
For general cancer information and other resources from the National Cancer Institute, visit:
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen del PDQ sobre el cáncer contiene información actualizada del tratamiento del cáncer de mama masculino. El propósito es informar y ayudar a los pacientes, sus familiares y cuidadores. No da pautas ni recomendaciones formales para tomar decisiones relacionadas con la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre el tratamiento de adultos. Tratamiento del cáncer de mama en hombres (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Actualizado:
URL de origen: https://www.cancer.gov/node/4393/syndication
Agencia de origen: National Cancer Institute (NCI)
Fecha de captura: 2013-09-14 09:02:11.0