








Tratamiento de la enfermedad trofoblástica gestacional
Obtenga una atención excepcional para la enfermedad trofoblástica gestacional y el cáncer ginecológico en el Montefiore Einstein Comprehensive Cancer Center. Nuestro equipo multidisciplinario tiene una amplia experiencia en el tratamiento de este tipo de cáncer. Como uno de los primeros centros del cáncer designados por el NCI, llevamos más de 50 años liderando en la investigación, el diagnóstico y el tratamiento de más de 200 tipos de cáncer.
Estamos a la vanguardia en el tratamiento y la investigación de la enfermedad trofoblástica gestacional y los cánceres ginecológicos. Ofrecemos planes de tratamiento integrales, individualizados según las necesidades de nuestros pacientes. En el Montefiore Einstein Comprehensive Cancer Center, damos acceso a atención médica innovadora y de vanguardia, basada en las últimas investigaciones, y la oportunidad de participar en ensayos clínicos.
Cuando necesite atención para la enfermedad trofoblástica gestacional, acuda a nuestros proveedores, a quienes les apasiona acabar con el cáncer y abordar todas sus necesidades de salud.

El Montefiore Einstein Comprehensive Cancer Center, designado como centro integral del cáncer por el National Cancer Institute (NCI), apoya la misión y las normas del NCI. La siguiente información sobre los tipos de cáncer, prevención y tratamientos ha sido facilitada por el NCI.
Tratamiento de la enfermedad trofoblástica gestacional (PDQ®): versión para pacientes
Información general sobre la enfermedad trofoblástica gestacional
Puntos clave
- La enfermedad trofoblástica gestacional (ETG) es un grupo de enfermedades raras en las que crecen células trofoblásticas anómalas dentro del útero después de la concepción.
- La mola hidatiforme (MH) es el tipo más común de ETG.
- La neoplasia trofoblástica gestacional (NTG) es un tipo de enfermedad trofoblástica gestacional (ETG) que casi siempre es maligna.
- Molas invasivas
- Coriocarcinomas
- Tumores trofoblásticos del sitio placentario
- Tumores trofoblásticos epitelioides
- La edad y un embarazo molar previo aumentan el riesgo de desarrollar ETG.
- Los signos de la ETG son sangrado vaginal anómalo y un útero más grande de lo normal.
- Las pruebas que examinan el útero se utilizan para detectar (encontrar) y diagnosticar la enfermedad trofoblástica gestacional.
- Certain factors affect prognosis (chance of recovery) and treatment options.
La enfermedad trofoblástica gestacional (ETG) es un grupo de enfermedades raras en las que crecen células trofoblásticas anómalas dentro del útero después de la concepción.
En la enfermedad trofoblástica gestacional (ETG), se desarrolla un tumor dentro del útero a partir del tejido que se forma después de la concepción (la unión del espermatozoide y el óvulo). Este tejido está formado por células trofoblásticas y normalmente rodea el óvulo fecundado en el útero. Estas células ayudan a conectar el óvulo fecundado a la pared del útero y forman parte de la placenta (el órgano que transfiere los nutrientes de la madre al feto).
A veces, el óvulo fecundado y las células del trofoblasto no se desarrollan correctamente. En lugar de un feto sano, se forma un tumor. Mientras no se manifiesten signos o síntomas del tumor, el embarazo parecerá normal.
La mayoría de las ETG son benignas (no cancerosas) y no se propagan, pero algunos tipos se vuelven malignos (cancerosos) y se diseminan a tejidos cercanos o partes distantes del cuerpo.
La enfermedad trofoblástica gestacional (ETG) es un término general que comprende diferentes tipos de enfermedades:
- Molas hidatiformes (MH)
- Completar HM.
- MH parcial
- Trofoblástico gestacional Neoplasia (NTG)
- Molas invasivas.
- Coriocarcinomas.
- Tumores trofoblásticos del sitio placentario (PSTT; son muy raros).
- Tumores trofoblásticos epitelioides (TTE; estos son aún más raros).
La mola hidatiforme (MH) es el tipo más común de ETG.
Las MH son tumores de crecimiento lento que parecen sacos de líquido. También se lo denomina embarazo molar. Se desconoce la causa de las molas hidatidiformes.
Las MH pueden ser completas o parciales:
- Una MH completa se forma cuando el espermatozoide fecunda un óvulo que no contiene el ADN de la madre. El óvulo tiene ADN del padre y las células que debían convertirse en la placenta son anómalas.
- Una MH parcial se forma cuando un espermatozoide fecunda un óvulo normal y existen dos conjuntos de ADN del padre en el óvulo fecundado. Solo se forma una parte del feto y las células que debían formar la placenta son anómalas.
La mayoría de las molas hidatidiformes son benignas, pero a veces se convierten en cáncer. Tener uno o más de los siguientes factores de riesgo aumenta la probabilidad de que una mola hidatidiforme se convierta en cáncer:
- Tener un embarazo antes de los 20 o después de los 35 años de edad.
- Un nivel muy alto de gonadotropina coriónica humana beta (beta-hCG, por sus siglas en inglés), una hormona producida por el cuerpo durante el embarazo.
- Un tumor grande en el útero.
- Un quiste ovárico de más de 6 centímetros
- Presión arterial alta durante el embarazo.
- Una glándula tiroides hiperactiva (se produce más hormona tiroidea).
- Náuseas y vómitos intensos durante el embarazo
- Células trofoblásticas en la sangre, que pueden bloquear los vasos sanguíneos pequeños.
- Problemas graves de coagulación sanguínea causados por la MH.
La neoplasia trofoblástica gestacional (NTG) es un tipo de enfermedad trofoblástica gestacional (ETG) que casi siempre es maligna.
La neoplasia trofoblástica gestacional (NTG) comprende las siguientes afecciones:
Molas invasivas
Las molas invasivas se componen de células trofoblásticas que crecen en la capa muscular del útero. Tienen mayor probabilidad de crecer y propagarse que las molas hidatiformes. En raras ocasiones, una mola hidatiforme completa o parcial puede convertirse en una mola invasiva. En ocasiones, una mola invasiva desaparece sin tratamiento.
Coriocarcinomas
Un coriocarcinoma es un tumor maligno que se forma a partir de células trofoblásticas y se disemina a la capa muscular del útero y a los vasos sanguíneos cercanos. También puede propagarse a otras partes del cuerpo, como el cerebro, los pulmones, el hígado, los riñones, el bazo, los intestinos, la pelvis o la vagina. Es más probable que se forme un coriocarcinoma en mujeres que han tenido alguno de los siguientes síntomas:
- Embarazo molar, especialmente con mola hidatidiforme completa.
- Embarazo normal.
- Embarazo tubárico (el óvulo fecundado se implanta en las trompas de Falopio en lugar del útero).
- Aborto espontáneo.
Tumores trofoblásticos del sitio placentario
Un tumor trofoblástico del sitio placentario (TTSP) es un tipo poco común de neoplasia trofoblástica gestacional que se forma donde la placenta se une al útero. El tumor se forma a partir de células trofoblásticas y se propaga al músculo del útero y a los vasos sanguíneos. También puede diseminarse a los pulmones, la pelvis o los ganglios linfáticos. Un TTSP crece muy lentamente y los signos o síntomas pueden aparecer meses o años después de un embarazo normal.
Tumores trofoblásticos epitelioides
Un tumor trofoblástico epitelioide (TTE) es un tipo muy poco común de neoplasia trofoblástica gestacional que puede ser benigna o maligna. Cuando el tumor es maligno, puede extenderse a los pulmones.
La edad y un embarazo molar previo aumentan el riesgo de desarrollar ETG.
Cualquier factor de riesgo que aumente el riesgo de desarrollar una enfermedad se denomina factor de riesgo. Tener un factor de riesgo no significa que tendrá cáncer, a la vez que no tener ningún factor de riesgo tampoco significa que no vaya a desarrollarlo. Consulte con su médico si cree que podría estar en riesgo. Los factores de riesgo para la ETG son los siguientes:
- Estar embarazada antes de los 20 años o después de los 35
- Tener un historial personal de mola hidatidiforme.
Los signos de la ETG son sangrado vaginal anómalo y un útero más grande de lo normal.
Estos y otros signos y síntomas pueden estar causados por la enfermedad trofoblástica gestacional o por otras afecciones. Consulte con su médico si presenta alguno de los siguientes síntomas:
- Sangrado vaginal no relacionado con la menstruación.
- Un útero más grande de lo esperado durante el embarazo.
- Dolor o presión en la pelvis.
- Náuseas y vómitos intensos durante el embarazo.
- Presión arterial alta con dolor de cabeza e hinchazón de pies y manos al principio del embarazo.
- Sangrado vaginal que continúa durante más tiempo de lo normal después del parto.
- Fatiga, dificultad para respirar, mareos y latidos cardiacos rápidos o irregulares causados por la anemia
La ETG a veces causa hipertiroidismo. Los signos y síntomas del hipertiroidismo son los siguientes:
- Latidos cardiacos rápidos o irregulares.
- Inestabilidad
- Transpiración
- Deposiciones frecuentes
- Problemas para dormir
- Sentirse ansioso o irritable.
- Pérdida de peso
Las pruebas que examinan el útero se utilizan para detectar (encontrar) y diagnosticar la enfermedad trofoblástica gestacional.
Se pueden utilizar las siguientes pruebas y procedimientos:
- Reconocimiento físico e historial de salud: se hace un reconocimiento del cuerpo para verificar signos generales de salud, incluida la detección de signos de enfermedad, como bultos o cualquier otra anomalía. También se registrará el historial de los hábitos de salud del paciente, así como de enfermedades y tratamientos pasados.
- Examen pélvico: un examen de la vagina, cuello uterino, útero, trompas de Falopio, ovarios, and recto. Un espéculo se introduce en la vagina y el médico o enfermero examina la vagina y el cuello uterino en busca de signos de enfermedad. Un Prueba de Papanicolaou del cuello uterino por lo general se hace. El médico o enfermero también inserta uno o dos lubricados, dedos enguantados de una mano en la vagina y coloca la otra mano sobre la parte inferior del abdomen para palpar el tamaño, la forma y la posición del útero y los ovarios. El médico o enfermero también inserta un dedo enguantado y lubricado en el recto para palpar bultos o áreas anormales.
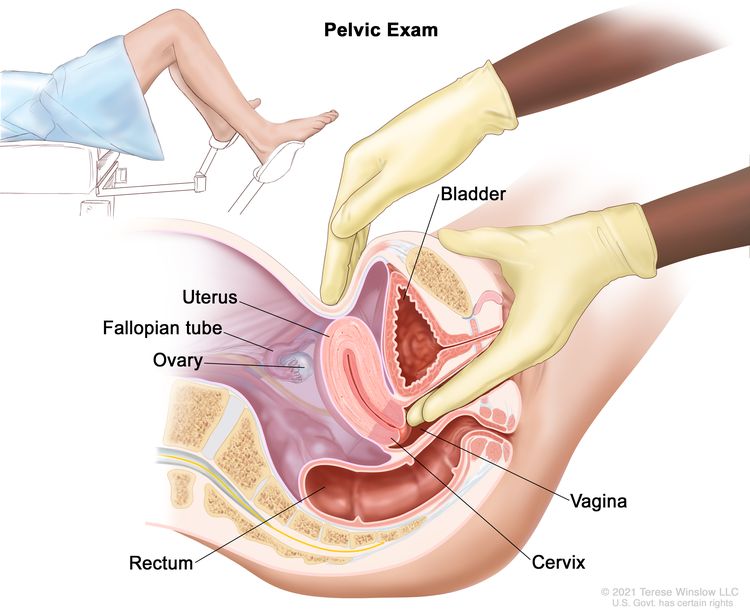
Examen pélvico. Un médico o enfermero introduce uno o dos dedos de una mano, con guantes y lubricados, en la vagina, mientras presiona la parte inferior del abdomen con la otra mano. Esto se hace para palpar el tamaño, la forma y la posición del útero y los ovarios. También se examinan la vagina, el cuello uterino, las trompas de Falopio y el recto.
- Ecografía pélvica: Procedimiento en el que ondas sonoras de alta energía (ultrasonido) rebotan en los tejidos u órganos internos de la pelvis y producen ecos. Estos ecos forman una imagen de los tejidos corporales llamada ecografía . En ocasiones, se realiza una ecografía transvaginal (ETV). Para la ETV, se introduce un transductor de ultrasonido (sonda) en la vagina para obtener la imagen ecográfica.
- Estudios de química sanguínea: es un procedimiento en el que se analiza una muestra de sangre para medir las cantidades de ciertas sustancias liberadas a la sangre por los órganos y tejidos del cuerpo. Una cantidad inusual (mayor o menor de lo normal) de una sustancia puede ser un signo de enfermedad. También se analiza la sangre para controlar el hígado, los riñones y la médula ósea.
- Prueba de marcadores tumorales séricos: es un procedimiento en el que se analiza una muestra de sangre para medir las cantidades de ciertas sustancias producidas por órganos, tejidos o células tumorales en el cuerpo. Ciertas sustancias están relacionadas con tipos específicos de cáncer cuando se encuentran en niveles elevados en el cuerpo. Estos se llaman marcadores tumorales. Para la ETG, se analiza la sangre para determinar el nivel de gonadotropina coriónica humana beta (beta-hCG), una hormona que produce el cuerpo durante el embarazo. La beta-hCG en la sangre de una mujer que no está embarazada puede ser un signo de ETG.
- Análisis de orina: es una prueba para verificar el color de la orina y su contenido, como azúcar, proteínas, sangre, bacterias y el nivel de beta-hCG.
Certain factors affect prognosis (chance of recovery) and treatment options.
La enfermedad trofoblástica gestacional generalmente se puede curar. El tratamiento y el pronóstico dependen de lo siguiente:
- El tipo de ETG
- Si el tumor se ha diseminado al útero, a los ganglios linfáticos o a partes distantes del cuerpo.
- La cantidad de tumores y su ubicación en el cuerpo.
- El tamaño del tumor más grande.
- El nivel de beta-hCG en la sangre.
- Qué tan pronto se diagnosticó el tumor después de que comenzó el embarazo.
- Si la ETG se desarrolló después de un embarazo molar, un aborto espontáneo o un embarazo normal.
- Tratamiento previo de la neoplasia trofoblástica gestacional.
Las opciones de tratamiento también dependen de si la mujer desea quedarse embarazada en el futuro.
Estadios de los tumores y las neoplasias trofoblásticas gestacionales
Puntos clave
- Una vez diagnosticada la neoplasia trofoblástica gestacional, se realizan pruebas para determinar si el cáncer se ha propagado desde donde comenzó a otras partes del cuerpo.
- There are three ways that cancer spreads in the body.
- El cáncer puede extenderse desde donde comenzó a otras partes del cuerpo.
- No existe un sistema de estadificación para las molas hidatiformes.
- Se utilizan los siguientes estadios para describir la neoplasia trofoblástica gestacional:
- Estadio I
- Estadio II
- Estadio III
- Estadio IV
- El tratamiento de la neoplasia trofoblástica gestacional se basa en el tipo de enfermedad, estadio o grupo de riesgo.
Una vez diagnosticada la neoplasia trofoblástica gestacional, se realizan pruebas para determinar si el cáncer se ha propagado desde donde comenzó a otras partes del cuerpo.
El proceso utilizado para determinar la extensión o propagación del cáncer se denomina estadificación . La información obtenida mediante estadificación ayuda a determinar el estadio de la enfermedad. En el caso de la neoplasia trofoblástica gestacional (NTG), el estadio es uno de los factores que se utilizan para planificar el tratamiento.
Se pueden realizar las siguientes pruebas y procedimientos para ayudar a determinar el estadio de la enfermedad:
- Radiografía de tórax: Radiografía de los órganos y huesos del interior del tórax. Un rayo X es un tipo de haz de energía que atraviesa el cuerpo y se graba en una película, generando imágenes de áreas internas.
- tomografía computarizada (TC): Procedimiento que genera una serie de imágenes detalladas del interior del cuerpo, tomadas desde diferentes ángulos. Las imágenes se crean mediante una computadora conectada a una máquina de rayos X. Se puede inyectar o ingerir un medio de contraste para que los órganos y tejidos se visualicen con mayor claridad. Este procedimiento también se denomina tomografía axial computarizada (TAC) o escáner axial computarizado.).
- Resonancia magnética ( resonancia magnética ) con gadolinio: Procedimiento que utiliza un imán, ondas de radio y una computadora para generar una serie de imágenes detalladas de áreas del interior del cuerpo, como el cerebro y la médula espinal . Se inyecta una sustancia llamada gadolinio en una vena. El gadolinio se acumula alrededor de las células cancerosas, haciéndolas más brillantes en la imagen. Este procedimiento también se denomina resonancia magnética nuclear (RMN).
- Punción lumbar: Procedimiento para extraer líquido cefalorraquídeo (LCR) de la columna vertebral . Se realiza insertando una aguja entre dos huesos de la columna vertebral y penetrando el LCR que rodea la médula espinal, extrayendo una muestra del líquido. Esta muestra de LCR se examina al microscopio para detectar signos de propagación del cáncer al cerebro y la médula espinal. Este procedimiento también se denomina PL o punción lumbar.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
El cáncer puede extenderse desde donde comenzó a otras partes del cuerpo.
Cuando el cáncer se extiende a otra parte del cuerpo se denomina metástasis. Las células cancerosas se desprenden de donde comenzaron (tumor primario) y viajan a través del sistema linfático o la sangre.
- Sistema linfático: el cáncer entra en el sistema linfático, viaja a través de los vasos linfáticos y forma un tumor (tumor metastásico) en otra parte del cuerpo.
- Sangre: el cáncer llega a la sangre, viaja a través de los vasos sanguíneos y forma un tumor (tumor metastásico) en otra parte del cuerpo.
El tumor metastásico es el mismo tipo de cáncer que el tumor primario. Por ejemplo, si el coriocarcinoma se propaga al pulmón, las células cancerosas pulmonares son en realidad células de coriocarcinoma. La enfermedad es coriocarcinoma metastásico, no cáncer de pulmón.
No existe un sistema de estadificación para las molas hidatiformes.
Las molas hidatiformes (MH) se encuentran únicamente en el útero y no se propagan a otras partes del cuerpo.
Se utilizan los siguientes estadios para describir la neoplasia trofoblástica gestacional:
Estadio I
En el estadio I, el tumor está sólo en el útero .
Estadio II
En el estadio II, el tumor se ha propagado más allá del útero hasta el ovario, la trompa de Falopio, la vagina y/o los tejidos conectivos alrededor del útero.
Estadio III
En el estadio III, el tumor se ha diseminado al pulmón, con o sin diseminación al ovario, las trompas de Falopio, la vagina y/o los tejidos conectivos alrededor del útero .
Estadio IV
En el estadio IV, el tumor se ha diseminado a partes distantes del cuerpo distintas de los pulmones .
El tratamiento de la neoplasia trofoblástica gestacional se basa en el tipo de enfermedad, estadio o grupo de riesgo.
Las molas invasivas y los coriocarcinomas se tratan según los grupos de riesgo . El estadio de la mola invasiva o el coriocarcinoma es un factor que se utiliza para determinar el grupo de riesgo. Otros factores incluyen los siguientes:
- La edad del paciente cuando se realiza el diagnóstico .
- Si el GTN se produjo después de un embarazo molar, un aborto espontáneo o un embarazo normal.
- Qué tan pronto se diagnosticó el tumor después de que comenzó el embarazo.
- El nivel de gonadotropina coriónica humana beta (beta-hCG) en la sangre.
- El tamaño del tumor más grande.
- Dónde se ha diseminado el tumor y la cantidad de tumores en el cuerpo.
- Con cuántos medicamentos de quimioterapia se ha tratado el tumor (para tumores recurrentes o resistentes).
Existen dos grupos de riesgo para molas invasivas y coriocarcinomas: bajo riesgo y alto riesgo. Los pacientes con enfermedad de bajo riesgo suelen recibir un tratamiento menos agresivo que los pacientes con enfermedad de alto riesgo.
Los tratamientos del tumor trofoblástico del sitio placentario (TTSP) y del tumor trofoblástico epitelioide (TTE) dependen del estadio de la enfermedad.
Neoplasia trofoblástica gestacional recidivante y resistente
La neoplasia trofoblástica gestacional recurrente (NTG) es un cáncer que ha reaparecido (regresado) después de haber sido tratado. El cáncer puede reaparecer en el útero o en otras partes del cuerpo.
La neoplasia trofoblástica gestacional que no responde al tratamiento se denomina GTN resistente.
Treatment Option Overview
Puntos clave
- Existen diferentes tipos de tratamiento para las pacientes con enfermedad trofoblástica gestacional.
- Se utilizan tres tipos de tratamiento estándar:
- Cirugía
- Quimioterapia
- Radioterapia
- New types of treatment are being tested in clinical trials.
- El tratamiento de la enfermedad trofoblástica gestacional puede producir efectos secundarios.
- Patients may want to think about taking part in a clinical trial.
- Patients can enter clinical trials before, during, or after starting their cancer treatment.
- Pueden ser necesarias pruebas de seguimiento.
Existen diferentes tipos de tratamiento para las pacientes con enfermedad trofoblástica gestacional.
Existen diferentes tipos de tratamiento disponibles para pacientes con enfermedad trofoblástica gestacional . Algunos tratamientos son estándar (el tratamiento utilizado actualmente) y otros se están probando en ensayos clínicos . Antes de comenzar el tratamiento, es posible que los pacientes consideren participar en un ensayo clínico. Un ensayo clínico de tratamiento es un estudio de investigación cuyo objetivo es mejorar los tratamientos actuales u obtener información sobre nuevos tratamientos para pacientes con cáncer . Cuando los ensayos clínicos demuestran que un nuevo tratamiento es mejor que el tratamiento estándar, este puede convertirse en el tratamiento estándar.
Se están realizando ensayos clínicos en muchas partes del país. Puede encontrar información sobre los ensayos clínicos en curso en el sitio web del NCI . Elegir el tratamiento oncológico más adecuado es una decisión que, idealmente, involucra al paciente, su familia y el equipo de atención médica.
Se utilizan tres tipos de tratamiento estándar:
Cirugía
El médico puede extirpar el cáncer realizando alguna de las siguientes cirugías:
- Dilatación y curetaje (D y C) con evacuación por succión: un quirúrgico procedimiento para eliminar anómalas tejidos y partes del revestimiento interior de la útero. El cuello uterino es dilatado y el material del interior del útero se extrae con un pequeño aspirador. dispositivoLuego se raspan suavemente las paredes del útero con una cureta (instrumento con forma de cuchara) para extraer cualquier material que pueda quedar en el útero. Este procedimiento puede llevarse a cabo en embarazos molares.
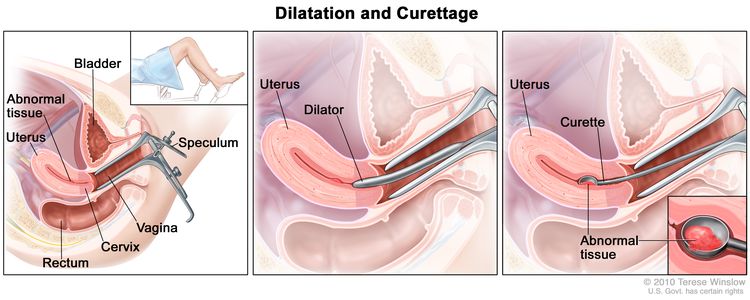
Dilatación y curetaje (D y C). Se inserta un espéculo en la vagina para ensancharla y observar el cuello uterino (primer gráfico). Se utiliza un dilatador para ensanchar el cuello uterino (gráfico del medio). Se coloca una cureta a través del cuello uterino hasta el útero para raspar el tejido anómalo (último gráfico).
- Histerectomía: Cirugía para extirpar el útero y, a veces, el cuello uterino. Si el útero y el cuello uterino se extraen a través de la vagina, la operación se llama histerectomía vaginal. Si se extirpan el útero y el cuello uterino a través de una gran incisión (corte) en el abdomen, la operación se denomina histerectomía abdominal total. Si se extirpan el útero y el cuello uterino a través de una pequeña incisión (corte) en el abdomen utilizando un laparoscopio, la operación se llama histerectomía laparoscópica total.
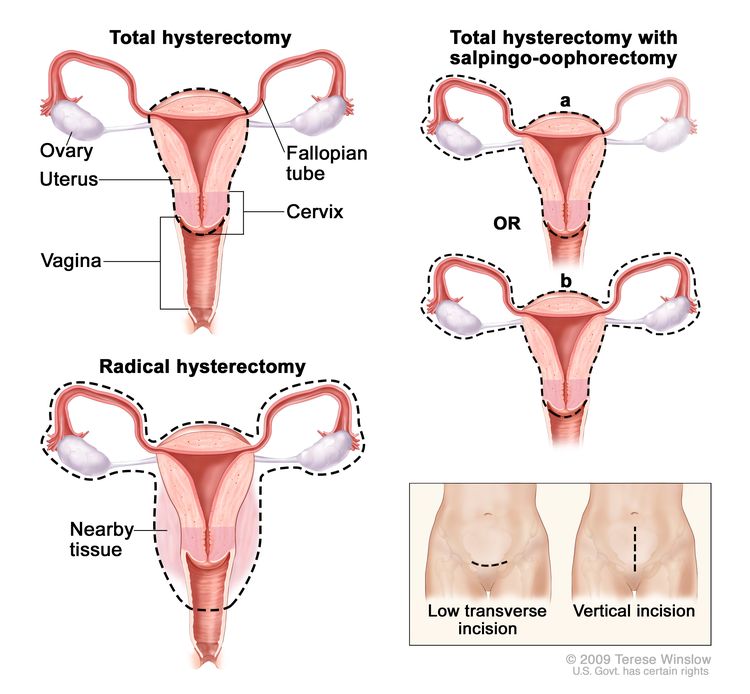
Histerectomía. El útero se extirpa quirúrgicamente con o sin otros órganos o tejidos. En una histerectomía total, se extirpan el útero y el cuello uterino. En una histerectomía total con salpingooforectomía, (a) se extirpan el útero, un ovario y una trompa de Falopio (unilaterales) o (b) se extirpan el útero, ambos ovarios y trompas de Falopio (bilaterales). En una histerectomía radical, se extirpan el útero, el cuello uterino, ambos ovarios, ambas trompas de Falopio y el tejido circundante. Estos procedimientos se realizan mediante una incisión transversal baja o una incisión vertical.
Después de que el doctor extirpe todo el cáncer visible en el momento de la cirugía, algunos pacientes podrían recibir quimioterapia para eliminar cualquier célula cancerosa restante. El tratamiento que se administra después de la cirugía para reducir el riesgo de reaparición del cáncer se denomina terapia adyuvante .
Quimioterapia
La quimioterapia es un tratamiento contra el cáncer que utiliza medicamentos para detener el crecimiento de las células cancerosas, ya sea destruyéndolas o impidiendo que se dividan. Cuando la quimioterapia se administra por vía oral o se inyecta en una vena o músculo, los medicamentos ingresan al torrente sanguíneo y pueden alcanzar las células cancerosas de todo el cuerpo ( quimioterapia sistémica ). Cuando la quimioterapia se administra directamente en el líquido cefalorraquídeo, un órgano o una cavidad corporal como el abdomen, los medicamentos afectan principalmente a las células cancerosas en esas áreas ( quimioterapia regional ). La forma en que se administra la quimioterapia depende del tipo y el estadio del cáncer que se esté tratando, o de si el tumor es de bajo o alto riesgo.
La quimioterapia combinada es un tratamiento que utiliza más de un medicina contra el cáncer.
Consulte Medicamentos aprobados para la enfermedad trofoblástica gestacional para obtener más información.
Radioterapia
La radioterapia es un tratamiento para el cáncer que utiliza rayos X de alta energía u otros tipos de radiación para destruir las células cancerosas o impedir su crecimiento. Existen dos tipos de radioterapia:
- La radioterapia externa utiliza una máquina fuera del cuerpo para enviar radiación hacia el cáncer.
- La radioterapia interna utiliza una sustancia radiactiva sellada en agujas, semillas, cables o catéteres que se colocan directamente en el cáncer o cerca de él.
La forma de administrar la radioterapia depende del tipo de enfermedad trofoblástica gestacional que se esté tratando. La radioterapia externa se utiliza para la enfermedad trofoblástica gestacional.
New types of treatment are being tested in clinical trials.
La información sobre los ensayos clínicos en curso está disponible en el sitio web del NCI .
El tratamiento de la enfermedad trofoblástica gestacional puede producir efectos secundarios.
Para obtener información sobre los efectos secundarios causados por el tratamiento para el cáncer, visite la página de efectos secundarios.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI’s clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Pueden ser necesarias pruebas de seguimiento.
A medida que avanza el tratamiento, se le realizarán pruebas o controles de seguimiento. Es posible que se repitan algunas pruebas para diagnosticar o estadificar el cáncer con el fin de evaluar cómo está funcionando el tratamiento. Las decisiones sobre si continuar, modificar o suspender el tratamiento pueden basarse en los resultados de estas pruebas.
Algunas pruebas seguirán realizándose de manera periódica después de terminar el tratamiento. Los resultados pueden indicar si su afección ha cambiado o si el cáncer ha redicivado (regresado).
Los niveles sanguíneos de gonadotropina coriónica humana beta (beta-hCG) se controlarán hasta 6 meses después de finalizar el tratamiento. Esto se debe a que un nivel de beta-hCG superior al normal puede indicar que el tumor no ha respondido al tratamiento o se ha convertido en cáncer.
Opciones de tratamiento para la enfermedad trofoblástica gestacional
For information about the treatments listed below, see the Treatment Option Overview section.
Molas hidatiformes
El tratamiento de una mola hidatiforme puede incluir lo siguiente:
- Cirugía ( dilatación y curetaje con evacuación por succión ) para extirpar el tumor .
Después de la cirugía, se realizan análisis de sangre de gonadotropina coriónica humana beta (beta-hCG) semanalmente hasta que el nivel de beta-hCG se normalice. Las pacientes también tienen visitas doctor de seguimiento mensuales durante un máximo de 6 meses. Si el nivel de beta-hCG no se normaliza o aumenta, podría significar que la mola hidatiforme no se extirpó por completo y se ha convertido en cáncer . El embarazo provoca un aumento en los niveles de beta-hCG, por lo que su doctor le pedirá que no se embarace hasta que finalice el seguimiento.
Para la enfermedad que persiste después de la cirugía, el tratamiento generalmente es quimioterapia .
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Neoplasia trofoblástica gestacional
Neoplasia trofoblástica gestacional de bajo riesgo
El tratamiento de la neoplasia trofoblástica gestacional (NTG) de bajo riesgo ( mola invasiva o coriocarcinoma ) puede incluir lo siguiente:
- Quimioterapia con uno o más medicamentos contra el cáncer. El tratamiento se administra hasta que el nivel de gonadotropina coriónica humana beta (beta-hCG) se normalice durante al menos 3 semanas después de finalizar el tratamiento.
Si el nivel de beta-hCG en la sangre no vuelve a la normalidad o el tumor se propaga a partes distantes del cuerpo, se administran regímenes de quimioterapia utilizados para el GTN metastásico de alto riesgo.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Neoplasia trofoblástica gestacional metastásica de alto riesgo
El tratamiento de la neoplasia trofoblástica gestacional metastásica de alto riesgo ( mola invasiva o coriocarcinoma ) puede incluir lo siguiente:
- Quimioterapia combinada.
- Quimioterapia intratecal y radioterapia dirigida al cerebro (para el cáncer que se ha propagado al pulmón, para evitar que se propague al cerebro).
- Quimioterapia en dosis altas o quimioterapia intratecal y/o radioterapia al cerebro (para el cáncer que se ha diseminado al cerebro).
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Tumores trofoblásticos gestacionales del sitio placentario y tumores trofoblásticos epitelioides
El tratamiento de los tumores trofoblásticos gestacionales del sitio placentario en estadio I y de los tumores trofoblásticos epitelioides puede incluir lo siguiente:
El tratamiento de los tumores trofoblásticos gestacionales del sitio placentario y de los tumores trofoblásticos epitelioides en estadio II puede consistir en:
- Cirugía para extirpar el tumor, que puede ir seguida de quimioterapia combinada .
El tratamiento de los tumores trofoblásticos gestacionales del sitio placentario y de los tumores trofoblásticos epitelioides en estadios III y IV puede consistir en:
- Quimioterapia combinada
- Cirugía para extirpar el cáncer que se ha propagado a otras partes, como el pulmón o el abdomen .
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Neoplasia trofoblástica gestacional recidivante o resistente
El tratamiento del tumor trofoblástico gestacional recurrente o resistente puede incluir lo siguiente:
- Quimioterapia con uno o más medicamentos anticancerígenos para tumores tratados previamente con cirugía .
- Quimioterapia combinada para tumores tratados previamente con quimioterapia.
- Cirugía para tumores que no responden a la quimioterapia.
Puede utilizar la búsqueda de ensayos clínicos y encontrar ensayos clínicos sobre cáncer patrocinados por el NCI que acepten participantes. La búsqueda le permite filtrar los ensayos según el tipo de cáncer, la edad y el lugar donde se realizan los ensayos. También encontrará información general sobre los ensayos clínicos.
Más información sobre la enfermedad trofoblástica gestacional
Para obtener más información del National Cancer Institute sobre tumores y neoplasias trofoblásticas gestacionales, consulte lo siguiente:
- Página de inicio de la enfermedad trofoblástica gestacional
- Medicamentos aprobados para la enfermedad trofoblástica gestacional
- Cáncer metastásico
For general cancer information and other resources from the National Cancer Institute, visit:
Sobre este resumen del PDQ
Acerca del PDQ
El Physician Data Query (PDQ) es la base de datos integral sobre el cáncer del National Cancer Institute (NCI). La base de datos del PDQ contiene resúmenes con la última información publicada sobre prevención, detección, genética, tratamiento, atención médica de apoyo y medicina complementaria y alternativa relacionada con el cáncer. La mayoría de los resúmenes se presentan en dos versiones. Las versiones para profesionales de la salud contienen información detallada escrita en lenguaje técnico. Las versiones para pacientes están escritas en un lenguaje fácil de entender y no tan técnico. Ambas versiones contienen información precisa y actualizada sobre el cáncer. La mayoría de las versiones también están disponibles en español.
El PDQ es un servicio del NCI. El NCI es parte de los Institutos Nacionales de Salud (NIH), que son el centro de investigación biomédica del Gobierno federal. Los resúmenes del PDQ se basan en una revisión independiente de la literatura médica. No son declaraciones de políticas del NCI ni de los NIH.
Propósito de este resumen
Este resumen sobre el cáncer del PDQ contiene información actualizada sobre el tratamiento de la enfermedad trofoblástica gestacional. Su propósito es informar y ayudar a pacientes, familias y cuidadores. No da pautas ni recomendaciones formales para la toma de decisiones sobre la atención médica.
Revisores y actualizaciones
Los comités editoriales escriben los resúmenes de información sobre el cáncer del PDQ y los mantienen actualizados. Estos comités están formados por equipos de especialistas en el tratamiento del cáncer y otras especialidades relacionadas con esta enfermedad. Los resúmenes se revisan periódicamente y se modifican cuando hay información nueva. La fecha de actualización al pie de cada resumen indica cuándo se realizó el cambio más reciente.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Adult Treatment Editorial Board.
Información sobre ensayos clínicos
Un ensayo clínico es un estudio para responder a una pregunta científica como, por ejemplo, si un tratamiento es mejor que otro. Los ensayos se basan en estudios anteriores y en lo aprendido en el laboratorio. Cada ensayo responde a determinadas preguntas científicas que permiten encontrar nuevas y mejores formas de ayudar a los pacientes con cáncer. Durante los ensayos clínicos de tratamiento, se recopila información sobre los efectos de un nuevo tratamiento y su eficacia. Si un ensayo clínico demuestra que un nuevo tratamiento es mejor que uno que se utiliza actualmente, el nuevo tratamiento puede convertirse en “estándar”. Los pacientes pueden valorar la posibilidad de participar en un ensayo clínico. Algunos ensayos clínicos solo están abiertos a pacientes que no hayan iniciado el tratamiento.
Los ensayos clínicos se pueden encontrar en línea en el sitio web del NCI. Para obtener más información, llame al Servicio de Información sobre el Cáncer (CIS, por sus siglas en inglés), el centro de contacto del NCI, al 1-800-4-CANCER (1-800-422-6237).
Permiso de uso de este resumen
Physician Data Query (PDQ) es una marca registrada. Se autoriza el libre uso del contenido de los documentos del PDQ como texto. Sin embargo, no se podrá identificar como un resumen de información sobre cáncer del PDQ del NCI, salvo que se reproduzca en su totalidad y se actualice con regularidad. Por otra parte, se permite que los autores incluyan una oración como “en el resumen del PDQ del NCI sobre la prevención del cáncer de mama se describen, de manera concisa, los siguientes riesgos: [incluir fragmento del resumen]”.
La forma recomendada para citar este resumen del PDQ es:
Comité editorial del PDQ® sobre el tratamiento para adultos. Tratamiento de la enfermedad trofoblástica gestacional (PDQ). Bethesda, MD: National Cancer Institute. Actualizado el [DD/MM/AAAA]
Las imágenes de este resumen se utilizan con el permiso del autor, artista y/o editorial para uso exclusivo en los resúmenes del PDQ. Si desea usar una imagen de un resumen del PDQ sin incluir el resumen completo, debe obtener autorización del propietario. El National Cancer Institute no puede otorgar dicho permiso. Para obtener más información sobre el uso de las imágenes de este resumen o de otras ilustraciones relacionadas con el cáncer, consulte Visuals Online, una colección de más de 3,000 imágenes científicas.
Descargo de responsabilidad
La información de estos resúmenes no debe utilizarse para tomar decisiones sobre reembolsos de seguros. Puede encontrar más información sobre la cobertura de seguros en Cancer.gov en el sitio Manejo de la atención del cáncer.
Contáctenos
Puede encontrar más información sobre cómo contactarnos o recibir ayuda en el sitio web Cancer.gov en la página Comuníquese con el NCI. También puede enviar sus preguntas a Cancer.gov en el apartado Escríbanos del sitio web.
Actualizado:
URL de origen: https://www.cancer.gov/node/551323/syndication
Agencia de origen: National Cancer Institute (NCI)
Fecha de captura: 14/09/2013 09:06:23.0