Video could not be played

Video could not be played

Video could not be played
News Releases
-

Video could not be played
-
Video could not be played
-
Video could not be played
News Release
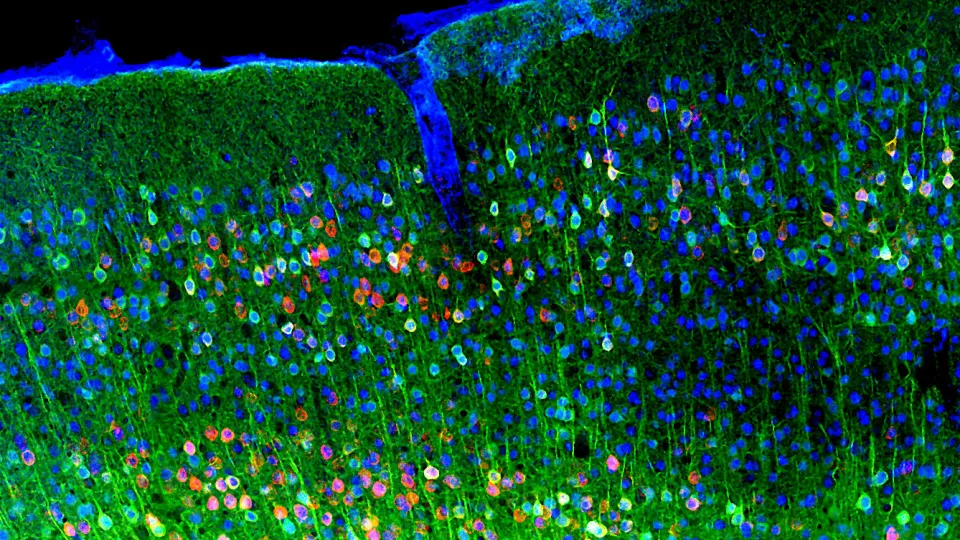
New Probes Reveal Proteins Inside Living Cells with Unprecedented Clarity
April 22, 2026
In the News
Header
Experts for Media
Header
Experts for Media

Video could not be played

Video could not be played

Video could not be played

Video could not be played

Video could not be played
Research



Education & Training