
Video could not be played
Feature
To Prevent Loss of Limbs Related to Diabetes, a New Team Approach
September 19, 2025

Video could not be played
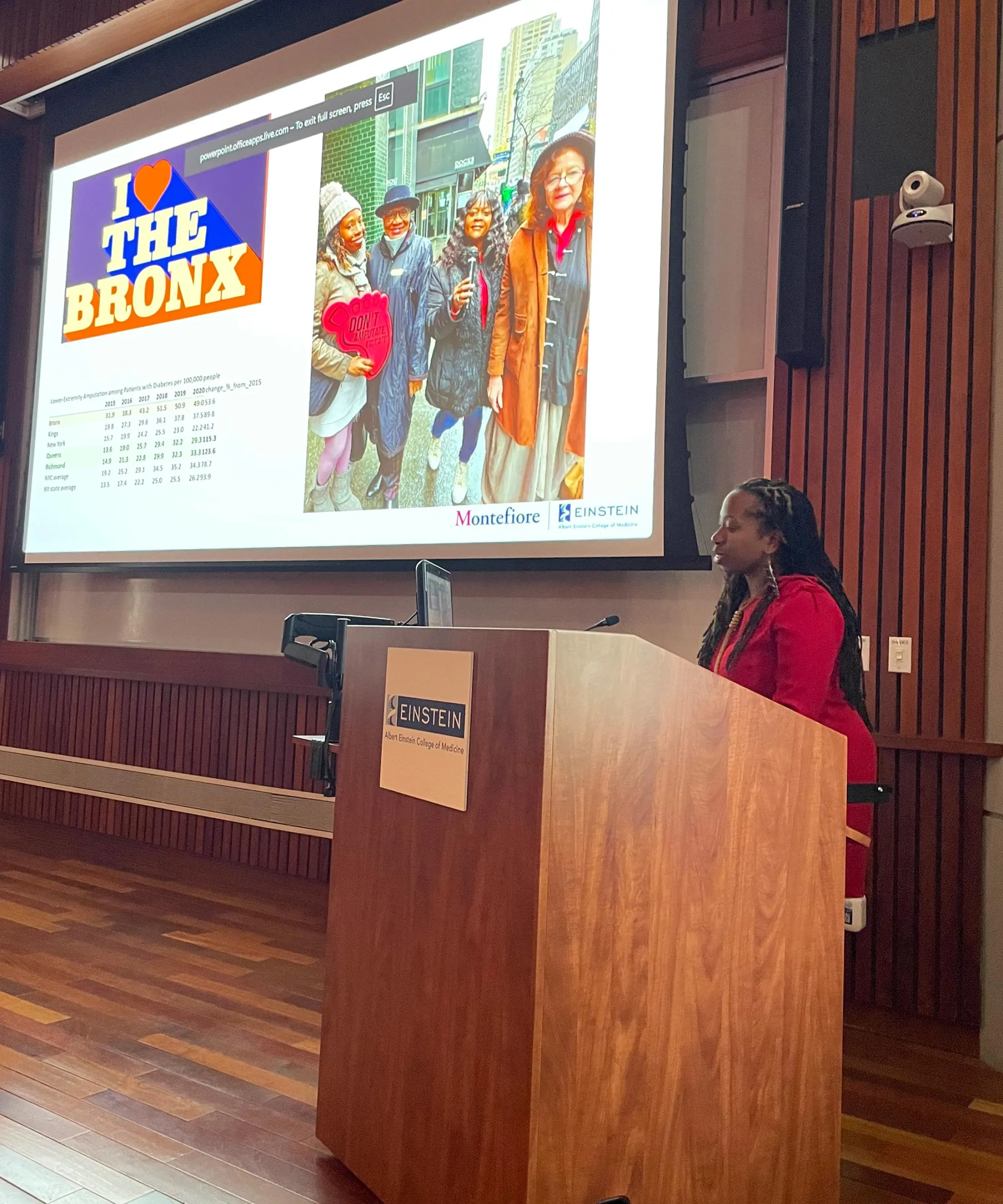
From left, guest speaker Dr. Foluso Fakorede at an event in September, with Dr. Alyson Myers; Dr. Jairo Arce-Morales; Dr. Gisette Reyes-Soffer, cardiologist at Columbia University; Dr. Johanna Daily; and Dr. Denise Levy.
About a third of people with diabetes will develop an ulcer, or open sore, on their foot. Uncontrolled blood sugar damages nerves and vasculature, which can lead to foot deformities and increased pressure on weight bearing parts of the foot, creating inflammation and callouses, and then sores. Foot ulcers affect an estimated 1.6 million people in the U.S. annually.By the time many diabetic patients find out they have an ulcer, it may already be too late. “Many patients with diabetes also have neuropathy, which causes loss of protective sensation,” explains Denise Levy, DPM, a surgically trained podiatrist at Montefiore Einstein. “Pain in this case is actually a gift,” she explains—it warns the patient that something is wrong and should prompt them to seek timely care.
Video could not be played
Endocrinologist and co-founder of the multidisciplinary clinic Dr. Alyson Myers presents at the event the clinic organized in recognition of Peripheral Arterial Disease Awareness Month in September.
Because diabetes can cause peripheral arterial disease, leading to poor blood flow in the feet, once an ulcer becomes infected—which can happen rapidly—it may be very hard for it to heal. In a matter of days, an infection that goes untreated can cause tissue damage that necessitates an amputation. “People wait too long,” says Johanna Daily, MD, MS, infectious disease physician in the Department of Medicine. “I tell my patients with diabetes to check their feet every day, and the moment you have anything going on, we cannot wait. It's like a stroke—the clock is ticking and the faster you can get treatment, the better the outcome.”
In addition to the catastrophic loss an amputation represents in the near term, it also drastically reduces a person’s chances of a long, healthy, and fulfilling life. “It becomes a major disability,” says Dr. Daily. “There's about a 50 percent mortality rate at five years. It's worse than cancer.”
A new approach
It’s not surprising then that in order to help prevent diabetic foot ulcers and keep them from progressing, physicians at a few leading institutions around the country are using a treatment model associated with cancer—multidisciplinary comprehensive care centers, where patients can see all the providers who have a role in shaping their care in one place and often, at the same time.
Last spring, Montefiore Einstein joined their ranks, launching a monthly Multidisciplinary Diabetic Foot Ulcer Clinic. One Friday morning a month at Montefiore’s Hutchinson campus at Waters Place, in addition to Dr. Levy and Dr. Daily, patients can see endocrinologist Alyson Myers, MD; vascular surgeon Manasa Kanneganti, MD; behavioral health specialist Jairo Arce-Morales, PhD; and Isatou Dukuray, NP, who specializes in wound care.
“Foot ulcers are an endocrine issue, for control of blood sugar,” says Dr. Daily. “It is a vascular issue. It often ends up being an infectious issue when an ulcer forms. There's definitely a need for behavioral health, because many people get diabetes distress. You need a nutritionist. And so we pitched this multidisciplinary clinic to Montefiore.” After more than a year of planning, the clinic launched in March of 2025. So far, it’s been a huge success, based on how the care team feels about what this model enables them to provide for patients, and in the outcomes they are seeing.
Since the clinic launched last spring, Dr. Levy has noticed a perceptible difference. “Patients are satisfied, their levels of distress are lower, and they feel more comfortable and safe in a system that understands how to address all their needs,” she says. “It's similar to the multifaceted, integrative care that oncology patients receive—the central focus, to improve quality of life.”
“We can all build on each other's thoughts, come up with a comprehensive treatment plan, and reinforce to the patient the importance follow-through,” says Dr. Kanneganti.
Dr. Daily adds, “The literature shows that multidisciplinary teams have better outcomes. There is less loss of limb.” The approach is also simply easier for patients. “We try to take care of all their issues in one setting,” she says. “It’s especially hard for them to come to many different doctors because of their disability, and often, their lack of resources.”
A national crisis
Rates of diabetes-related amputation—of toes, the lower leg, or sometimes, above the knee—are higher in the Bronx than the national average. “Risk factors for having diabetic foot ulcers leading to amputation are typically if you're a member of a non-white race,” says Dr. Myers. “It’s more common in Black, Hispanic, and Latino patients, which is also our population in the Bronx.” She adds that low socioeconomic status and lack of commercial insurance are also risk factors, and rates are also higher in men, who may be less likely than women to seek out care for both routine and urgent health issues.
Dr. Daily adds that in studies done around the U.S., “You can take the zip codes, know what the average household salary is, and you can correlate that to the risk of lower extremity amputation. In other words, if you are resource limited, you are more likely to lose your leg.” In the Bronx, many of these patients are also surprisingly young.
Before the clinic launched, the team conducted research to assess the scope of the problem locally. They applied for and received funding from the American Diabetes Association and the Center for Diabetes Translational Research here at Montefiore Einstein. They worked with residents and fellows on a chart review from the past 10 years and found that patients who came to the hospital here and were diagnosed with a diabetic foot ulcer had a 44 percent chance of receiving an amputation. “We were pretty devastated, because it's almost a one-in-two chance,” Dr. Myers says.
They also found that a few places around the country, including the University of Chicago and Stanford, have multidisciplinary clinics focused on early treatment of vascular problems and limb preservation. “Vascular surgeons can go in and either balloon a narrow vessel or bypass that vessel with stenting to try to improve the outcomes for people,” explains Dr. Myers. Once blood flow is improved, if someone does get an ulcer, it helps antibiotics to get to the site and allows for better healing.
Dr. Myers and Dr. Daily in the Department of Medicine were the first collaborators on board. They joined forces with Dr. Levy, an expert in diabetic limb salvage and limb preservation, and Dr. Kanneganti, who has a strong clinical interest in this area. “Arterial disease and limb salvage are what drew me to vascular surgery,” she says. “Walking is such a huge part of people’s quality of life, so I want to do everything we can to preserve that ability for our patients.”
Dr. Levy concurs. “When caring for the whole patient, we must consider what limb loss means beyond the physical: the potential loss of livelihood, the threat to independence, and the impact on dignity within the family structure.”
This is among the reasons Dr. Levy feels shifting from a reactive approach to a proactive one is so critical. And this is exactly what the new clinic is allowing doctors at Montefiore Einstein to do.
On the horizon
Technology is giving physicians new tools to prevent foot ulcers before they occur. The clinic team recently did a pilot study, led by Dr. Levy, in which patients were provided with a smart mat that is used once a day from the comfort of their home. The mat utilizes thermal imaging to sense the differences between areas of the plantar foot that signal inflammation or injury, a precursor to ulcer formation, and alerts clinicians remotely.
“The patient steps on the mat for 20 seconds a day, and the data is transmitted automatically to a monitoring service,” says Dr. Levy. “Care teams are alerted if concerning changes are detected, so they can intervene early with advice to offload or seek timely care from their provider.” She continues, “Research shows that identifying hot spots can predict formation of ulcers weeks before they occur. Catching these problems early reduces the risk of severe infections and amputation."
Out of 20 patients using the mat, only two developed ulcers, versus approximately 33 percent of diabetes patients nationally who develop ulcers. “Patients may still get an ulcer, but now we’ll catch it at stage 1, when it’s more treatable, instead of stage 4,” says Dr. Daily. However this and other preventive innovations are not yet covered by insurance. “We are compelled to document and advance this research to improve patient outcomes,” says Dr. Levy. “Sustainable impact requires insurers at the state and local levels to recognize the value of investing in the comprehensive care of this fragile, underserved population.”
Proper footwear is something else patients at the clinic have access to, via a provider of custom orthotic inserts and special shoes that offload pressure. Dr. Myers and the clinic team have found a partner in Josh White, DPM, vice president of Orthofeet, who comes to the clinic to fit patients.
Even after an amputation occurs, in addition to the work of adapting, patients still face significant risks of recurrence of ulcers, and with them, a second amputation. “The rate of remission for diabetic foot ulcers in the same limb on different anatomic locations is about 82 to 87 percent, while on the contralateral limb it's 42 percent,” says Dr. Levy. “Based on that data alone, we must invest in prevention rather than reactionary care.”
There are also systemic costs to take into account. “Hospital readmission rates for patients with diabetic foot ulcers are around 20 percent,” says Dr. Myers. Reducing readmissions for all patients who are hospitalized is a key national healthcare quality metric. “Keeping these patients out of the hospital benefits us as a health system,” Dr. Myers continues. “The clinic is helping defray costs, but more importantly, it’s improving patients’ quality of life. No one likes being in the hospital.”
Some of the next key steps include tracking how patients at the clinic fare over time, and finding ways to identify high-risk patients and get them there. The team hopes that as they are able to show strong outcomes in preventing amputations and keeping patients out of the hospital, support for the clinic will grow, and they’ll be able to expand its hours.
“It's about the human factor,” says Dr. Levy. “Trust in care matters: the patients who joined us at the launch of our multidisciplinary clinic trust the care they are receiving, and that trust is reflected in their continued engagement and return visits. We are currently experiencing the results of that.”